
The Clinical Experience of Mycobacterial Culture Yield of Pleural Tissue by Pleuroscopic Pleural Biopsy among Tuberculous Pleurisy Patients
 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Diagnostic Criteria of TB Pleurisy
2.3. Procedure and Equipment
2.4. Specimen Processing
2.5. Drug Susceptibility Testing (DST)
2.6. Statistical Analysis
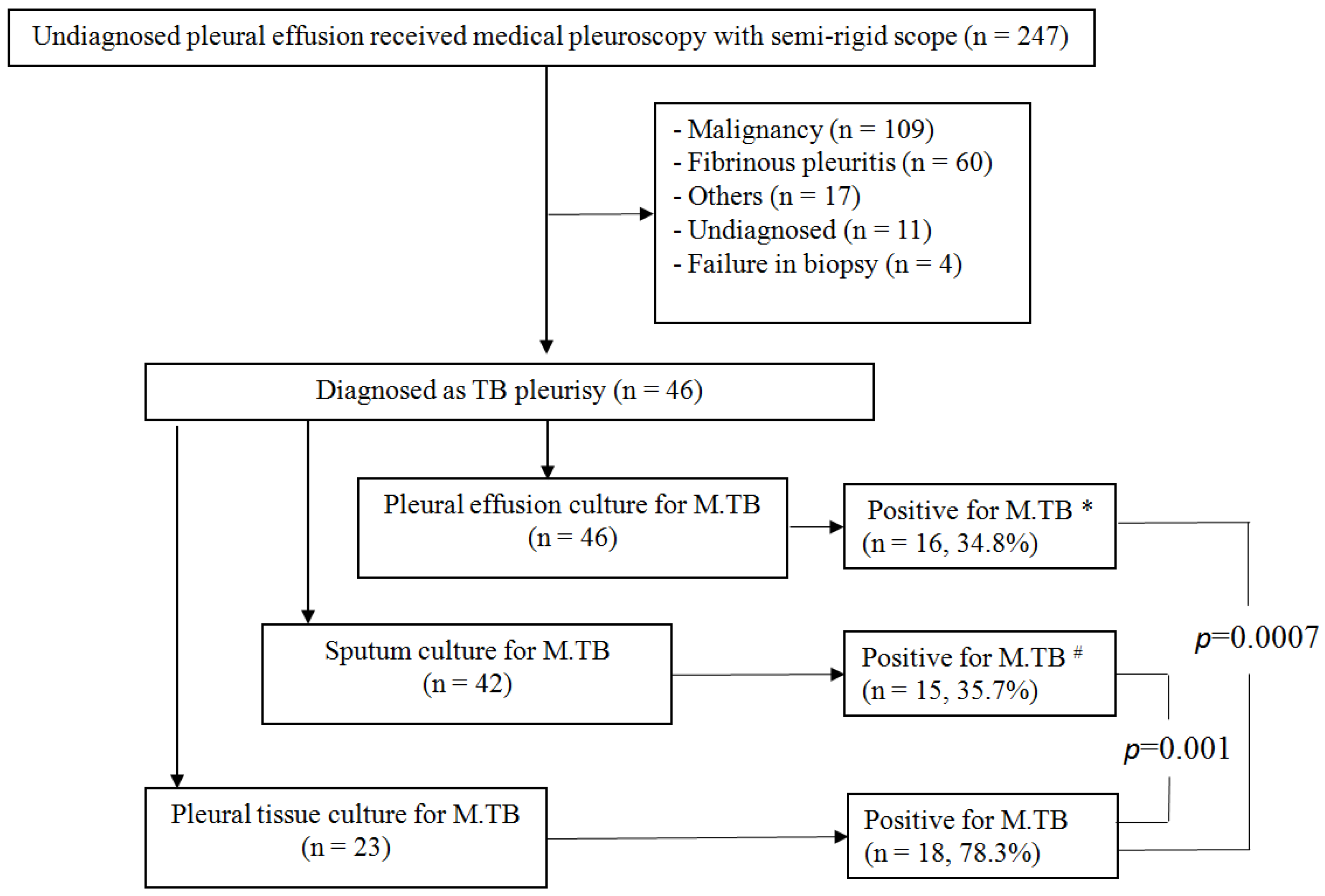
3. Results
3.1. TB Pleurisy Diagnosis by M. TB Cultures and Pathology Results
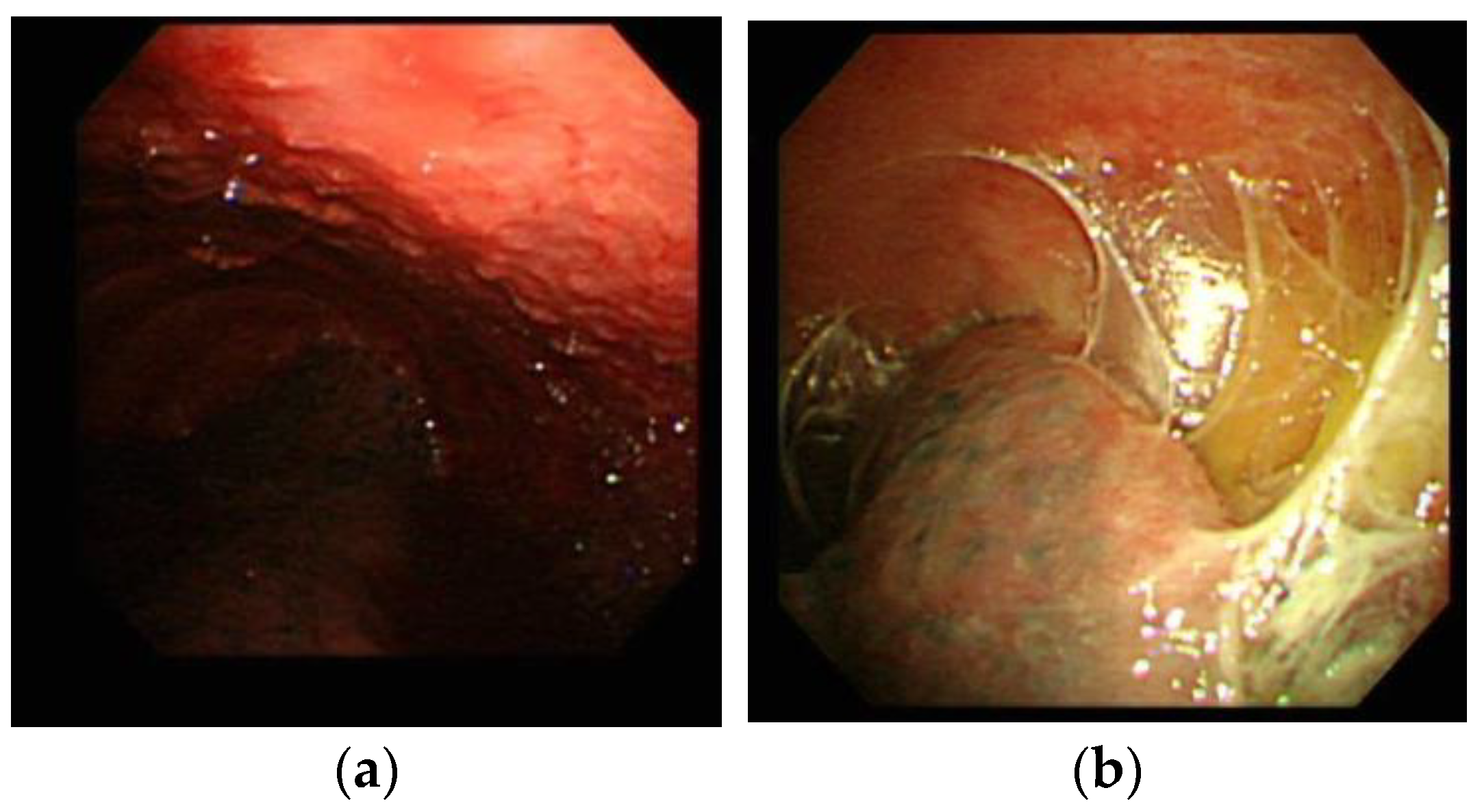
3.2. TB Pleurisy Diagnosis by M. TB Cultures and Pleuroscopic Features
3.3. Drug Sensitivity of Mycobacterial Cultures from Pleural Tissue
3.4. Complications and Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2021; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Lo, H.Y.; Yang, S.L.; Chou, P.; Chuang, J.H.; Chiang, C.Y. Completeness and timeliness of tuberculosis notification in Taiwan. BMC Public Health 2011, 11, 915. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Y.; Pan, S.W.; Shen, H.S.; Chuang, F.Y.; Feng, J.Y.; Su, W.J. Declining trend in incidence of tuberculosis in adolescents and young adults in Taiwan. Eur. Respir. J. 2019, 53, 1801305. [Google Scholar] [CrossRef] [PubMed]
- Light, R.W. Update on tuberculous pleural effusion. Respirology 2010, 15, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Ozvaran, M.K.; Baran, R.; Tor, M.; Dilek, I.; Demiryontar, D.; Arinç, S.; Toker, N.; Chousein, E.U.; Soğukpinar, Ö. Extrapulmonary tuberculosis in non-human immunodeficiency virus-infected adults in an endemic region. Ann. Thorac. Med. 2007, 2, 118–121. [Google Scholar] [CrossRef]
- Liam, C.K.; Lim, K.H.; Wong, C.M. Causes of pleural exudates in a region with a high incidence of tuberculosis. Respirology 2000, 5, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.S.; Li, S.H.; Chang, C.H.; Chung, F.T.; Chiu, L.C.; Chou, C.L.; Wang, C.W.; Lin, S.M. Diagnosis of tuberculosis pleurisy with three endoscopic features via pleuroscopy. Ther. Adv. Respir. Dis. 2021, 15, 1753466621989532. [Google Scholar] [CrossRef]
- Light, R.W. Useful tests on the pleural fluid in the management of patients with pleural effusions. Curr. Opin. Pulm. Med. 1999, 5, 245–249. [Google Scholar] [CrossRef]
- Bueno, C.E.; Clemente, M.G.; Castro, B.C.; Martín, L.M.; Ramos, S.R.; Panizo, A.G.; Glez-Río, J.M. Cytologic and bacteriologic analysis of fluid and pleural biopsy specimens with Cope’s needle. Study of 414 patients. Arch. Intern. Med. 1990, 150, 1190–1194. [Google Scholar] [CrossRef]
- Seibert, A.F.; Haynes, J., Jr.; Middleton, R.; Bass, J.B., Jr. Tuberculous pleural effusion. Twenty-year experience. Chest 1991, 99, 883–886. [Google Scholar] [CrossRef]
- Lin, C.M.; Lin, S.M.; Chung, F.T.; Lin, H.C.; Lee, K.Y.; Huang, C.D.; Kuo, C.H.; Liu, C.Y.; Wang, C.H.; Kuo, H.P. Amplified Mycobacterium tuberculosis direct test for diagnosing tuberculous pleurisy—A diagnostic accuracy study. PLoS ONE 2012, 7, e44842. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.; Wei, J.; Yu, D. Application of NGS in Diagnosis of Tuberculous Pleurisy with Multiple Negative Tests: A Case Report. Infect. Drug Resist. 2020, 13, 3543–3550. [Google Scholar] [CrossRef]
- Dohál, M.; Dvořáková, V.; Šperková, M.; Pinková, M.; Spitaleri, A.; Norman, A.; Cabibbe, A.M.; Rasmussen, E.M.; Porvazník, I.; Škereňová, M.; et al. Whole genome sequencing of multidrug-resistant Mycobacterium tuberculosis isolates collected in the Czech Republic, 2005–2020. Sci. Rep. 2022, 12, 7149. [Google Scholar] [CrossRef] [PubMed]
- Sharma, K.; Verma, R.; Advani, J.; Chatterjee, O.; Solanki, H.S.; Sharma, A.; Varma, S.; Modi, M.; Ray, P.; Mukherjee, K.K.; et al. Whole Genome Sequencing of Mycobacterium tuberculosis Isolates From Extrapulmonary Sites. OMICS 2017, 21, 413–425. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.S.; Li, S.H.; Chang, C.H.; Chung, F.T.; Chiu, L.C.; Chou, C.L.; Wang, C.W.; Lin, S.M. Comparison of Diagnostic Yield and Safety between Semirigid Pleuroscopic Cryobiopsy and Forceps Biopsy for Undiagnosed Pleural Effusion. Can. Respir. J. 2019, 2019, 5490896. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.Y.; Lin, S.M.; Shie, S.S.; Chou, P.C.; Huang, C.D.; Chung, F.T.; Kuo, C.H.; Chang, P.J.; Kuo, H.P. Clinical characteristics and treatment outcomes of patients with low- and high-concentration isoniazid-monoresistant tuberculosis. PLoS ONE 2014, 9, e86316. [Google Scholar] [CrossRef]
- Moon, J.W.; Chang, Y.S.; Kim, S.K.; Kim, Y.S.; Lee, H.M.; Kim, S.K.; Chang, J. The clinical utility of polymerase chain reaction for the diagnosis of pleural tuberculosis. Clin. Infect. Dis. 2005, 41, 660–666. [Google Scholar] [CrossRef]
- Antoniskis, D.; Amin, K.; Barnes, P.F. Pleuritis as a manifestation of reactivation tuberculosis. Am. J. Med. 1990, 89, 447–450. [Google Scholar] [CrossRef]
- Lin, S.M.; Ni, Y.L.; Kuo, C.H.; Lin, T.Y.; Wang, T.Y.; Chung, F.T.; Kuo, H.P. Endobronchial ultrasound increases the diagnostic yields of polymerase chain reaction and smear for pulmonary tuberculosis. J. Thorac. Cardiovasc. Surg. 2010, 139, 1554–1560. [Google Scholar] [CrossRef]
- Harris, R.C.; Grandjean, L.; Martin, L.J.; Miller, A.J.; Nkang, J.E.; Allen, V.; Khan, M.S.; Fielding, K.; Moore, D.A. The effect of early versus late treatment initiation after diagnosis on the outcomes of patients treated for multidrug-resistant tuberculosis: A systematic review. BMC Infect. Dis. 2016, 16, 193. [Google Scholar] [CrossRef]
- Lin, Y.; Enarson, D.A.; Du, J.; Dlodlo, R.A.; Chiang, C.Y.; Rusen, I.D. Risk factors for unfavourable treatment outcome among new smear-positive pulmonary tuberculosis cases in China. Public Health Action 2017, 7, 299–303. [Google Scholar] [CrossRef] [Green Version]
- Lin, M.T.; Wang, J.Y.; Yu, C.J.; Lee, L.N.; Yang, P.C. Mycobacterium tuberculosis and polymorphonuclear pleural effusion: Incidence and clinical pointers. Respir. Med. 2009, 103, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Burgess, L.J.; Maritz, F.J.; Le Roux, I.; Taljaard, J.J. Combined use of pleural adenosine deaminase with lymphocyte/neutrophil ratio. Increased specificity for the diagnosis of tuberculous pleuritis. Chest 1996, 109, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Neves, D.D.; Dias, R.M.; Cunha, A.J. Predictive model for the diagnosis of tuberculous pleural effusion. Braz. J. Infect. Dis. 2007, 11, 83–88. [Google Scholar] [CrossRef]
- Christopher, D.J.; Dinakaran, S.; Gupta, R.; James, P.; Isaac, B.; Thangakunam, B. Thoracoscopic pleural biopsy improves yield of Xpert MTB/RIF for diagnosis of pleural tuberculosis. Respirology 2018, 23, 714–717. [Google Scholar] [CrossRef]
- Gao, S.; Wang, C.; Yu, X.; Teng, T.; Shang, Y.; Jia, J.; Dong, L.; Zhao, L.; Liu, S.; Chu, N.; et al. Xpert MTB/RIF Ultra enhanced tuberculous pleurisy diagnosis for patients with unexplained exudative pleural effusion who underwent a pleural biopsy via thoracoscopy: A prospective cohort study. Int. J. Infect. Dis. 2021, 106, 370–375. [Google Scholar] [CrossRef]
- Pereyra, M.F.; San-José, E.; Ferreiro, L.; Golpe, A.; Antúnez, J.; González-Barcala, F.J.; Abdulkader, I.; Álvarez-Dobaño, J.M.; Rodríguez-Núñez, N.; Valdés, L. Role of blind closed pleural biopsy in the managment of pleural exudates. Can. Respir. J. 2013, 20, 362–366. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.; Ibrahim, W.H.; Raza, T.; Mushtaq, K.; Arshad, A.; Ahmed, M.; Taha, S.; Al Sarafandi, S.; Karim, H.; Abdul-Sattar, H.A. Medical thoracoscopy for exudative pleural effusion: An eight-year experience from a country with a young population. BMC Pulm. Med. 2017, 17, 151. [Google Scholar] [CrossRef]
- Pablos-Mendez, A.; Raviglione, M.C.; Laszlo, A.; Binkin, N.; Rieder, H.L.; Bustreo, F.; Cohn, D.L.; Lambregts-van Weezenbeek, C.S.; Kim, S.J.; Chaulet, P.; et al. Global surveillance for antituberculosis-drug resistance, 1994–1997. World Health Organization-International Union against Tuberculosis and Lung Disease Working Group on Anti-Tuberculosis Drug Resistance Surveillance. N. Engl. J. Med. 1998, 338, 1641–1649. [Google Scholar]
- Espinal, M.A.; Laszlo, A.; Simonsen, L.; Boulahbal, F.; Kim, S.J.; Reniero, A.; Hoffner, S.; Rieder, H.L.; Binkin, N.; Dye, C.; et al. Global trends in resistance to antituberculosis drugs. World Health Organization-International Union against Tuberculosis and Lung Disease Working Group on Anti-Tuberculosis Drug Resistance Surveillance. N. Engl. J. Med. 2001, 344, 1294–1303. [Google Scholar] [CrossRef]
- Cattamanchi, A.; Dantes, R.B.; Metcalfe, J.Z.; Jarlsberg, L.G.; Grinsdale, J.; Kawamura, L.M.; Osmond, D.; Hopewell, P.C.; Nahid, P. Clinical characteristics and treatment outcomes of patients with isoniazid-monoresistant tuberculosis. Clin. Infect. Dis. 2009, 48, 179–185. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Total n = 46 |
|---|---|
| Age, median (IQR) | 62.5 (20.4–92.0) |
| Male Gender | 30 (65.2%) |
| Smoking status | |
| Current smoker | 3 (6.5%) |
| Prior smoker | 11 (23.9%) |
| Never smoker | 32 (69.6%) |
| Location of pleural effusion | |
| Right | 28 (60.9%) |
| Left | 13 (28.3%) |
| Bilateral | 5 (10.9%) |
| Pleural effusion lymphocyte percentage (%), median (IQR) * | 87.5% (76.0–95.0%) |
| Pleural effusion LDH (mg/dL), median (IQR) | 309 (229.5–405.5) |
| Pleural effusion total protein (mg/dL), median (IQR) | 5.05 (4.2–5.4) |
| Serum LDH (mg/dL), median (IQR) | 199 (178–249) |
| Serum total protein (mg/dL), median (IQR) | 6.95 (6.5–7.7) |
| Pleural effusion/Serum LDH ratio | 1.40 ± 0.54 |
| Pleural effusion/Serum total protein ratio | 0.68 ± 0.11 |
| Pathology Results | Positive Mycobacterial Culture in | ||
|---|---|---|---|
| Sputum n = 15 | Pleural Fluid n = 16 | Pleural Tissue Biopsy * n = 18 | |
| Acid-fast bacillus in specimens | 1 (6.7%) | 1 (6.3%) | 0 (0.0%) |
| Epithelioid cell granuloma | 8 (53.3%) | 6 (37.5%) | 6 (33.3%) |
| Caseous granuloma + epithelioid cell granuloma | 7 (46.7%) | 10 (62.5%) | 10 (55.6%) |
| Visual Characteristic by Pleuroscopy | Positive Mycobacterial Cultures/Features under Pleuroscope | ||
|---|---|---|---|
| Sputum | Pleural Fluid | Pleural Tissue Biopsy | |
| With micronodules | 10/32 (31.3%) | 10/34 (29.4%) | 12/17 (70.6%) |
| With adhesion lesions | 11/31 (48.0%) | 14/33 (42.4%) | 17/18 (94.4%) |
| With combination of micronodules and adhesion lesions | 6/22 (27.3%) | 8/22 (36.4%) | 11/12 (91.7%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.-S.; Chiu, L.-C.; Chang, C.-H.; Chung, F.-T.; Li, S.-H.; Chou, C.-L.; Wang, C.-W.; Lin, S.-M. The Clinical Experience of Mycobacterial Culture Yield of Pleural Tissue by Pleuroscopic Pleural Biopsy among Tuberculous Pleurisy Patients. Medicina 2022, 58, 1280. https://doi.org/10.3390/medicina58091280
Lee C-S, Chiu L-C, Chang C-H, Chung F-T, Li S-H, Chou C-L, Wang C-W, Lin S-M. The Clinical Experience of Mycobacterial Culture Yield of Pleural Tissue by Pleuroscopic Pleural Biopsy among Tuberculous Pleurisy Patients. Medicina. 2022; 58(9):1280. https://doi.org/10.3390/medicina58091280
Chicago/Turabian StyleLee, Chung-Shu, Li-Chung Chiu, Chih-Hao Chang, Fu-Tsai Chung, Shih-Hong Li, Chun-Liang Chou, Chih-Wei Wang, and Shu-Min Lin. 2022. "The Clinical Experience of Mycobacterial Culture Yield of Pleural Tissue by Pleuroscopic Pleural Biopsy among Tuberculous Pleurisy Patients" Medicina 58, no. 9: 1280. https://doi.org/10.3390/medicina58091280