

Low-Cost Predictors for Liver Function and Clinical Outcomes after Sustained Virological Response in Patients with HCV-Related Cirrhosis and Thrombocytopenia

Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
2.3. Variables Collected
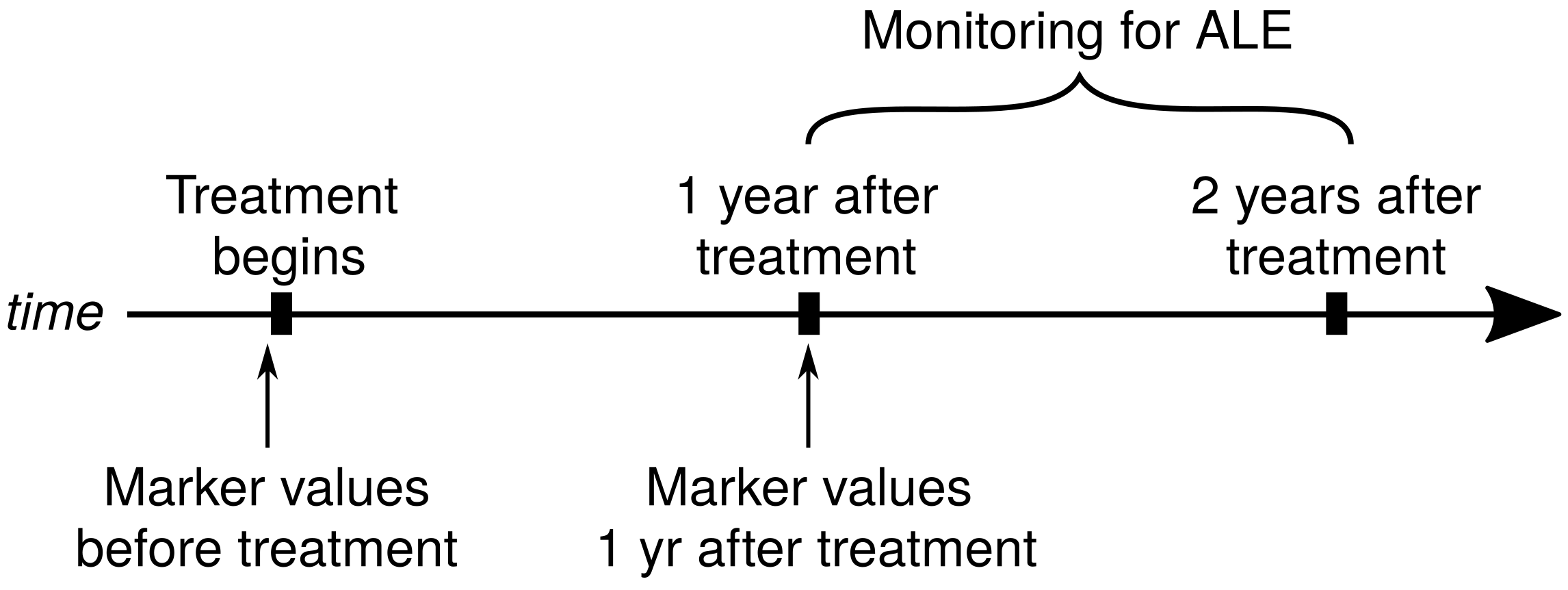
2.4. Timeline
- (a) Before treatment;
- (b) At the one-year follow-up visit;
- (c) For the dynamics of markers, we also calculated their changes in time (defined as: the value at 1 year − value before treatment), for each variable.
2.5. Software and Calculation
3. Results
3.1. Overall Group Evolution
3.1.1. Platelets and Leukocyte Count, Haemoglobin, Serum Albumin—Evolution in Time
3.1.2. APRI, MELD and FIB-4 Scores—Evolution in Time
3.2. Adverse Liver Events
- The presence or absence of adverse liver effects (both HCC and ascites/GI bleeding);
- Only the presence/absence of HCC;
- Only the presence/absence of ascites/GI bleeding.
3.2.1. Identified Concerning Factors for Adverse Liver Events (Both HCC and Ascites/Bleeding)
- FIB-4 score at 1 year (Figure 4a)For one unit increase in the FIB-4 score at 1 year the overall odds ratio (OR) of developing adverse liver events (vs. not developing) increased by a factor of 1.65;
- An AFP increase after 1 year (Figure 4b)The AFP change (as defined in Methods, Section 2.4) is the AFP value at 1 year − AFP value at the beginning. For a unit increase in the AFP change, the OR increased by a factor of 1.0;
- MELD score at 1 year (Figure 4c);For a unit increase in the MELD score, the OR increased by a factor of 2.26.
3.2.2. Identified Concerning Factor for Hepatocellular Carcinoma
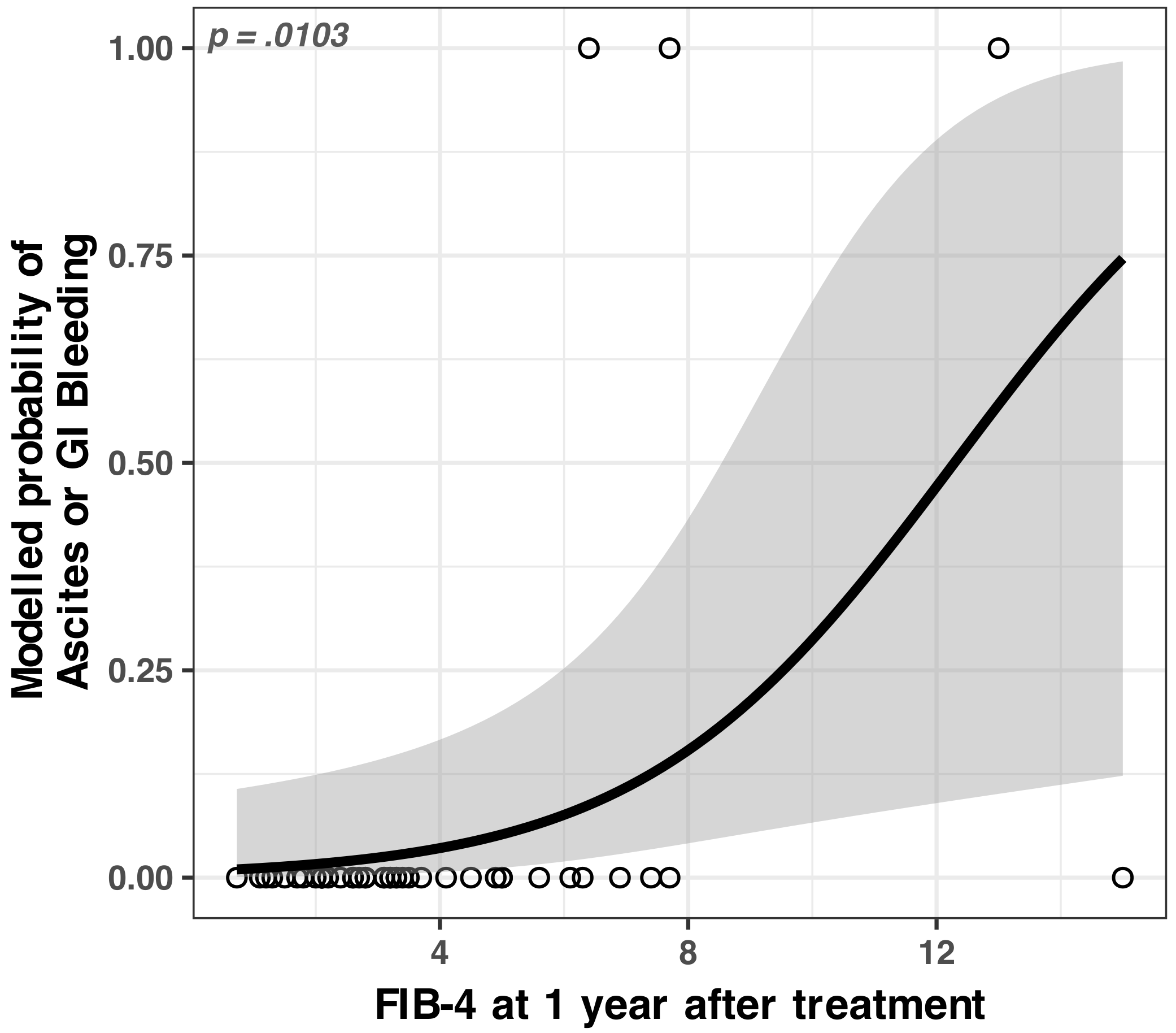
3.2.3. Identified Concerning Factor for Ascites/GI Bleeding
4. Discussion
4.1. General Improvement after Therapy
4.1.1. Haematological Improvements
4.1.2. Hepatic Function Improvements
4.2. Rare Adverse Liver Events
4.2.1. Identified Concerning Factors for Adverse Liver Events (Both HCC and Ascites/Bleeding)
4.2.2. Identified Concerning Factors for Hepatocellular Carcinoma
4.2.3. Identified Concerning Factors for Ascites/GI Bleeding
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AIC | Akaike Information Criterion |
| APRI | AST to Platelet Ratio Index score |
| AST | Aspartate aminotransferase |
| CHILD | Child–Pugh Score for Cirrhosis Mortality |
| CI | Confidence interval |
| DAA | Direct-acting antivirals |
| FIB-4 | Fibrosis-4 Index for Liver Fibrosis score |
| GI | Gastrointestinal |
| HBV | Hepatitis B virus |
| HCC | Hepatocellular carcinoma |
| HCV | Hepatitis C virus |
| HCV–RNA | Hepatitis C virus ribonucleic acid |
| INR | International normalized ratio |
| IQR | Interquartile range |
| MELD | Model for End-Stage Liver Disease score |
| OR | Odds Ratio |
| SVR | Sustained virological response |
| TCP | Thrombocytopenia |
Appendix A. Statistics
Appendix A.1. Statistics of Serum Markers
- Average values of blood platelet count increased with an average of 22,600/µL (Wilcoxon signed-rank test with continuity correction, Z = 4.61, p < 0.001).
- The leukocyte count increased with an average of 1102/µL (Wilcoxon signed-rank test with continuity correction, Z = 4.31, p < 0.001).
- Haemoglobinemia increased with an average 0.65 mg/dL (Welch t-test, t(45) = 2.934, p < 0.003).
- Albuminemia increased with an average of 0.29 g/dL (Wilcoxon signed-rank test with continuity correction, Z = 4.09, p < 0.001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Before Treatment, N = 46 1 | 1 Year, N = 46 1 |
|---|---|---|
| Platelet count/µL | 98,722 (32,220) | 121,348 (55,928) |
| Leucocytes/µL | 4826 (1889) | 5928 (2055) |
| Hb mg/dL | 13.08 (2.35) | 13.73 (1.96) |
| Serum albumin g/dL | 4.13 (0.44) | 4.41 (0.55) |
Appendix A.2. Statistics of Liver Scores
- APRI had a significant decrease (Wilcoxon signed-rank test with continuity correction, Z = −5.81, p < 0.001);
- FIB-4 score had a significant decrease (Wilcoxon signed-rank test with continuity correction, Z = 5.56, p < 0.001).
| Characteristic | Before Treatment, N = 46 1 | 1 Year, N = 46 1 |
|---|---|---|
| APRI Score | 1.90 (1.30, 3.20) | 0.52 (0.38, 0.94) |
| MELD Score | 8.00 (7.00, 10.00) | 8.00 (7.00, 9.00) |
| FIB-4 Score | 5.4 (3.9, 9.7) | 3.2 (2.1, 5.0) |
Appendix A.3. Statistical Modelling
| Characteristic | OR 1 | 95% CI 1 | p-Value 2 |
|---|---|---|---|
| (Intercept) | 0.0000 | 0.0000, 0.0877 | 0.0212 |
| FIB-4 at 1 year | 1.6549 | 1.1814, 2.8482 | 0.0029 |
| AFP change after 1 year | 1.0077 | 1.0027, 1.0233 | 0.0025 |
| MELD at 1 year | 2.2616 | 1.1149, 6.8938 | 0.0223 |
| Serum albumin, before treatment | 3.3884 | 0.2711, 253.1818 | 0.3793 * |
| Platelet count at 1 year | 1.0000 | 0.9999, 1.0000 | 0.0927 * |
| Characteristic | OR 1 | 95% CI 1 | p-Value 2 |
|---|---|---|---|
| (Intercept) | 2.3603 | 0.0747, 87.5143 | 0.6214 * |
| Leucocyte count at 1 year | 0.9994 | 0.9985, 1.0000 | 0.07505 * |
| Characteristic | OR1 | 95% CI 1 | p-Value 2 |
|---|---|---|---|
| (Intercept) | 0.0133 | 0.0007, 0.0863 | <0.001 |
| FIB-4 at 1 year | 1.4049 | 1.0866, 1.9716 | 0.0103 |
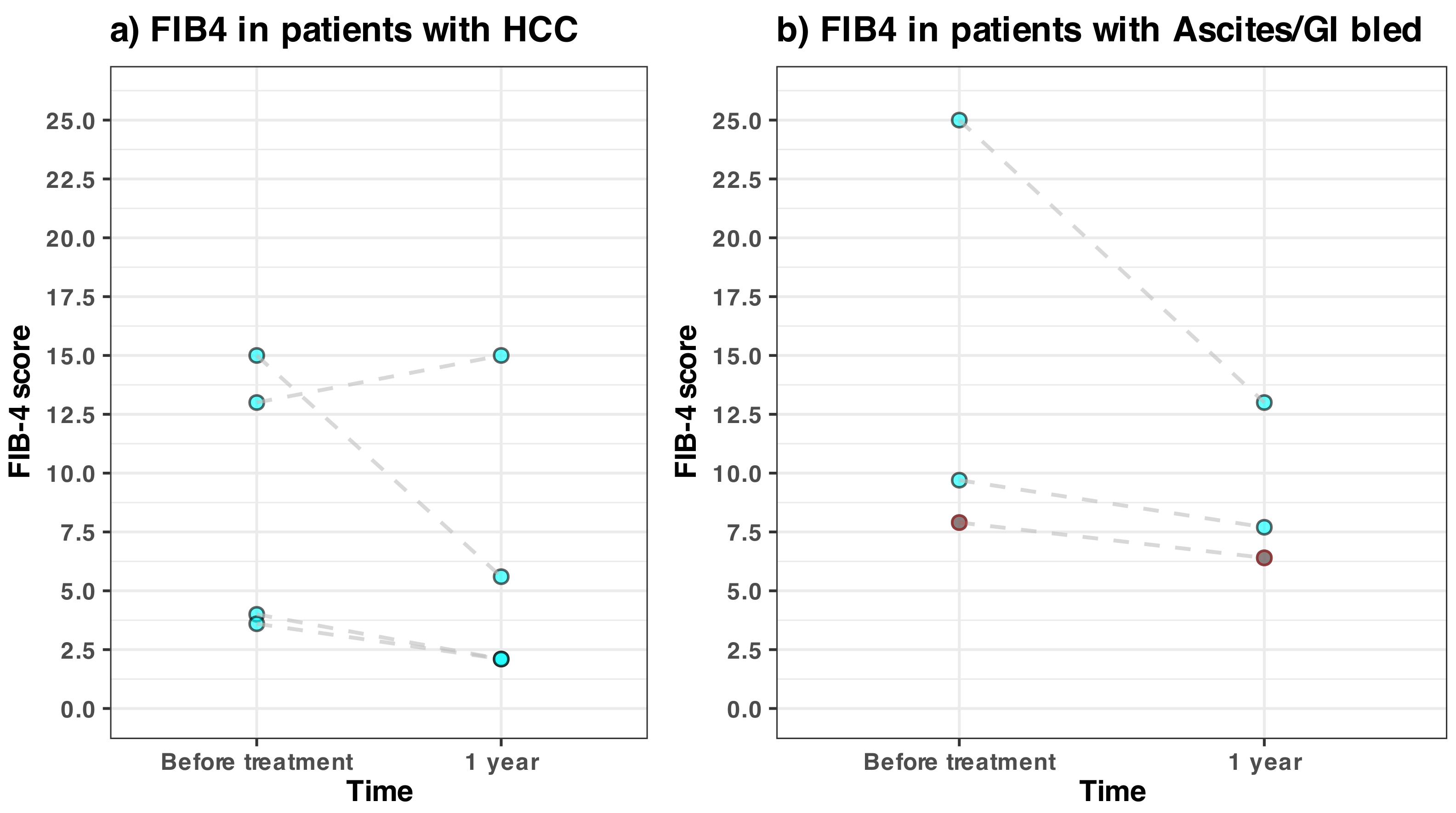
Appendix A.4. FIB-4 Details in Patients with Adverse Liver Effects

References
- Polaris Observatory HCV Collaborators. Global Prevalence and Genotype Distribution of Hepatitis C Virus Infection in 2015: A Modelling Study. Lancet. Gastroenterol. Hepatol. 2017, 2, 161–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velosa, J. Why Is Viral Eradication so Important in Patients with HCV-related Cirrhosis? Antivir. Ther. 2017, 22, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Chopra, S.; Clinical Manifestations and Natural History of Chronic Hepatitis C Virus Infection. UpToDate, Wolters Kluwer (Ed. Di Bisceglie A.M. and Bloom A.). 2022. Available online: https://www.uptodate.com/contents/clinical-manifestations-and-natural-history-of-chronic-hepatitis-c-virus-infection (accessed on 31 December 2022).
- Rawi, S.; Wu, G.Y. Pathogenesis of Thrombocytopenia in Chronic HCV Infection: A Review. J. Clin. Transl. Hepatol. 2020, 8, 184–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Intagliata, N.; Shah, N.L. Hemostatic Abnormalities in Patients with Liver Disease. UpToDate, Wolters Kluwer (Ed. Leung L.L.K. and Tirnauer J.S.). 2022. Available online: https://www.uptodate.com/contents/hemostatic-abnormalities-in-patients-with-liver-disease (accessed on 31 December 2022).
- Louie, K.S.; Micallef, J.M.; Pimenta, J.M.; Forssen, U.M. Prevalence of thrombocytopenia among patients with chronic hepatitis C: A systematic review. J. Viral Hepat. 2010, 18, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kozbial, K.; Moser, S.; Al-Zoairy, R.; Schwarzer, R.; Datz, C.; Stauber, R.; Laferl, H.; Strasser, M.; Beinhardt, S.; Stättermayer, A.F.; et al. Follow-up of Sustained Virological Responders with Hepatitis C and Advanced Liver Disease after Interferon/Ribavirin-Free Treatment. Liver Int. Off. J. Int. Assoc. Study Liver 2018, 38, 1028–1035. [Google Scholar] [CrossRef] [PubMed]
- Veldt, B.J.; Heathcote, E.J.; Wedemeyer, H.; Reichen, J.; Hofmann, W.P.; Zeuzem, S.; Manns, M.P.; Hansen, B.E.; Schalm, S.W.; Janssen, H.L.A. Sustained Virologic Response and Clinical Outcomes in Patients with Chronic Hepatitis C and Advanced Fibrosis. Ann. Intern. Med. 2007, 147, 677–684. [Google Scholar] [CrossRef] [Green Version]
- Van der Meer, A.J.; Veldt, B.J.; Feld, J.J.; Wedemeyer, H.; Dufour, J.F.; Lammert, F.; Duarte-Rojo, A.; Heathcote, E.J.; Manns, M.P.; Kuske, L.; et al. Association between Sustained Virological Response and All-Cause Mortality among Patients with Chronic Hepatitis C and Advanced Hepatic Fibrosis. JAMA 2012, 308, 2584–2593. [Google Scholar] [CrossRef]
- European Association for Study of Liver. EASL Recommendations on Treatment of Hepatitis C 2015. J. Hepatol. 2015, 63, 199–236. [Google Scholar] [CrossRef] [Green Version]
- Ghany, M.G.; Morgan, T.R.; AASLD-IDSA Hepatitis C Guidance Panel. Hepatitis C Guidance 2019 Update: American Association for the Study of Liver Diseases–Infectious Diseases Society of America Recommendations for Testing, Managing, and Treating Hepatitis C Virus Infection. Hepatology 2020, 71, 686–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tachi, Y.; Hirai, T.; Miyata, A.; Ohara, K.; Iida, T.; Ishizu, Y.; Honda, T.; Kuzuya, T.; Hayashi, K.; Ishigami, M.; et al. Progressive Fibrosis Significantly Correlates with Hepatocellular Carcinoma in Patients with a Sustained Virological Response. Hepatol. Res. Off. J. Jpn. Soc. Hepatol. 2015, 45, 238–246. [Google Scholar] [CrossRef]
- Poynard, T.; Moussalli, J.; Munteanu, M.; Thabut, D.; Lebray, P.; Rudler, M.; Ngo, Y.; Thibault, V.; Mkada, H.; Charlotte, F.; et al. Slow Regression of Liver Fibrosis Presumed by Repeated Biomarkers after Virological Cure in Patients with Chronic Hepatitis C. J. Hepatol. 2013, 59, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Mandorfer, M.; Kozbial, K.; Schwabl, P.; Freissmuth, C.; Schwarzer, R.; Stern, R.; Chromy, D.; Stättermayer, A.F.; Reiberger, T.; Beinhardt, S.; et al. Sustained Virologic Response to Interferon-Free Therapies Ameliorates HCV-induced Portal Hypertension. J. Hepatol. 2016, 65, 692–699. [Google Scholar] [CrossRef] [PubMed]
- Knop, V.; Hoppe, D.; Welzel, T.; Vermehren, J.; Herrmann, E.; Vermehren, A.; Friedrich-Rust, M.; Sarrazin, C.; Zeuzem, S.; Welker, M.W. Regression of Fibrosis and Portal Hypertension in HCV-associated Cirrhosis and Sustained Virologic Response after Interferon-Free Antiviral Therapy. J. Viral Hepat. 2016, 23, 994–1002. [Google Scholar] [CrossRef] [PubMed]
- Chekuri, S.; Nickerson, J.; Bichoupan, K.; Sefcik, R.; Doobay, K.; Chang, S.; DelBello, D.; Harty, A.; Dieterich, D.T.; Perumalswami, P.V.; et al. Liver Stiffness Decreases Rapidly in Response to Successful Hepatitis C Treatment and Then Plateaus. PLoS ONE 2016, 11, e0159413. [Google Scholar] [CrossRef] [Green Version]
- Pockros, P.; Crissien-Martinez, A.; Frenette, C.; Skillin, C.; Bao, F.; Du, E.; Pan, J.; Waalen, J. Degree of Liver Fibrosis Regression Predicted by Transient Elastography after Cure of Chronic Hepatitis C with Direct Acting Antivirals Is Overestimated but Confirmed by Liver Biopsy. J. Hepatol. 2017, 66, S108. [Google Scholar] [CrossRef]
- ANRS CO13 HEPAVIH Cohort. Regression of Liver Stiffness after Sustained Hepatitis C Virus (HCV) Virological Responses among HIV/HCV-coinfected Patients. AIDS 2015, 29, 1821–1830. [Google Scholar] [CrossRef] [PubMed]
- Cheung, M.C.M.; Walker, A.J.; Hudson, B.E.; Verma, S.; McLauchlan, J.; Mutimer, D.J.; Brown, A.; Gelson, W.T.H.; MacDonald, D.C.; Agarwal, K.; et al. Outcomes after Successful Direct-Acting Antiviral Therapy for Patients with Chronic Hepatitis C and Decompensated Cirrhosis. J. Hepatol. 2016, 65, 741–747. [Google Scholar] [CrossRef] [Green Version]
- Pascasio, J.M.; Vinaixa, C.; Ferrer, M.T.; Colmenero, J.; Rubin, A.; Castells, L.; Manzano, M.L.; Lorente, S.; Testillano, M.; Xiol, X.; et al. Clinical Outcomes of Patients Undergoing Antiviral Therapy While Awaiting Liver Transplantation. J. Hepatol. 2017, 67, 1168–1176. [Google Scholar] [CrossRef]
- Krassenburg, L.A.P.; Maan, R.; Ramji, A.; Manns, M.P.; Cornberg, M.; Wedemeyer, H.; de Knegt, R.J.; Hansen, B.E.; Janssen, H.L.A.; de Man, R.A.; et al. Clinical Outcomes Following DAA Therapy in Patients with HCV-related Cirrhosis Depend on Disease Severity. J. Hepatol. 2021, 74, 1053–1063. [Google Scholar] [CrossRef]
- Pugh, R.N.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the Oesophagus for Bleeding Oesophageal Varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. 2020. Available online: https://www.r-project.org/ (accessed on 18 May 2021).
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the Tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef] [Green Version]
- Heinze, G.; Ploner, M.; Jiricka, L. Logistf: Firth’s Bias-Reduced Logistic Regression. R Package Manual Version 1.24. 2020. Available online: https://cran.r-project.org/package=logistf (accessed on 18 January 2021).
- Firth, D. Bias Reduction of Maximum Likelihood Estimates. Biometrika 1993, 80, 27–38. [Google Scholar] [CrossRef]
- Venables, V.N.; Ripley, B.D. Modern Applied Statistics with S, 4th ed.; Springer: New York, NY, USA, 2002. [Google Scholar]
- Lu, M.; Li, J.; Zhang, T.; Rupp, L.B.; Trudeau, S.; Holmberg, S.D.; Moorman, A.C.; Spradling, P.R.; Teshale, E.H.; Xu, F.; et al. Serum Biomarkers Indicate Long-term Reduction in Liver Fibrosis in Patients With Sustained Virological Response to Treatment for HCV Infection. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2016, 14, 1044–1055.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Ambrosio, R.; Aghemo, A.; Rumi, M.G.; Ronchi, G.; Donato, M.F.; Paradis, V.; Colombo, M.; Bedossa, P. A Morphometric and Immunohistochemical Study to Assess the Benefit of a Sustained Virological Response in Hepatitis C Virus Patients with Cirrhosis. Hepatology 2012, 56, 532–543. [Google Scholar] [CrossRef]
- D’Ambrosio, R.; Degasperi, E.; Aghemo, A.; Fraquelli, M.; Lampertico, P.; Rumi, M.G.; Facchetti, F.; Grassi, E.; Casazza, G.; Rosenberg, W.; et al. Serological Tests Do Not Predict Residual Fibrosis in Hepatitis C Cirrhotics with a Sustained Virological Response to Interferon. PLoS ONE 2016, 11, e0155967. [Google Scholar] [CrossRef]
- Belli, L.S.; Berenguer, M.; Cortesi, P.A.; Strazzabosco, M.; Rockenschaub, S.R.; Martini, S.; Morelli, C.; Donato, F.; Volpes, R.; Pageaux, G.P.; et al. Delisting of Liver Transplant Candidates with Chronic Hepatitis C after Viral Eradication: A European Study. J. Hepatol. 2016, 65, 524–531. [Google Scholar] [CrossRef]
- Perricone, G.; Duvoux, C.; Berenguer, M.; Cortesi, P.A.; Vinaixa, C.; Facchetti, R.; Mazzarelli, C.; Rockenschaub, S.R.; Martini, S.; Morelli, C.; et al. Delisting HCV-infected Liver Transplant Candidates Who Improved after Viral Eradication: Outcome 2 Years after Delisting. Liver Int. Off. J. Int. Assoc. Study Liver 2018, 38, 2170–2177. [Google Scholar] [CrossRef]
- Lee, C.I.; Elmore, J.G. Radiation-Related Risks of Imaging. UpToDate, Wolters Kluwer (Ed. Givens J. and D’Aronson M.). 2022. Available online: https://www.uptodate.com/contents/radiation-related-risks-of-imaging (accessed on 31 December 2022).
- Pereira Guedes, T.; Fragoso, P.; Lemos, C.; Garrido, M.; Silva, J.; Falcão, D.; Maia, L.; Moreira, T.; Manuel Ferreira, J.; Pedroto, I. Long-Term Follow-Up of Advanced Liver Disease after Sustained Virological Response to Treatment of Hepatitis C with Direct-Acting Antivirals: Outcomes from a Real-World Portuguese Cohort. GE Port. J. Gastroenterol. 2020, 27, 149–159. [Google Scholar] [CrossRef]
- Chang, K.C.; Tseng, P.L.; Wu, Y.Y.; Hung, H.C.; Huang, C.M.; Lu, S.N.; Wang, J.H.; Lee, C.M.; Chen, C.H.; Tsai, M.C.; et al. A Polymorphism in Interferon L3 Is an Independent Risk Factor for Development of Hepatocellular Carcinoma after Treatment of Hepatitis C Virus Infection. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2015, 13, 1017–1024. [Google Scholar] [CrossRef]
- Hedenstierna, M.; Nangarhari, A.; Weiland, O.; Aleman, S. Diabetes and Cirrhosis Are Risk Factors for Hepatocellular Carcinoma After Successful Treatment of Chronic Hepatitis C. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2016, 63, 723–729. [Google Scholar] [CrossRef]
- Bonis, P.A.L.; Tong, M.J.; Blatt, L.M.; Conrad, A.; Griffith, J.L. A Predictive Model for The Development of Hepatocellular Carcinoma, Liver Failure, Or Liver Transplantation for Patients Presenting To Clinic With Chronic Hepatitis C. Am. J. Gastroenterol. 1999, 94, 1605–1612. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Mariño, Z.; Perelló, C.; Iñarrairaegui, M.; Ribeiro, A.; Lens, S.; Díaz, A.; Vilana, R.; Darnell, A.; Varela, M.; et al. Unexpected High Rate of Early Tumor Recurrence in Patients with HCV-related HCC Undergoing Interferon-Free Therapy. J. Hepatol. 2016, 65, 719–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waziry, R.; Hajarizadeh, B.; Grebely, J.; Amin, J.; Law, M.; Danta, M.; George, J.; Dore, G.J. Hepatocellular Carcinoma Risk Following Direct-Acting Antiviral HCV Therapy: A Systematic Review, Meta-Analyses, and Meta-Regression. J. Hepatol. 2017, 67, 1204–1212. [Google Scholar] [CrossRef] [PubMed]
- Saraiya, N.; Yopp, A.C.; Rich, N.E.; Odewole, M.; Parikh, N.D.; Singal, A.G. Systematic Review with Meta-Analysis: Recurrence of Hepatocellular Carcinoma Following Direct-Acting Antiviral Therapy. Aliment. Pharmacol. Ther. 2018, 48, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Aleman, S.; Rahbin, N.; Weiland, O.; Davidsdottir, L.; Hedenstierna, M.; Rose, N.; Verbaan, H.; Stål, P.; Carlsson, T.; Norrgren, H.; et al. A Risk for Hepatocellular Carcinoma Persists Long-Term after Sustained Virologic Response in Patients with Hepatitis C-associated Liver Cirrhosis. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2013, 57, 230–236. [Google Scholar] [CrossRef]
- El-Serag, H.B.; Kanwal, F.; Richardson, P.; Kramer, J. Risk of Hepatocellular Carcinoma after Sustained Virological Response in Veterans with Hepatitis C Virus Infection. Hepatology 2016, 64, 130–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dieperink, E.; Pocha, C.; Thuras, P.; Knott, A.; Colton, S.; Ho, S.B. All-Cause Mortality and Liver-Related Outcomes Following Successful Antiviral Treatment for Chronic Hepatitis C. Dig. Dis. Sci. 2014, 59, 872–880. [Google Scholar] [CrossRef]
- Kanwal, F.; Kramer, J.R.; Asch, S.M.; Cao, Y.; Li, L.; El-Serag, H.B. Long-Term Risk of Hepatocellular Carcinoma in HCV Patients Treated With Direct Acting Antiviral Agents. Hepatology 2020, 71, 44–55. [Google Scholar] [CrossRef]
- Ioannou, G.N.; Beste, L.A.; Green, P.K.; Singal, A.G.; Tapper, E.B.; Waljee, A.K.; Sterling, R.K.; Feld, J.J.; Kaplan, D.E.; Taddei, T.H.; et al. Increased Risk for Hepatocellular Carcinoma Persists Up to 10 Years After HCV Eradication in Patients With Baseline Cirrhosis or High FIB-4 Scores. Gastroenterology 2019, 157, 1264–1278. [Google Scholar] [CrossRef] [Green Version]
- Na, S.K.; Lee, S.J.; Cho, Y.K.; Kim, Y.N.; Choi, E.K.; Song, B.C. Aspartate Aminotransferase-to-Platelet Ratio or Fibros-4 Index Predicts the Development of Hepatocellular Carcinoma in Chronic Hepatitis C Patients with Sustained Virologic Response to Interferon Therapy. J. Interferon Cytokine Res. Off. J. Int. Soc. Interferon Cytokine Res. 2019, 39, 703–710. [Google Scholar] [CrossRef]
- Owusu Sekyere, S.; Schlevogt, B.; Mettke, F.; Kabbani, M.; Deterding, K.; Wirth, T.C.; Vogel, A.; Manns, M.P.; Falk, C.S.; Cornberg, M.; et al. HCC Immune Surveillance and Antiviral Therapy of Hepatitis C Virus Infection. Liver Cancer 2019, 8, 41–65. [Google Scholar] [CrossRef] [PubMed]
- Amaddeo, G.; Nguyen, C.T.; Maillé, P.; Mulé, S.; Luciani, A.; Machou, C.; Rodrigues, A.; Regnault, H.; Mallat, A.; Laurent, A.; et al. Intrahepatic Immune Changes after Hepatitis c Virus Eradication by Direct-Acting Antiviral Therapy. Liver Int. Off. J. Int. Assoc. Study Liver 2020, 40, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Simili, A.; Mazzella, G.; Ravaioli, F.; Festi, D.; Bacchi-Reggiani, M.L.; Porro, A.; Bazzoli, F.; Azzaroli, F. Interleukin 28 Polymorphisms and Hepatocellular Carcinoma Development after Direct Acting Antiviral Therapy for Chronic Hepatitis C. J. Gastrointest. Liver Dis. JGLD 2019, 28, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Inoue-Shinomiya, E.; Murakawa, M.; Asahina, Y.; Nakagawa, M.; Tsuchiya, J.; Sato, A.; Tsunoda, T.; Miyoshi, M.; Nitta, S.; Kawai-Kitahata, F.; et al. Association of Serum Interferon-Λ3 Levels with Hepatocarcinogenesis in Chronic Hepatitis C Patients Treated with Direct-Acting Antiviral Agents. Hepatol. Res. Off. J. Jpn. Soc. Hepatol. 2019, 49, 500–511. [Google Scholar] [CrossRef]
- Huang, C.F.; Wang, S.C.; Yeh, M.L.; Huang, C.I.; Tsai, P.C.; Lin, Z.Y.; Chen, S.C.; Dai, C.Y.; Huang, J.F.; Chuang, W.L.; et al. Association of Serial Serum Major Histocompatibility Complex Class I Chain-Related A Measurements with Hepatocellular Carcinoma in Chronic Hepatitis C Patients after Viral Eradication. J. Gastroenterol. Hepatol. 2019, 34, 249–255. [Google Scholar] [CrossRef]
- Matsuura, K.; Sawai, H.; Ikeo, K.; Ogawa, S.; Iio, E.; Isogawa, M.; Shimada, N.; Komori, A.; Toyoda, H.; Kumada, T.; et al. Genome-Wide Association Study Identifies TLL1 Variant Associated With Development of Hepatocellular Carcinoma After Eradication of Hepatitis C Virus Infection. Gastroenterology 2017, 152, 1383–1394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iio, E.; Matsuura, K.; Shimada, N.; Atsukawa, M.; Itokawa, N.; Abe, H.; Kato, K.; Takaguchi, K.; Senoh, T.; Eguchi, Y.; et al. TLL1 Variant Associated with Development of Hepatocellular Carcinoma after Eradication of Hepatitis C Virus by Interferon-Free Therapy. J. Gastroenterol. 2019, 54, 339–346. [Google Scholar] [CrossRef]
- John, M.; Metwally, M.; Mangia, A.; Romero-Gomez, M.; Berg, T.; Sheridan, D.; George, J.; Eslam, M. TLL1 Rs17047200 Increases the Risk of Fibrosis Progression in Caucasian Patients With Chronic Hepatitis C. Gastroenterology 2017, 153, 1448–1449. [Google Scholar] [CrossRef] [Green Version]
- Degasperi, E.; Galmozzi, E.; Facchetti, F.; Farina, E.; D’Ambrosio, R.; Soffredini, R.; Iavarone, M.; Lampertico, P. TLL1 Variants Do Not Predict Hepatocellular Carcinoma Development in HCV Cirrhotic Patients Treated with Direct-Acting Antivirals. J. Viral Hepat. 2019, 26, 1233–1236. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; Wei, G.; Chang, Q.; Peng, R.; Shi, G.; Zheng, P.; He, F.; Wang, W.; Ming, L. The platelet-to-lymphocyte ratio, superior to the neutrophil-to-lymphocyte ratio, correlates with hepatitis C virus infection. Int. J. Infect. Dis. 2016, 45, 72–77. [Google Scholar] [CrossRef]
- Wu, Y.L.; Fulgenzi, C.A.M.; D’Alessio, A.; Cheon, J.; Nishida, N.; Saeed, A.; Wietharn, B.; Cammarota, A.; Pressiani, T.; Personeni, N.; et al. Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios as Prognostic Biomarkers in Unresectable Hepatocellular Carcinoma Treated with Atezolizumab plus Bevacizumab. Cancers 2022, 14, 5834. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Liu, J.; Wang, J.; Xie, T.; Zhang, Q.; Feng, S.; Deng, H.; Zhong, B. Platelet-to-lymphocyte ratio (PLR) and neutrophil-to-lymphocyte ratio (NLR) are associated with chronic hepatitis B virus (HBV) infection. Int. Immunopharmacol. 2017, 51, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Tian, N.; Li, P.; He, Y.; Tong, L.; Xie, W. The correlation between neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio with nonalcoholic fatty liver disease: A cross-sectional study. Eur. J. Gastroenterol. Hepatol. 2022, 34, 1158–1164. [Google Scholar] [CrossRef]
- Kawagishi, N.; Suda, G.; Nakamura, A.; Kimura, M.; Maehara, O.; Suzuki, K.; Nakamura, A.; Ohara, M.; Izumi, T.; Umemura, M.; et al. Liver steatosis and dyslipidemia after HCV eradication by direct acting antiviral agents are synergistic risks of atherosclerosis. PLOS ONE 2018, 13, e0209615. [Google Scholar] [CrossRef] [Green Version]
- Ramadan, M.S.; Boccia, F.; Moretto, S.M.; Gregorio, F.D.; Gagliardi, M.; Iossa, D.; Durante-Mangoni, E.; Zampino, R. Cardiovascular Risk in Patients with Chronic Hepatitis C Treated with Direct Acting Antivirals. J. Clin. Med. 2022, 11, 5781. [Google Scholar] [CrossRef] [PubMed]
- Graf, C.; Welzel, T.; Bogdanou, D.; Vermehren, J.; Beckel, A.; Bojunga, J.; Friedrich-Rust, M.; Dietz, J.; Kubesch, A.; Mondorf, A.; et al. Hepatitis C Clearance by Direct-Acting Antivirals Impacts Glucose and Lipid Homeostasis. J. Clin. Med. 2020, 9, 2702. [Google Scholar] [CrossRef]






| Characteristic | Overall, N = 46 1 | Female, N = 29 1 | Male, N = 17 1 |
|---|---|---|---|
| Age (years) | 64 (58, 67) | 65 (61, 71) | 57 (51, 66) |
| HCC | 4 (8.7%) | 3 (10%) | 1 (5.9%) |
| Ascites, GI bleeding | 3 (6.5%) | 1 (3.4%) | 2 (12%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Omer, S.; Iftime, A.; Constantinescu, I.; Dina, I. Low-Cost Predictors for Liver Function and Clinical Outcomes after Sustained Virological Response in Patients with HCV-Related Cirrhosis and Thrombocytopenia. Medicina 2023, 59, 146. https://doi.org/10.3390/medicina59010146
Omer S, Iftime A, Constantinescu I, Dina I. Low-Cost Predictors for Liver Function and Clinical Outcomes after Sustained Virological Response in Patients with HCV-Related Cirrhosis and Thrombocytopenia. Medicina. 2023; 59(1):146. https://doi.org/10.3390/medicina59010146
Chicago/Turabian StyleOmer, Secil, Adrian Iftime, Ileana Constantinescu, and Ion Dina. 2023. "Low-Cost Predictors for Liver Function and Clinical Outcomes after Sustained Virological Response in Patients with HCV-Related Cirrhosis and Thrombocytopenia" Medicina 59, no. 1: 146. https://doi.org/10.3390/medicina59010146