
Association between Novel Hematological Indices and Measures of Disease Activity in Patients with Rheumatoid Arthritis


Abstract
:1. Introduction
2. Subjects and Methods
2.1. Study Population
2.2. Collection of Clinical Information
2.3. Assessment of Disease Activity Measures in RA
2.4. Assessment of Hematological Indices
2.5. Statistical Analysis
3. Results
3.1. General Characteristics of the Study Population
3.2. Comparison of Hematological Indices between RA Patients and Controls
3.3. Correlation between Hematological Indices and Disease Activity Parameters
3.4. Comparison of Hematological Indices among Disease Activities Based on Composite Measures
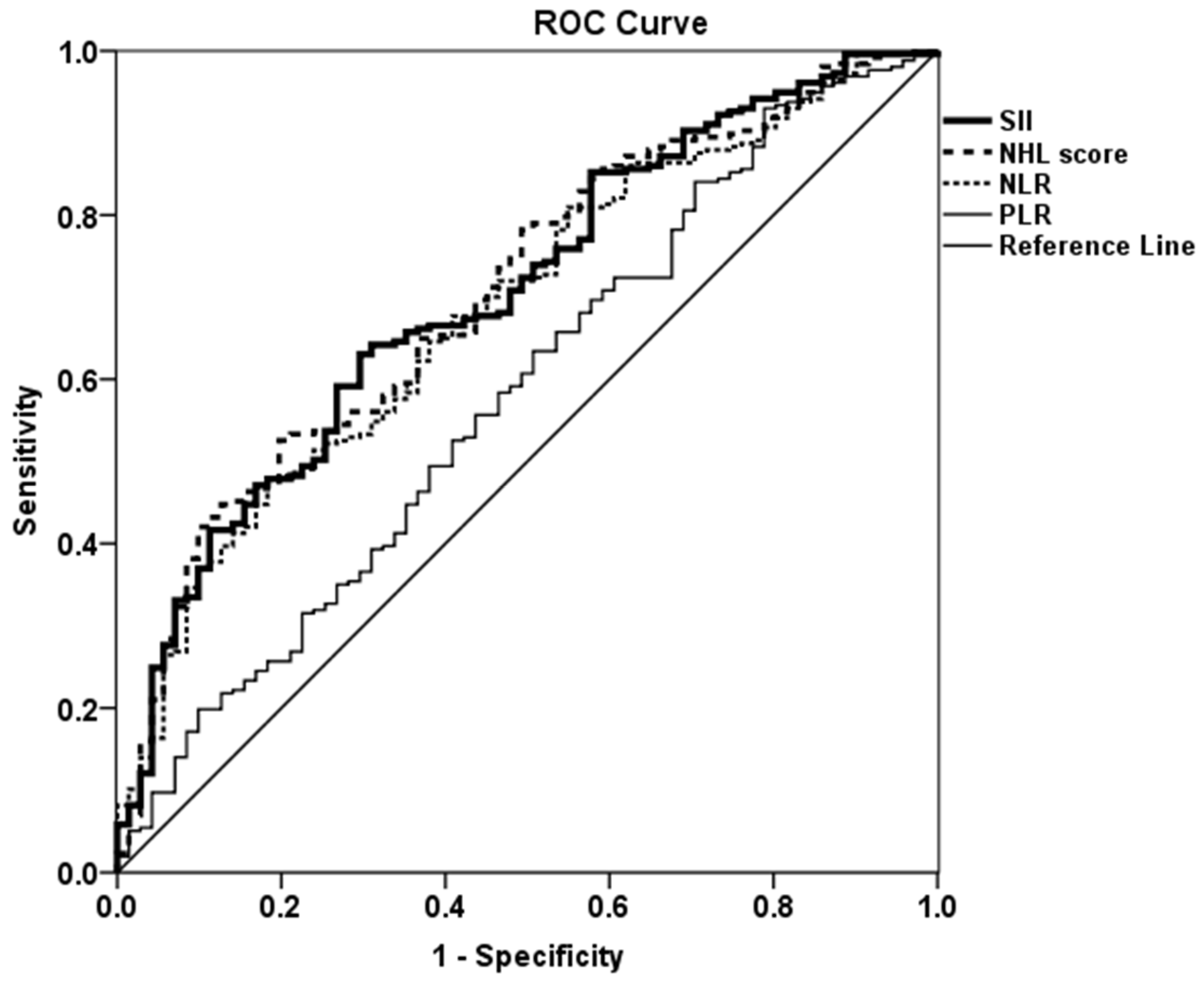
3.5. Assessment of Accuracy of Hematological Indices for the Diagnosis and Remission in RA Using ROC Curve
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aletaha, D.; Smolen, J.S. Diagnosis and Management of Rheumatoid Arthritis: A Review. JAMA 2018, 320, 1360–1372. [Google Scholar] [CrossRef]
- Guo, Q.; Wang, Y.; Xu, D.; Nossent, J.; Pavlos, N.J.; Xu, J. Rheumatoid arthritis: Pathological mechanisms and modern pharmacologic therapies. Bone Res. 2018, 6, 15. [Google Scholar] [CrossRef] [Green Version]
- Anderson, J.K.; Zimmerman, L.; Caplan, L.; Michaud, K. Measures of rheumatoid arthritis disease activity: Patient (PtGA) and Provider (PrGA) Global Assessment of Disease Activity, Disease Activity Score (DAS) and Disease Activity Score with 28-Joint Counts (DAS28), Simplified Disease Activity Index (SDAI), Clinical Disease Activity Index (CDAI), Patient Activity Score (PAS) and Patient Activity Score-II (PASII), Routine Assessment of Patient Index Data (RAPID), Rheumatoid Arthritis Disease Activity Index (RADAI) and Rheumatoid Arthritis Disease Activity Index-5 (RADAI-5), Chronic Arthritis Systemic Index (CASI), Patient-Based Disease Activity Score With ESR (PDAS1) and Patient-Based Disease Activity Score without ESR (PDAS2), and Mean Overall Index for Rheumatoid Arthritis (MOI-RA). Arthritis Care. Res. 2011, 63 (Suppl. 11), S14–S36. [Google Scholar]
- van der Heijde, D.M.; van ‘t Hof, M.; van Riel, P.L.; van de Putte, L.B. Development of a disease activity score based on judgment in clinical practice by rheumatologists. J. Rheumatol. 1993, 20, 579–581. [Google Scholar]
- Smolen, J.S.; Breedveld, F.C.; Schiff, M.H.; Kalden, J.R.; Emery, P.; Eberl, G.; van Riel, P.L.; Tugwell, P. A simplified disease activity index for rheumatoid arthritis for use in clinical practice. Rheumatology 2003, 42, 244–257. [Google Scholar] [CrossRef] [Green Version]
- Aletaha, D.; Smolen, J. The Simplified Disease Activity Index (SDAI) and the Clinical Disease Activity Index (CDAI): A review of their usefulness and validity in rheumatoid arthritis. Clin. Exp. Rheumatol. 2005, 23, S100–S108. [Google Scholar]
- Boilard, E.; Nigrovic, P.A.; Larabee, K.; Watts, G.F.; Coblyn, J.S.; Weinblatt, M.E.; Massarotti, E.M.; Remold-O’Donnell, E.; Farndale, R.W.; Ware, J.; et al. Platelets amplify inflammation in arthritis via collagen-dependent microparticle production. Science 2010, 327, 580–583. [Google Scholar] [CrossRef] [Green Version]
- Scapini, P.; Cassatella, M.A. Social networking of human neutrophils within the immune system. Blood 2014, 124, 710–719. [Google Scholar] [CrossRef]
- Gabay, C.; Kushner, I. Acute-phase proteins and other systemic responses to inflammation. N. Engl. J. Med. 1999, 340, 448–454. [Google Scholar] [CrossRef]
- Maden, M.; Pamuk, G.E.; Pamuk, Ö.N. Development of Atherosclerotic Cardiovascular Mortality in Gouty Arthritis and Rheumatoid Arthritis Patients: Are They Associated With Mean Platelet Volume and Neutrophil-Lymphocyte Ratio? A Comparative Study. Arch. Rheumatol. 2017, 32, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Uslu, A.U.; Küçük, A.; Şahin, A.; Ugan, Y.; Yılmaz, R.; Güngör, T.; Bağcacı, S.; Küçükşen, S. Two new inflammatory markers associated with Disease Activity Score-28 in patients with rheumatoid arthritis: Neutrophil-lymphocyte ratio and platelet-lymphocyte ratio. Int. J. Rheum. Dis. 2015, 18, 731–735. [Google Scholar] [CrossRef]
- Sargin, G.; Senturk, T.; Yavasoglu, I.; Kose, R. Relationship between neutrophil-lymphocyte, platelet-lymphocyte ratio and disease activity in rheumatoid arthritis treated with rituximab. Int. J. Rheum. Dis. 2018, 21, 2122–2127. [Google Scholar] [CrossRef]
- Tekeoğlu, İ.; Gürol, G.; Harman, H.; Karakeçe, E.; Çiftçi, İ.H. Overlooked hematological markers of disease activity in rheumatoid arthritis. Int. J. Rheum. Dis. 2016, 19, 1078–1082. [Google Scholar] [CrossRef]
- Yolbas, S.; Yildirim, A.; Gozel, N.; Uz, B.; Koca, S.S. Hematological Indices May Be Useful in the Diagnosis of Systemic Lupus Erythematosus and in Determining Disease Activity in Behçet’s Disease. Med. Princ. Pract. 2016, 25, 510–516. [Google Scholar] [CrossRef]
- Mercan, R.; Bitik, B.; Tufan, A.; Bozbulut, U.B.; Atas, N.; Ozturk, M.A.; Haznedaroglu, S.; Goker, B. The Association Between Neutrophil/Lymphocyte Ratio and Disease Activity in Rheumatoid Arthritis and Ankylosing Spondylitis. J. Clin. Lab. Anal. 2016, 30, 597–601. [Google Scholar] [CrossRef] [Green Version]
- Fu, H.; Qin, B.; Hu, Z.; Ma, N.; Yang, M.; Wei, T.; Tang, Q.; Huang, Y.; Huang, F.; Liang, Y.; et al. Neutrophil- and platelet-to-lymphocyte ratios are correlated with disease activity in rheumatoid arthritis. Clin. Lab. 2015, 61, 269–273. [Google Scholar] [CrossRef]
- Lee, H.N.; Kim, Y.K.; Kim, G.T.; Ahn, E.; So, M.W.; Sohn, D.H.; Lee, S.G. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio as predictors of 12-week treatment response and drug persistence of anti-tumor necrosis factor-α agents in patients with rheumatoid arthritis: A retrospective chart review analysis. Rheumatol. Int. 2019, 39, 859–868. [Google Scholar] [CrossRef]
- Kim, J.W.; Jung, J.Y.; Suh, C.H.; Kim, H.A. Systemic immune-inflammation index combined with ferritin can serve as a reliable assessment score for adult-onset Still’s disease. Clin. Rheumatol. 2021, 40, 661–668. [Google Scholar] [CrossRef]
- Kim, Y.; Choi, H.; Jung, S.M.; Song, J.J.; Park, Y.B.; Lee, S.W. Systemic immune-inflammation index could estimate the cross-sectional high activity and the poor outcomes in immunosuppressive drug-naïve patients with antineutrophil cytoplasmic antibody-associated vasculitis. Nephrology 2019, 24, 711–717. [Google Scholar] [CrossRef]
- Wu, J.; Yan, L.; Chai, K. Systemic immune-inflammation index is associated with disease activity in patients with ankylosing spondylitis. J. Clin. Lab. Anal. 2021, 35, e23964. [Google Scholar] [CrossRef]
- Kim, H.J.; Lee, J.H.; Jang, S.Y.; Bae, M.H.; Yang, D.H.; Park, H.S.; Cho, Y.K.; Jeong, M.H.; Park, J.S.; Kim, H.S.; et al. Prognostic value of novel neutrophil-to-hemoglobin and lymphocyte score in patients with acute myocardial infarction. Eur. J. Inflamm. 2021, 19, 20587392211039095. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis. Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Kaplan, M.J. Role of neutrophils in systemic autoimmune diseases. Arthritis. Res. Ther. 2013, 15, 219. [Google Scholar] [CrossRef]
- Wright, H.L.; Moots, R.J.; Edwards, S.W. The multifactorial role of neutrophils in rheumatoid arthritis. Nat. Rev. Rheumatol. 2014, 10, 593–601. [Google Scholar] [CrossRef]
- Smith, T.L.; Weyrich, A.S. Platelets as central mediators of systemic inflammatory responses. Thromb. Res. 2011, 127, 391–394. [Google Scholar] [CrossRef] [Green Version]
- Olumuyiwa-Akeredolu, O.O.; Page, M.J.; Soma, P.; Pretorius, E. Platelets: Emerging facilitators of cellular crosstalk in rheumatoid arthritis. Nat. Rev. Rheumatol. 2019, 15, 237–248. [Google Scholar] [CrossRef]
- Symmons, D.P.; Farr, M.; Salmon, M.; Bacon, P.A. Lymphopenia in rheumatoid arthritis. J. R. Soc. Med. 1989, 82, 462–463. [Google Scholar] [CrossRef]
- Ponchel, F.; Morgan, A.W.; Bingham, S.J.; Quinn, M.; Buch, M.; Verburg, R.J.; Henwood, J.; Douglas, S.H.; Masurel, A.; Conaghan, P.; et al. Dysregulated lymphocyte proliferation and differentiation in patients with rheumatoid arthritis. Blood 2002, 100, 4550–4556. [Google Scholar] [CrossRef] [Green Version]
- Ganz, T. Anemia of Inflammation. N. Engl. J. Med. 2019, 381, 1148–1157. [Google Scholar] [CrossRef]
- Wilson, A.; Yu, H.T.; Goodnough, L.T.; Nissenson, A.R. Prevalence and outcomes of anemia in rheumatoid arthritis: A systematic review of the literature. Am. J. Med. 2004, 116 (Suppl. 7A), 50S–57S. [Google Scholar] [CrossRef]
- Satis, S. New Inflammatory Marker Associated with Disease Activity in Rheumatoid Arthritis: The Systemic Immune-Inflammation Index. Curr. Health Sci. J. 2021, 47, 553–557. [Google Scholar]
- Cheung, P.P.; Mari, K.; Devauchelle-Pensec, V.; Jousse-Joulin, S.; D’Agostino, M.A.; Chalès, G.; Gaudin, P.; Mariette, X.; Saraux, A.; Dougados, M. Predictive value of tender joints compared to synovitis for structural damage in rheumatoid arthritis. RMD Open 2016, 2, e000205. [Google Scholar] [CrossRef] [Green Version]
- Zengin, O.; Onder, M.E.; Kalem, A.; Bilici, M.; Türkbeyler, I.H.; Ozturk, Z.A.; Kisacik, B.; Onat, A.M. New inflammatory markers in early rheumatoid arthritis. Z. Rheumatol. 2018, 77, 144–150. [Google Scholar] [CrossRef]
- Lee, Y.H. Association between the Neutrophil-to-lymphocyte Ratio, and Platelet-to-lymphocyte Ratio and Rheumatoid Arthritis and their Correlations with the Disease Activity: A Meta-analysis. J. Rheum. Dis. 2018, 25, 169–178. [Google Scholar] [CrossRef]
- Zhang, Y.; Yin, Y.; Kuai, S.; Shan, Z.; Pei, H.; Wang, J. Combination of neutrophil to lymphocyte ratio and platelet to lymphocyte ratio as diagnostic biomarker for rheumatoid arthritis. Int. J. Clin. Exp. Med. 2016, 9, 22076–22081. [Google Scholar]
- Jin, Z.; Cai, G.; Zhang, P.; Li, X.; Yao, S.; Zhuang, L.; Ren, M.; Wang, Q.; Yu, X. The value of the neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio as complementary diagnostic tools in the diagnosis of rheumatoid arthritis: A multicenter retrospective study. J. Clin. Lab. Anal. 2021, 35, e23569. [Google Scholar] [CrossRef]
- Karimifar, M.; Salesi, M.; Farajzadegan, Z. The association of anti-CCP1 antibodies with disease activity score 28 (DAS-28) in rheumatoid arthritis. Adv. Biomed. Res. 2012, 1, 30. [Google Scholar] [CrossRef]
- Shakiba, Y.; Koopah, S.; Jamshidi, A.R.; Amirzargar, A.A.; Massoud, A.; Kiani, A.; Nicknam, M.H.; Nazari, B.; Nikbin, B. Anti-cyclic citrullinated peptide antibody and rheumatoid factor isotypes in Iranian patients with rheumatoid arthritis: Evaluation of clinical value and association with disease activity. Iran. J. Allergy Asthma Immunol. 2014, 13, 147–156. [Google Scholar]
- Targońska-Stępniak, B.; Zwolak, R.; Piotrowski, M.; Grzechnik, K.; Majdan, M. The Relationship between Hematological Markers of Systemic Inflammation (Neutrophil-To-Lymphocyte, Platelet-To-Lymphocyte, Lymphocyte-To-Monocyte Ratios) and Ultrasound Disease Activity Parameters in Patients with Rheumatoid Arthritis. J. Clin. Med. 2020, 9, 2760. [Google Scholar] [CrossRef]
- Sokka, T.; Toloza, S.; Cutolo, M.; Kautiainen, H.; Makinen, H.; Gogus, F.; Skakic, V.; Badsha, H.; Peets, T.; Baranauskaite, A.; et al. Women, men, and rheumatoid arthritis: Analyses of disease activity, disease characteristics, and treatments in the QUEST-RA study. Arthritis Res. Ther. 2009, 11, R7. [Google Scholar]


{kind=link}
| Variables | Rheumatoid Arthritis (n = 257) | Healthy Controls (n = 71) | p Value |
|---|---|---|---|
| Age (year) | 60.7 ± 8.7 | 60.4 ± 7.5 | 0.797 |
| Disease duration (year) | 11.2 ± 8.2 | ||
| Rheumatoid factor (IU/mL) | 99.2 ± 147.9 | ||
| Rheumatoid factor (≥14 IU/mL), n (%) | 226 (87.9) | ||
| Anti-cyclic citrullinated peptide (U/mL) | 317.4 ± 198.9 | ||
| Anti-cyclic citrullinated peptide (≥17 U/mL), n (%) | 224 (87.2) | ||
| Disease activity indices | |||
| Erythrocyte sedimentation rate (mm/h) | 28.5 ± 20.8 | 19.8 ± 13.5 | <0.001 |
| C-reactive protein (mg/L) | 5.0 ± 11.5 | 1.9 ± 4.5 | 0.001 |
| Tender joint count | 3.02 ± 3.27 | ||
| Swollen joint count | 0.74 ± 2.02 | ||
| Patient VAS (mm) | 30.2 ± 24.6 | ||
| Physician VAS (mm) | 19.0 ± 15.3 | ||
| DAS28-ESR | 3.45 ± 1.22 | ||
| DAS28-CRP | 2.71 ± 1.12 | ||
| CDAI | 8.7 ± 7.5 | ||
| SDAI | 9.2 ± 8.1 | ||
| Current medications | |||
| Glucocorticoid | 213 (82.9) | ||
| csDMARDs | 247 (96.1) | ||
| bDMARDs | 79 (30.7) | ||
| tsDMARDs | 22 (8.6) |
| Variables | Rheumatoid Arthritis (n = 257) | Healthy Controls (n = 71) | p Value |
|---|---|---|---|
| Whole blood cell counts | |||
| White blood count (×103/µL) | 6.9 ± 2.3 | 5.4 ± 1.3 | <0.001 |
| Hemoglobin (g/dL) | 12.5 ± 1.2 | 12.9 ± 1.2 | 0.012 |
| Platelet (×103/µL) | 264.4 ± 73.4 | 234.1 ± 63.6 | 0.002 |
| Neutrophil (%) | 60.3 ± 10.8 | 53.3 ± 10.4 | <0.001 |
| Lymphocytes (%) | 28.9 ± 9.6 | 36.1 ± 10.0 | <0.001 |
| Neutrophil (×103/µL) | 4.3 ± 1.9 | 2.9 ± 1.0 | <0.001 |
| Lymphocytes (×103/µL) | 1.9 ± 0.7 | 1.9 ± 0.6 | 0.736 |
| Hematological indices | |||
| SII | 697.1 ± 579.4 | 409.1 ± 277.4 | <0.001 |
| NHL score (/g/dL) | 0.207 ± 0.140 | 0.135 ± 0.080 | <0.001 |
| NLR | 2.552 ± 1.673 | 1.693 ± 0.858 | <0.001 |
| PLR | 158.2 ± 93.6 | 134.9 ± 55.2 | 0.046 |
| Disease Activity Indices | Hematological Indices | |||||||
|---|---|---|---|---|---|---|---|---|
| SII | NHL Score | NLR | PLR | |||||
| r | p | r | p | r | p | r | p | |
| Composite indices | ||||||||
| DAS28-ESR | 0.159 | 0.011 | 0.133 | 0.033 | 0.111 | 0.075 | 0.030 | 0.637 |
| DAS28-CRP | 0.196 | 0.002 | 0.183 | 0.003 | 0.172 | 0.006 | 0.027 | 0.666 |
| CDAI | 0.173 | 0.006 | 0.171 | 0.006 | 0.158 | 0.011 | 0.012 | 0.844 |
| SDAI | 0.144 | 0.021 | 0.194 | 0.002 | 0.179 | 0.004 | 0.031 | 0.618 |
| Individual indices | ||||||||
| ESR | 0.144 | 0.021 | 0.107 | 0.086 | 0.064 | 0.307 | 0.048 | 0.446 |
| CRP | 0.299 | <0.001 | 0.251 | <0.001 | 0.224 | <0.001 | 0.193 | 0.025 |
| Tender joint count | 0.059 | 0.344 | 0.048 | 0.440 | 0.044 | 0.485 | −0.043 | 0.493 |
| Swollen joint count | 0.215 | <0.001 | 0.230 | <0.001 | 0.214 | 0.001 | 0.078 | 0.215 |
| Physician VAS | 0.222 | <0.001 | 0.228 | <0.001 | 0.207 | 0.001 | 0.057 | 0.360 |
| Patient VAS | 0.130 | 0.038 | 0.124 | 0.047 | 0.118 | 0.059 | −0.005 | 0.939 |
| Hematological Indices | Disease Activity Subgroups Based on Composite Indices | |||
|---|---|---|---|---|
| Remission | Low | Moderate to High | p Value | |
| DAS28-ESR | ||||
| SII | 391.2 (265.4–571.6) | 543.5 (366.8–801.9) | 606.5 (423.5–961.3) | <0.001 |
| NHL score | 0.143 (0.102–0.197) | 0.188 (0.112–0.238) | 0.192 (0.127–0.276) | 0.004 |
| NLR | 1.771 (1.302–2.545) | 2.186 (1.460–3.234) | 2.305 (1.618–3.214) | 0.021 |
| PLR | 124.6 (102.7–156.1) | 146.7 (110.4–185.7) | 148.4 (119.8–185.9) | 0.021 |
| DAS28-CRP | ||||
| SII | 440.0 (324.6–733.7) | 598.5 (371.7–750.2) | 672.5 (423.3–1068.4) | 0.001 |
| NHL score | 0.150 (0.102–0.225) | 0.176 (0.119–0.230) | 0.204 (0.131–0.284) | 0.005 |
| NLR | 1.828 (1.314–2.696) | 2.137 (1.485–2.901) | 2.531 (1.699–3.322) | 0.012 |
| PLR | 129.5 (103.1–162.5) | 144.4 (116.9–183.6) | 147.2 (118.7–186.3) | 0.165 |
| SDAI | ||||
| SII | 812.5 (505.8–1266.1) | 507.6 (342.4–762.4) | 757.2 (473.3–1171.3) | 0.001 |
| NHL score | 0.228 (0.176–0.332) | 0.164 (0.115–0.232) | 0.232 (0.138–0.300) | 0.003 |
| NLR | 2.720 (1.910–3.566) | 2.001 (1.437–2.864) | 2.768 (1.771–3.516) | 0.007 |
| PLR | 148.1 (121.0–185.6) | 137.8 (111.0–173.9) | 149.2 (118.7–193.2) | 0.293 |
| CDAI | ||||
| SII | 433.5 (3.27.1–804.8) | 506.0 (338.1–746.1) | 759.5 (477.5–1174.0) | 0.001 |
| NHL score | 0.160 (0.110–0.267) | 0.162 (0.110–0.223) | 0.232 (0.142–0.303) | 0.002 |
| NLR | 1.944 (1.384–3.455) | 1.954 (1.405–2.727) | 2.775 (1.773–3.553) | 0.003 |
| PLR | 131.4 (107.4–163.5) | 137.3 (108.9–172.4) | 149.9 (119.0–196.0) | 0.314 |
| Variables | AUC | 95% CI | p Value |
|---|---|---|---|
| SII | 0.662 | 0.583–0.741 | <0.001 |
| NHL score | 0.623 | 0.544–0.701 | 0.003 |
| NLR | 0.608 | 0.528–0.688 | 0.010 |
| PLR | 0.628 | 0.550–0.706 | 0.002 |
| ESR | 0.807 | 0.749–0.864 | <0.001 |
| CRP | 0.692 | 0.627–0.757 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choe, J.-Y.; Lee, C.U.; Kim, S.-K. Association between Novel Hematological Indices and Measures of Disease Activity in Patients with Rheumatoid Arthritis. Medicina 2023, 59, 117. https://doi.org/10.3390/medicina59010117
Choe J-Y, Lee CU, Kim S-K. Association between Novel Hematological Indices and Measures of Disease Activity in Patients with Rheumatoid Arthritis. Medicina. 2023; 59(1):117. https://doi.org/10.3390/medicina59010117
Chicago/Turabian StyleChoe, Jung-Yoon, Chan Uk Lee, and Seong-Kyu Kim. 2023. "Association between Novel Hematological Indices and Measures of Disease Activity in Patients with Rheumatoid Arthritis" Medicina 59, no. 1: 117. https://doi.org/10.3390/medicina59010117