The Addition of Hypomethylating Agents to Low-Intensity Induction Chemotherapy Does Not Improve Outcomes in Elderly Acute Myeloid Leukemia Patients: A Single-Center Retrospective Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatment
2.3. Definitions and Statistical Analysis
3. Results
3.1. Clinical Characteristics
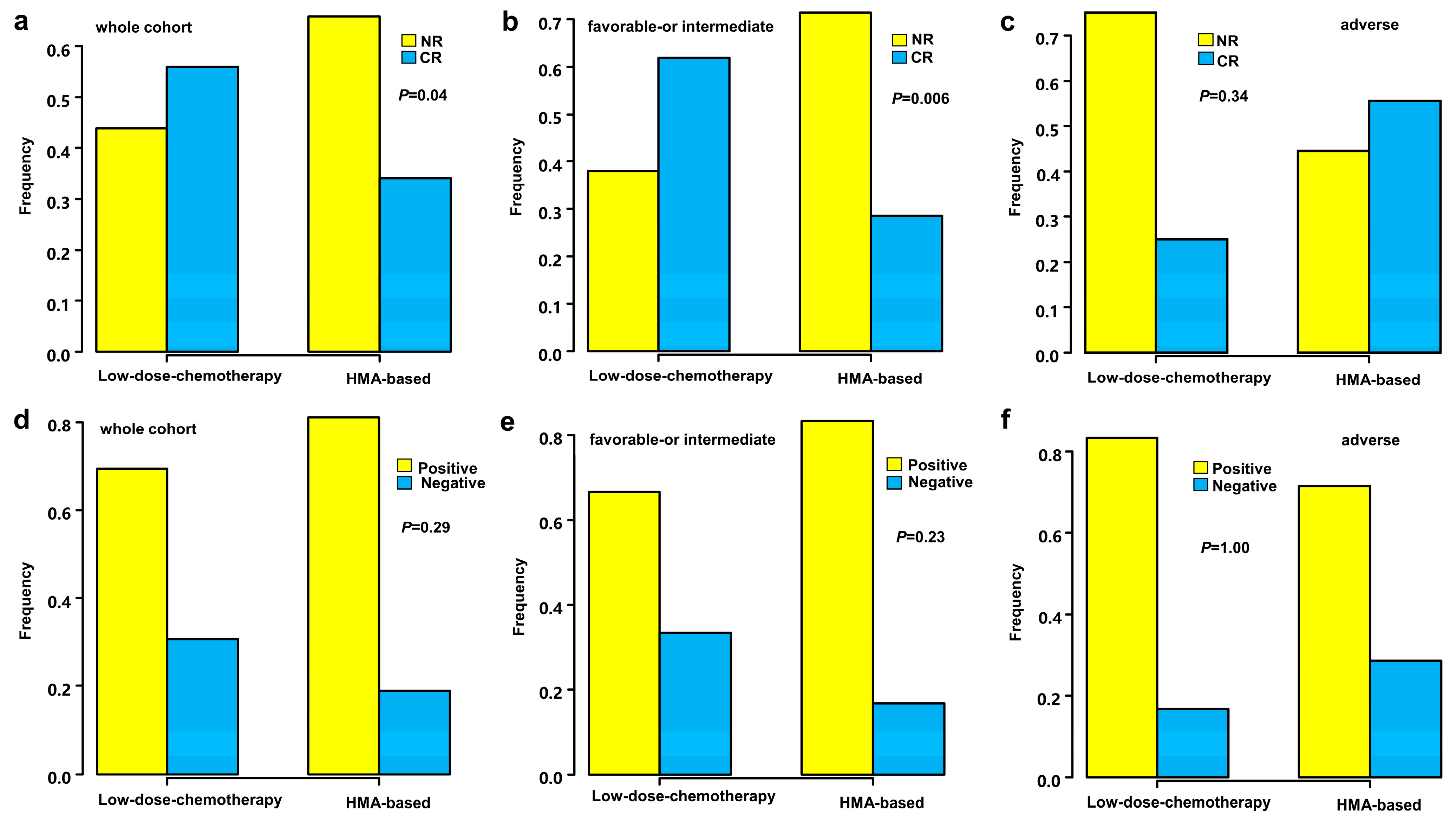
3.2. Response to Induction Therapy
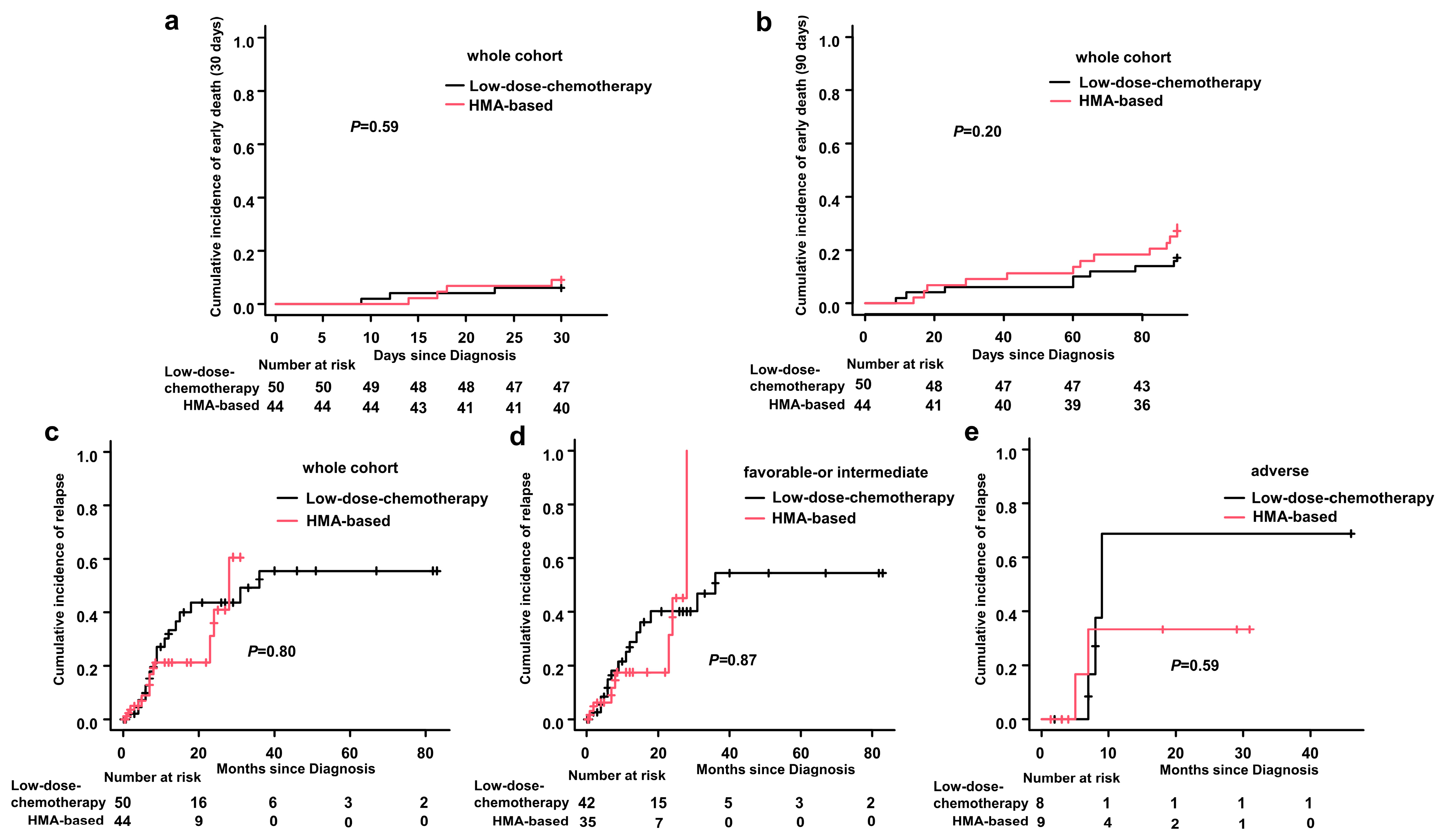
3.3. Early Death
3.4. Disease Relapse
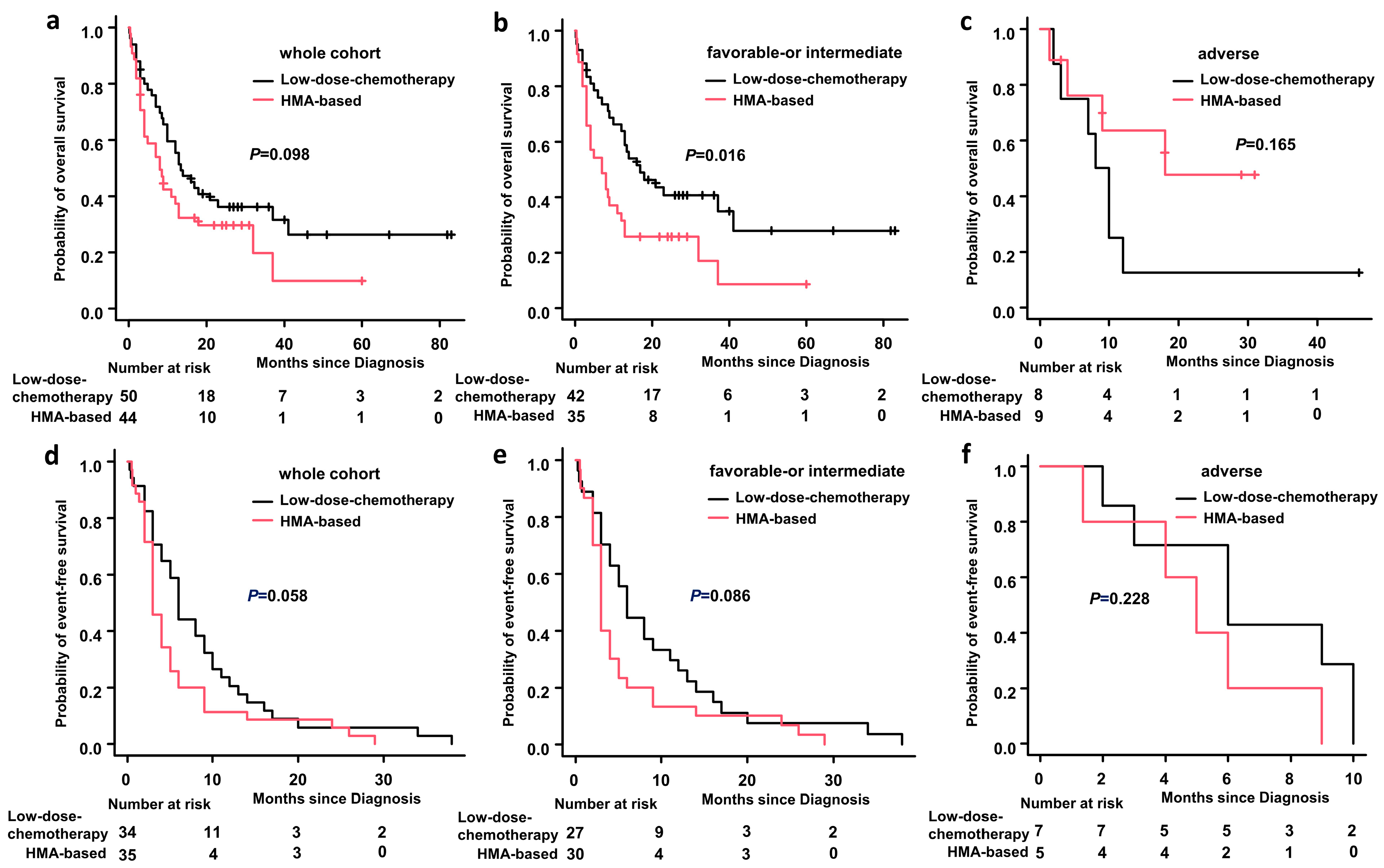
3.5. OS and EFS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shallis, R.M.; Wang, R. Epidemiology of acute myeloid leukemia: Recent progress and enduring challenges. Blood Rev. 2019, 36, 70–87. [Google Scholar] [CrossRef] [PubMed]
- Quintas-Cardama, A.; Ravandi, F. Epigenetic therapy is associated with similar survival compared with intensive chemotherapy in older patients with newly diagnosed acute myeloid leukemia. Blood 2012, 120, 4840–4845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowenberg, B.; Ossenkoppele, G.J. High-dose daunorubicin in older patients with acute myeloid leukemia. N. Engl. J. Med. 2009, 361, 1235–1248. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, B.C.; Satram-Hoang, S. Big data analysis of treatment patterns and outcomes among elderly acute myeloid leukemia patients in the United States. Ann. Hematol. 2015, 94, 1127–1138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oran, B.; Weisdorf, D.J. Survival for older patients with acute myeloid leukemia: A population-based study. Haematologica 2012, 97, 1916–1924. [Google Scholar] [CrossRef] [PubMed]
- Zavras, P.D.; Shastri, A. Clinical Trials Assessing Hypomethylating Agents Combined with Other Therapies: Causes for Failure and Potential Solutions. Clin. Cancer Res. 2021, 27, 6653–6661. [Google Scholar] [CrossRef] [PubMed]
- Dawson, M.A. The cancer epigenome: Concepts, challenges, and therapeutic opportunities. Science 2017, 355, 1147–1152. [Google Scholar] [CrossRef] [PubMed]
- Craddock, C.; Quek, L. Azacitidine fails to eradicate leukemic stem/progenitor cell populations in patients with acute myeloid leukemia and myelodysplasia. Leukemia 2013, 27, 1028–1036. [Google Scholar] [CrossRef] [PubMed]
- DiNardo, C.D.; Pratz, K. Venetoclax combined with decitabine or azacitidine in treatment-naive, elderly patients with acute myeloid leukemia. Blood 2019, 133, 7–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dohner, H.; Estey, E. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.E.; Heidel, F.H. Randomized comparison of low dose cytarabine with or without glasdegib in patients with newly diagnosed acute myeloid leukemia or high-risk myelodysplastic syndrome. Leukemia 2019, 33, 379–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DiNardo, C.D.; Jonas, B.A. Azacitidine and Venetoclax in Previously Untreated Acute Myeloid Leukemia. N. Engl. J. Med. 2020, 383, 617–629. [Google Scholar] [CrossRef] [PubMed]
- Kantarjian, H.M.; Thomas, X.G. Multicenter, randomized, open-label, phase III trial of decitabine versus patient choice, with physician advice, of either supportive care or low-dose cytarabine for the treatment of older patients with newly diagnosed acute myeloid leukemia. J. Clin. Oncol. 2012, 30, 2670–2677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frohling, S.; Schlenk, R.F. Cytogenetics and age are major determinants of outcome in intensively treated acute myeloid leukemia patients older than 60 years: Results from AMLSG trial AML HD98-B. Blood 2006, 108, 3280–3288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, X.N.; Zhou, X.P. Epigenetic priming with decitabine followed by low-dose idarubicin/cytarabine has an increased anti-leukemic effect compared to traditional chemotherapy in high-risk myeloid neoplasms. Leuk. Lymphoma 2016, 57, 1311–1318. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| HMA-Based n = 44 | Low-Dose-Chemotherapy n = 50 | p Values | |
|---|---|---|---|
| Age (years), median (range) | 69 (60–83) | 70 (60–83) | 0.539 |
| Age ≥ 75 years, n (%) | 8 (18.2) | 7(14.0) | 0.767 |
| Sex: M/F, n (%) | 21/23 (47.7/52.3) | 30/20 (60.0/40.0) | 0.300 |
| WBC at first diagnosis (×109/L), median (range) | 6.8 (0.52–172.05) | 5.5 (0.83–139.2) | 0.264 |
| PLT at first diagnosis (×109/L), median (range) | 56.5 (6–532) | 52.5 (4–285) | 0.557 |
| LDH level at first diagnosis, median (range) | 302 (153–11,372) | 346 (127–889) | 0.771 |
| CD56 positive expression, n (%) | 6 (13.6) | 11 (22.0) | 0.421 |
| ECOG-PS, n (%) 0–1 ≥2 | 19 (43.2) 25 (56.8) | 16 (32.0) 34 (68.0) | 0.291 |
| Comorbidities, n (%) Hypertension Diabetes Heart disease Cerebral infarction Hepatitis Arrhythmia Tumor Rheumatism Fracture Gout lumbar disc protrusion Eye diseases Hypothyroidism Mental illness Pulmonary tuberculosis Syphilis Chronic obstructive pulmonary disease None | 10 (22.7) 5 (11.4) 0 (0.0) 3 (6.9) 2 (4.5) 0 (0.0) 2 (4.5) 1 (2.3) 1 (2.3) 1 (2.3) 0 (0.0) 1 (2.3) 1 (2.3) 0 (0.0) 0 (0.0) 1 (2.3) 1 (2.3) 15 (34.1) | 15 (30.0) 5 (10.0) 1 (2.0) 0 (0.0) 2 (4.0) 2 (4.0) 1 (2.0) 0 (0.0) 2 (4.0) 0 (0.0) 2 (4.0) 1 (2.0) 0 (0.0) 1 (2.0) 1 (2.0) 0 (0.0) 2 (4.0) 15 (30.0) | 0.645 |
| Two or more comorbidities, n (%) | 9 (20.5) | 6 (12.0) | 0.398 |
| Molecular biology, n (%) NPM1 mutation FLT3 mutation FLT3 mutation MPM1 mutation Biallelic mutated CEBPA CEBPA mutation CEBPB mutation CBFB-MYH11 mutation AML1-ETO mutation MLL arrangements DNMT3A mutation TET-2 mutation CSF3R mutation Negative detection No data | 6 (13.6) 2 (4.5) 1 (2.3) 1 (2.3) 0 (0.0) 1 (2.3) 1 (2.3) 1 (2.3) 1 (2.3) 1 (2.3) 1 (2.3) 0 (0.0) 19 (43.2) 9 (20.5) | 5 (10.0) 3 (6.0) 3 (6.0) 3 (6.0) 1 (2.0) 0 (0.0) 0 (0.0) 2 (4.0) 0 (0.0) 0 (0.0) 0 (0.0) 1 (2.0) 29 (58.0) 3 (6.0) | 0.178 |
| ELN risk assessment, n (%) Favorable-risk Intermediate-risk High-risk | 10 (22.7) 25 (56.8) 9 (20.5) | 8 (16.0) 34 (68.0) 8 (16.0) | 0.558 |
| Response after one course of induction, n (%) CR CRi PR ORR | 15 (34.1) 3 (6.8) 6 (13.6) 24 (54.5) | 28 (56.0) 4 (8.0) 4 (8.0) 36 (72.0) | 0.040 1.000 0.579 0.090 |
| Severe infection at first diagnosis, n (%) | 24 (54.5) | 26 (52.0) | 0.838 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, D.; Wang, X.; Tong, J.; Zhou, L.; Chen, E.; Zhou, Z.; Xue, L.; Zhang, X.; Sun, G.; Zheng, C. The Addition of Hypomethylating Agents to Low-Intensity Induction Chemotherapy Does Not Improve Outcomes in Elderly Acute Myeloid Leukemia Patients: A Single-Center Retrospective Study. Medicina 2023, 59, 114. https://doi.org/10.3390/medicina59010114
Liu D, Wang X, Tong J, Zhou L, Chen E, Zhou Z, Xue L, Zhang X, Sun G, Zheng C. The Addition of Hypomethylating Agents to Low-Intensity Induction Chemotherapy Does Not Improve Outcomes in Elderly Acute Myeloid Leukemia Patients: A Single-Center Retrospective Study. Medicina. 2023; 59(1):114. https://doi.org/10.3390/medicina59010114
Chicago/Turabian StyleLiu, Dan, Xiaoyu Wang, Juan Tong, Li Zhou, Erling Chen, Ziwei Zhou, Lei Xue, Xuhan Zhang, Guangyu Sun, and Changcheng Zheng. 2023. "The Addition of Hypomethylating Agents to Low-Intensity Induction Chemotherapy Does Not Improve Outcomes in Elderly Acute Myeloid Leukemia Patients: A Single-Center Retrospective Study" Medicina 59, no. 1: 114. https://doi.org/10.3390/medicina59010114