

A Predictive Model to Evaluate the HbeAg Positivity of Chronic Hepatitis B Virus Patients in Clinics: A Cross-Sectional Study
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Methods
2.3. Statistical Analysis
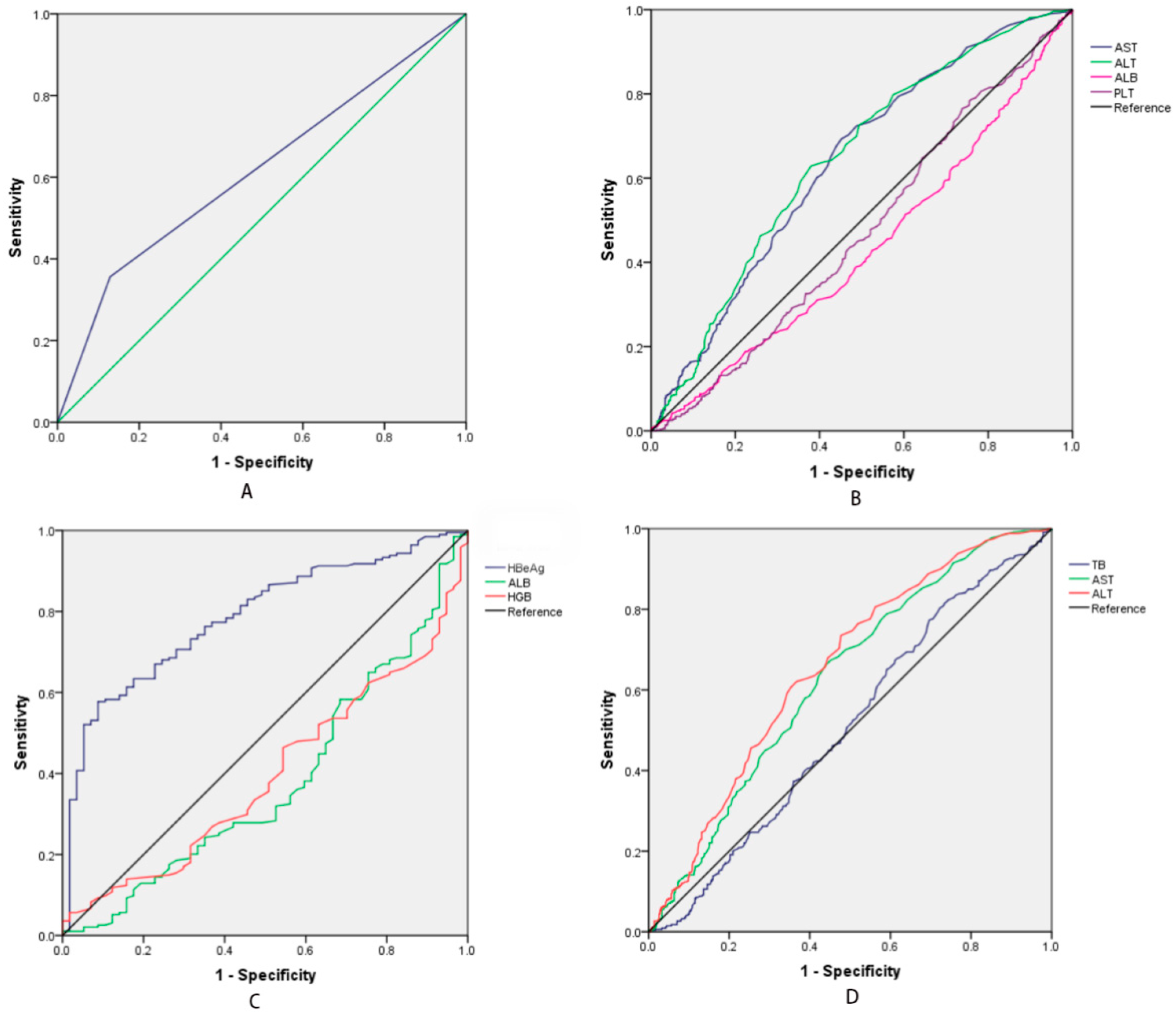
3. Results
3.1. The Characteristic of HBeAg (+) and HBeAg (−) Patients
3.2. The Characteristics in Different HBV DNA Levels
3.3. The Different HBV DNA Levels in the HBeAg (+) Group
3.4. The Different HBV DNA Levels in the HBeAg (−) Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- World Health Organization. [Fact Sheet]. Hepatitis B. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b/ (accessed on 24 June 2022).
- Kao, J.H.; Chen, D.S. Global control of hepatitis B virus infection. Lancet Infect. Dis. 2002, 2, 395–403. [Google Scholar] [CrossRef]
- Yang, K.; Pan, Y.; Jin, L.; Yu, F.; Zhang, F. Low Serum Soluble Transferrin Receptor Levels Are Associated with Poor Prognosis in Patients with Hepatitis B Virus-Related Acute-on-Chronic Liver Failure. Biol. Trace Elem. Res. 2022; epub ahead of print. [Google Scholar] [CrossRef]
- Shi, M.; Zhou, Z.; Zhou, Z.; Shen, L.; Shen, J.; Zhou, G.; Zhu, R. Identification of key genes and infiltrating immune cells among acetaminophen-induced acute liver failure and HBV-associated acute liver failure. Ann. Transl. Med. 2022, 10, 775. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.H.; Shi, C.H. Molecular characteristics and stages of chronic hepatitis B virus infection. World J. Gastroenterol. 2009, 15, 3099–3105. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Cho, H.C.; Choi, M.S.; Lee, J.H.; Koh, K.C.; Yoo, B.C.; Paik, S.W. The change of the quantitative HBsAg level during the natural course of chronic hepatitis B. Liver Int. 2011, 31, 817–823. [Google Scholar] [CrossRef]
- Jaroszewicz, J.; Serrano, B.C.; Wursthorn, K.; Deterding, K.; Schlue, J.; Raupach, R.; Flisiak, R.; Bock, C.-T.; Manns, M.P.; Wedemeyer, H.; et al. Hepatitis B surface antigen (HBsAg) levels in the natural history of hepatitis B virus (HBV)-infection: A European perspective. J. Hepatol. 2010, 52, 514–522. [Google Scholar] [CrossRef]
- Liaw, Y.F.; Kao, J.H.; Piratvisuth, T.; Chan, H.L.; Chien, R.N.; Liu, C.J.; Gane, E.; Locarnini, S.; Lim, S.G.; Han, K.H.; et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: A 2012 update. Hepatol. Int. 2012, 6, 531–561. [Google Scholar] [CrossRef]
- Iloeje, U.H.; Yang, H.I.; Su, J.; Jen, C.L.; You, S.L.; Chen, C.J. Predicting cirrhosis risk based on the level of circulating hepatitis B viral load. Gastroenterology 2006, 130, 678–686. [Google Scholar] [CrossRef]
- Gish, R.G.; Locarnini, S.A. Chronic hepatitis B: Current testing strategies. Clin. Gastroenterol. Hepatol. 2006, 4, 666–676. [Google Scholar] [CrossRef]
- Andersson, K.L.; Chung, R.T. Monitoring During and After Antiviral Therapy for Hepatitis B. Hepatology 2009, 49, S166–S173. [Google Scholar] [CrossRef] [Green Version]
- Gupta, E.; Kumar, A.; Choudhary, A.; Kumar, M.; Sarin, S.K. Serum hepatitis B surface antigen levels correlate with high serum HBV DNA levels in patients with chronic hepatitis B: A cross-sectional study. Indian J. Med. Microbiol. 2012, 30, 150–154. [Google Scholar] [CrossRef]
- Nguyen, T.; Thompson, A.J.; Bowden, S.; Croagh, C.; Bell, S.; Desmond, P.V.; Levy, M.; Locarnini, S.A. Hepatitis B surface antigen levels during the natural history of chronic hepatitis B: A perspective on Asia. J. Hepatol. 2010, 52, 508–513. [Google Scholar] [CrossRef]
- Vigano, M.; Lampertico, P. Clinical implications of HBsAg quantification in patients with chronic hepatitis B. Saudi J. Gastroenterol. 2012, 18, 81–86. [Google Scholar] [PubMed]
- Alghamdi, A.; Aref, N.; El-Hazmi, M.; Al-Hamoudi, W.; Alswat, K.; Helmy, A.; Sanai, F.M.; Abdo, A.A. Correlation between Hepatitis B surface antigen titers and HBV DNA levels. Saudi J. Gastroenterol. 2013, 19, 252–257. [Google Scholar] [PubMed]
- Brunetto, M.R.; Oliveri, F.; Colombatto, P.; Moriconi, F.; Ciccorossi, P.; Coco, B.; Romagnoli, V.; Cherubini, B.; Moscato, G.; Maina, A.M.; et al. Hepatitis B surface antigen serum levels help to distinguish active from inactive hepatitis B virus genotype D carriers. Gastroenterology 2010, 139, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.L.; Liao, L.Y.; Liu, C.J.; Yu, M.W.; Chen, P.J.; Lai, M.Y.; Chen, D.S.; Kao, J.H. Hepatitis B viral factors in HBeAg-negative carriers with persistently normal serum alanine aminotransferase levels. Hepatology 2007, 45, 1193–1198. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, M.; Misra, S.P.; Misra, V.; Pandey, A.; Pant, S.; Singh, R.; Verma, M. Seroprevalence of hepatitis B infection during pregnancy and risk of perinatal transmission. Indian J. Gastroenterol. 2011, 30, 66–71. [Google Scholar] [CrossRef]
- Chen, P.; Xie, Q.; Lu, X.; Yu, C.; Xu, K.; Ruan, B.; Cao, H.; Gao, H.; Li, L. Serum HBeAg and HBV DNA levels are not always proportional and only high levels of HBeAg most likely correlate with high levels of HBV DNA A community-based study. Medicine 2017, 96, e7766. [Google Scholar] [CrossRef]
- Lai, C.L.; Ratziu, V.; Yuen, M.F.; Poynard, T. Viral hepatitis B. Lancet 2003, 362, 2089–2094. [Google Scholar] [CrossRef]
- Iannacone, M.; Sitia, G.; Isogawa, M.; Marchese, P.; Castro, M.G.; Lowenstein, P.R.; Chisari, F.; Ruggeri, Z.M.; Guidotti, L.G. Platelets mediate cytotoxic T lymphocyte-induced liver damage. Nat. Med. 2005, 11, 1167–1169. [Google Scholar] [CrossRef] [Green Version]
- Iannacone, M.; Sitia, G.; Guidotti, L.G. On the role of platelets in the pathogenesis of viral hepatitis. J. Hepatol. 2009, 51, 599–600. [Google Scholar] [CrossRef]
- Foy, B.H.; Sundt, T.M.; Carlson, J.C.T.; Aguirre, A.D.; Higgins, J.M. Human acute inflammatory recovery is defined by co-regulatory dynamics of white blood cell and platelet populations. Nat. Commun. 2022, 13, 4705. [Google Scholar] [CrossRef] [PubMed]
- Lin, Q.; Yang, G.; Ruan, J.; Yu, P.; Deng, C.; Pan, W. Study of the Significance of Thromboelastography Changes in Patients with Dyslipidemia. Emerg. Med. Int. 2022, 2022, 1927881. [Google Scholar] [CrossRef] [PubMed]
- Sarin, S.K.; Kumar, M. Should chronic HBV infected patients with normal ALT treated: Debate. Hepatol. Int. 2008, 2, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Zeng, D.-W.; Liu, Y.-R.; Dong, J.; Zhu, Y.-Y.; Li, Y.-B.; Chen, J.; Zheng, Q.; Jiang, J.-J. Serum HBsAg and HBeAg levels are associated with liver pathological stages in the immune clearance phase of hepatitis B virus chronic infection. Mol. Med. Rep. 2015, 11, 3465–3472. [Google Scholar] [CrossRef]
- Almeida-Becerril, T.; Rodríguez-Cruz, M.; Hernández-Cruz, S.Y.; Ruiz-Cruz, E.D.; Mendoza, C.R.S.; Cárdenas-Conejo, A.; Escobar-Cedillo, R.E.; Ávila-Moreno, F.; Aquino-Jarquin, G. Natural history of circulating miRNAs in Duchenne disease: Association with muscle injury and metabolic parameters. Acta Neurol. Scand. 2022; epub ahead of print. [Google Scholar] [CrossRef]
- Kim, H.C.; Nam, C.M.; Jee, S.H.; Han, K.H.; Oh, D.K.; Suh, I. Normal serum aminotransferase concentration and risk of mortality from liver diseases: Prospective cohort study. BMJ 2004, 328, 983–988. [Google Scholar] [PubMed]
- Cai, J.; Wu, W.; Wu, J.; Chen, Z.; Wu, Z.; Tang, Y.; Hu, M. Prevalence and clinical characteristics of hepatitis B surface antigen-negative/hepatitis B core antibody-positive patients with detectable serum hepatitis B virus DNA. Ann. Transl. Med. 2022, 10, 25. [Google Scholar] [CrossRef] [PubMed]
- Werle-Lapostolle, B.; Bowden, S.; Locarnini, S.; Wursthorn, K.; Petersen, J.; Lau, G.; Trepo, C.; Marcellin, P.; Goodman, Z.; Delaney, W.E., IV; et al. Persistence of cccDNA during the natural history of chronic hepatitis B and decline during adefovir dipivoxil therapy. Gastroenterology 2004, 126, 1750–1758. [Google Scholar] [CrossRef]
- Wursthorn, K.; Lutgehetmann, M.; Dandri, M.; Volz, T.; Buggisch, P.; Zollner, B.; Longerich, T.; Schirmacher, P.; Metzler, F.; Zankel, M.; et al. Peginterferon alpha-2b plus adefovir induce strong cccDNA decline and HBsAg reduction in patients with chronic hepatitis B. Hepatology 2006, 44, 675–684. [Google Scholar] [CrossRef]
- Chan, H.L.; Wong, V.W.; Tse, A.M.; Tse, C.; Chim, A.M.; Chan, H.; Wong, G.L.; Sung, J.J. Serum hepatitis B surface antigen quantitation can reflect hepatitis B virus in the liver and predict treatment response. Clin. Gastroenterol. Hepatol. 2007, 5, 1462–1468. [Google Scholar] [CrossRef]
- Shanshan, W.; Xinfang, D.; Shuihong, Y.; Kecong, L.; Jinjin, Q.; Zhi, C.; Feng, C. Pathological changes of liver one year later in CHB patients with negative HBV DNA. Infect. Agents Cancer 2019, 14, 48. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | HBeAg | HBV DNA Levels | ||||
|---|---|---|---|---|---|---|
| HBeAg (+) | HBeAg (−) | P1 Value | High | Low | P2 Value | |
| Sex (male/female) | 223/29 | 658/110 | 0.258 | 474/61 | 407/78 | 0.030 |
| Age (years) | 46.49 ± 10.47 | 52.12 ± 12.03 | <0.001 | 50.42 ± 11.29 | 51.05 ± 12.56 | 0.394 |
| HGB (g/L) | 135.63 ± 23.00 | 134.90 ± 21.69 | 0.650 | 134.46 ± 22.88 | 135.78 ± 21.02 | 0.340 |
| PLT (×109/L) | 121.60 ± 76.57 | 140.81 ± 82.00 | 0.001 | 129.84 ± 70.75 | 142.87 ± 90.80 | 0.011 |
| WBC (×109/L) | 5.48 ± 3.38 | 5.91 ± 3.42 | 0.083 | 5.66 ± 3.23 | 5.95 ± 3.60 | 0.184 |
| TB (umol/L) | 25.94 ± 53.78 | 25.37 ± 51.48 | 0.878 | 23.18 ± 45.26 | 28.09 ± 58.7 | 0.133 |
| AST (IU/L) (Median) | 96 | 65 | 0.023 | 100 | 60 | 0.001 |
| ALT (IU/L) (Median) | 72 | 51 | 0.071 | 85 | 44 | <0.001 |
| ALB (g/L) | 38.42 ± 7.51 | 39.21 ± 5.63 | 0.080 | 38.46 ± 6.56 | 39.62 ± 5.63 | 0.003 |
| PT (s) | 12.87 ± 2.35 | 12.71 ± 2.30 | 0.362 | 12.84 ± 2.19 | 12.65 ± 2.44 | 0.177 |
| HBV-DNA levels (>2 × 103 IU/mL × 103 IU/mL) | 194/58 | 341/427 | <0.001 | - | - | - |
| HBeAg (+)/HBeAg (−) | - | - | - | 194/341 | 58/427 | <0.001 |
| CHB | |||||
|---|---|---|---|---|---|
| Variable | B | p | Exp(B) | Exp(B) 95% CI | |
| Down | Up | ||||
| ALT | 0.004 | 0.002 | 1.004 | 1.002 | 1.007 |
| ALB | −0.029 | 0.010 | 0.971 | 0.950 | 0.993 |
| HBeAg (+) | 1.412 | <0.001 | 4.104 | 2.941 | 5.726 |
| Constant | 0.779 | 0.035 | 2.178 | - | - |
| HBeAg (+) | |||||
| HGB | −0.016 | 0.028 | 0.984 | 0.970 | 0.998 |
| HBeAg | 0.007 | 0.011 | 1.007 | 1.001 | 1.012 |
| Constant | 3.070 | 0.003 | 21.542 | - | - |
| HBeAg (−) | |||||
| TB | −0.006 | 0.008 | 0.994 | 0.989 | 0.998 |
| ALT | 0.005 | <0.001 | 1.005 | 1.003 | 1.008 |
| Constant | −0.385 | 0.001 | 0.680 | - | - |
| HBeAg (+) | HBeAg (−) | |||||||
|---|---|---|---|---|---|---|---|---|
| High HBV DNA | Low HBV DNA | p1 Value | Cut-Off Value | High HBV DNA | Low HBV DNA | p2 Value | Cut-Off Value | |
| Sex (male/female) | 172/22 | 51/7 | 0.879 | - | 302/49 | 356/71 | 0.305 | - |
| Age (years) | 46.82 ± 10.58 | 45.44 ± 9.93 | 0.378 | - | 52.46 ± 11.18 | 51.82 ± 12.7 | 0.463 | - |
| HGB (g/L) | 133.71 ± 23.94 | 142.09 ± 18.19 | 0.015 | 170.5 | 134.89 ± 22.27 | 134.93 ± 21.25 | 0.979 | - |
| PLT (×109/L) | 120.67 ± 72.38 | 124.53 ± 90.49 | 0.739 | - | 135.09 ± 69.37 | 145.36 ± 90.66 | 0.086 | - |
| WBC (×109/L) | 5.47 ± 3.28 | 5.52 ± 3.74 | 0.912 | - | 5.78 ± 3.19 | 6.00 ± 3.59 | 0.359 | - |
| TB (umol/L) | 27.51 ± 60.89 | 21.04 ± 15.67 | 0.425 | - | 20.71 ± 60.89 | 29.05 ± 62.12 | 0.026 | 11.15 |
| AST (IU/L) | 101.48 ± 141.86 | 73.78 ± 106.62 | 0.170 | - | 77.81 ± 85.51 | 64.13 ± 79.50 | 0.022 | 42.5 |
| ALT (IU/L) | 71.29 ± 95.64 | 60.36 ± 59.75 | 0.411 | - | 68.10 ± 64.78 | 52.00 ± 59.54 | 0.001 | 36.5 |
| ALB (g/L) | 37.88 ± 7.76 | 40.23 ± 6.37 | 0.036 | 25.0 | 38.79 ± 5.75 | 39.54 ± 5.52 | 0.068 | - |
| PT (s) | 12.98 ± 2.52 | 12.49 ± 1.62 | 0.173 | - | 12.77 ± 1.96 | 12.67 ± 2.53 | 0.556 | - |
| HBeAg levels (S/CO) | 138.00 ± 238.74 | 24.46 ± 132.97 | 0.001 | 16.15 | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, N.; Zheng, J.; Huang, Y.; Pu, X.; Jiang, L.; Yang, J. A Predictive Model to Evaluate the HbeAg Positivity of Chronic Hepatitis B Virus Patients in Clinics: A Cross-Sectional Study. Medicina 2022, 58, 1279. https://doi.org/10.3390/medicina58091279
Wang N, Zheng J, Huang Y, Pu X, Jiang L, Yang J. A Predictive Model to Evaluate the HbeAg Positivity of Chronic Hepatitis B Virus Patients in Clinics: A Cross-Sectional Study. Medicina. 2022; 58(9):1279. https://doi.org/10.3390/medicina58091279
Chicago/Turabian StyleWang, Ning, Jinli Zheng, Yang Huang, Xingyu Pu, Li Jiang, and Jiayin Yang. 2022. "A Predictive Model to Evaluate the HbeAg Positivity of Chronic Hepatitis B Virus Patients in Clinics: A Cross-Sectional Study" Medicina 58, no. 9: 1279. https://doi.org/10.3390/medicina58091279