
Outcomes in Hybrid Breast Reconstruction: A Systematic Review

 ,
, 
Abstract
:1. Introduction
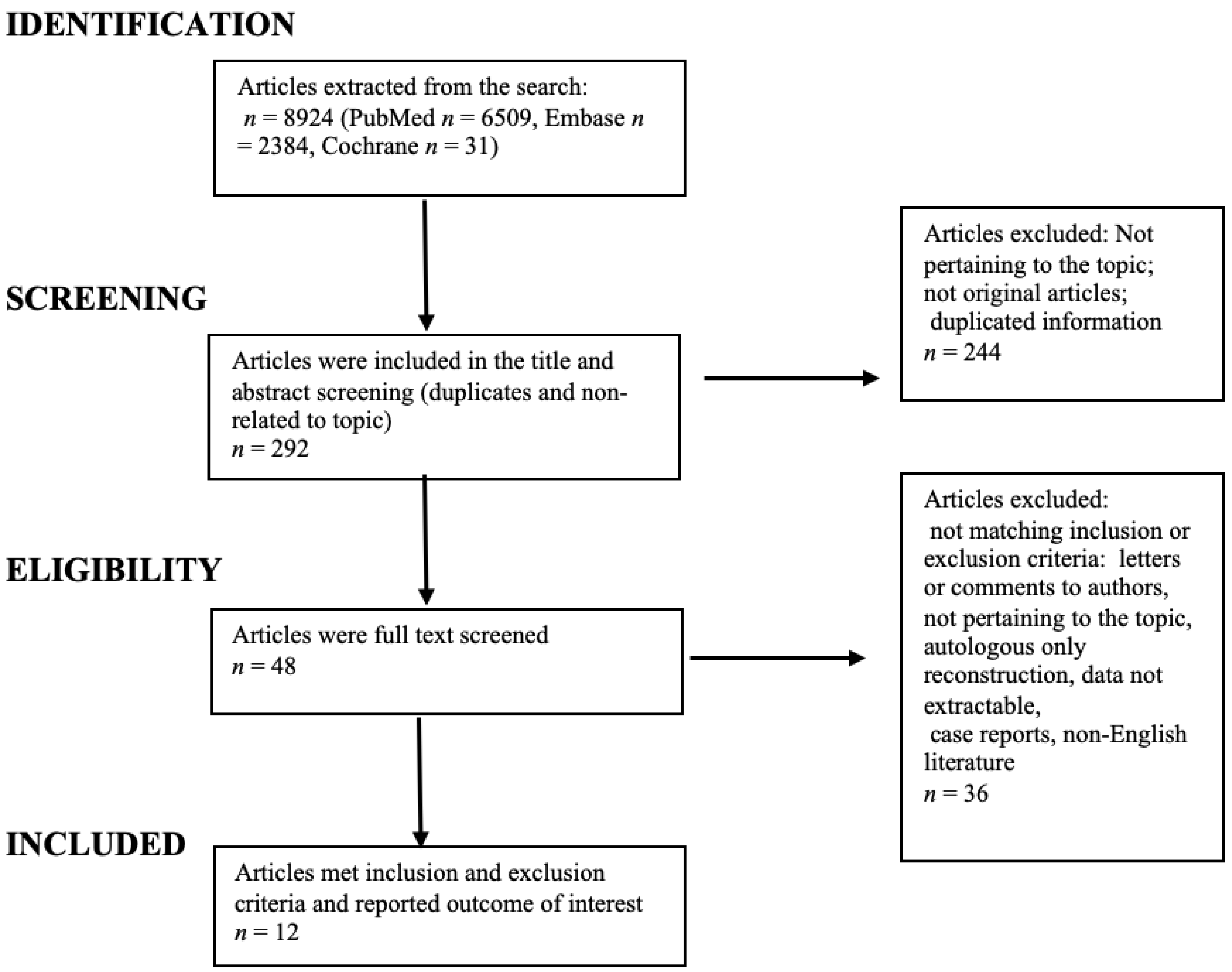
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, J.; Chan, P.S.; Lok, V.; Chen, X.; Ding, H.; Jin, Y.; Yuan, J.; Lao, X.Q.; Zheng, Z.J.; Wong, M.C. Global incidence and mortality of breast cancer: A trend analysis. Aging 2021, 13, 5748–5803. [Google Scholar] [CrossRef] [PubMed]
- Ilonzo, N.; Tsang, A.; Tsantes, S.; Estabrook, A.; Ma, A.M.T. Breast reconstruction after mastectomy: A ten-year analysis of trends and immediate postoperative outcomes. Breast 2017, 32, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Herly, M.; Ørholt, M.; Larsen, A.; Pipper, C.B.; Bredgaard, R.; Gramkow, C.S.; Katz, A.J.; Drzewiecki, K.T.; Vester-Glowinski, P.V. Efficacy of breast reconstruction with fat grafting: A systematic review and meta-analysis. J. Plast. Reconstr. Aesthet. Surg. 2018, 71, 1740–1750. [Google Scholar] [CrossRef] [PubMed]
- Ejaz, A.; Yang, K.S.; Venkatesh, K.P.; Chinnapaka, S.; Kokai, L.E.; Rubin, J.P. The Impact of Human Lipoaspirate and Adipose Tissue-Derived Stem Cells Contact Culture on Breast Cancer Cells: Implications in Breast Reconstruction. Int. J. Mol. Sci. 2020, 21, 9171. [Google Scholar] [CrossRef] [PubMed]
- Casarrubios, J.M.; Francés, M.; Fuertes, V.; Singer, M.; Navarro, C.; García-Duque, O.; Fernández-Palacios, J. Oncological outcomes of lipofilling in breast reconstruction: A matched cohort study with 250 patients. Gland. Surg. 2021, 10, 914–923. [Google Scholar] [CrossRef] [PubMed]
- Shamoun, F.; Asaad, M.; Hanson, S.E. Oncologic Safety of Autologous Fat Grafting in Breast Reconstruction. Clin. Breast Cancer 2021, 21, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Waked, K.; Colle, J.; Doornaert, M.; Cocquyt, V.; Blondeel, P. Systematic review: The oncological safety of adipose fat transfer after breast cancer surgery. Breast 2017, 31, 128–136. [Google Scholar] [CrossRef]
- Stumpf, C.C.; Zucatto, Â.E.; Cavalheiro, J.A.C.; de Melo, M.P.; Cericato, R.; Damin, A.P.S.; Biazús, J.V. Oncologic safety of immediate autologous fat grafting for reconstruction in breast-conserving surgery. Breast Cancer Res. Treat. 2020, 180, 301–309. [Google Scholar] [CrossRef]
- Kenny, E.M.; Egro, F.M.; Ejaz, A.; Coleman, S.R.; Greenberger, J.S.; Rubin, J.P. Fat Grafting in Radiation-Induced Soft-Tissue Injury: A Narrative Review of the Clinical Evidence and Implications for Future Studies. Plast. Reconstr. Surg. 2021, 147, 819–838. [Google Scholar] [CrossRef]
- Alessandri-Bonetti, M.; Egro, F.M.; Persichetti, P.; Coleman, S.R.; Rubin, J.P. The Role of Fat Grafting in Alleviating Neuropathic Pain: A Critical Review of the Literature. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2216. [Google Scholar] [CrossRef]
- Gronovich, Y.; Winder, G.; Maisel-Lotan, A.; Lysy, I.; Sela, E.; Spiegel, G.; Carmon, M.; Hadar, T.; Elami, A.; Eizenman, N.; et al. Hybrid Prepectoral Direct-to-Implant and Autologous Fat Graft Simultaneously in Immediate Breast Reconstruction: A Single Surgeon’s Experience with 25 Breasts in 15 Consecutive Cases. Plast. Reconstr. Surg. 2022, 149, 386e–391e. [Google Scholar] [CrossRef]
- Auclair, E.; Anavekar, N. Combined Use of Implant and Fat Grafting for Breast Augmentation. Clin. Plast. Surg. 2015, 42, 307–314. [Google Scholar] [CrossRef]
- Gronovich, Y.; Winder, G.; Maisel-Lotan, A.; Lysy, I.; Sela, E.; Spiegel, G.; Carmon, M.; Hadar, T.; Elami, A.; Eizenman, N.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar]
- Sommeling, C.E.; Van Landuyt, K.; Depypere, H.; Van den Broecke, R.; Monstrey, S.; Blondeel, P.N.; Morrison, W.A.; Stillaert, F.B. Composite breast reconstruction: Implant-based breast reconstruction with adjunctive lipofilling. J. Plast. Reconstr. Aesthet. Surg. 2017, 70, 1051–1058. [Google Scholar] [CrossRef]
- Razzouk, K.; Humbert, P.; Borens, B.; Gozzi, M.; Al Khori, N.; Pasquier, J.; Rafii Tabrizi, A. Skin trophicity improvement by mechanotherapy for lipofilling-based breast reconstruction postradiation therapy. Breast J. 2020, 26, 725–728. [Google Scholar] [CrossRef]
- Razzouk, K.; Fitoussi, A.; Al Khori, N.; Pasquier, J.; Chouchane, L.; Tabrizi, A.R. Breast Reconstruction Combining Lipofilling and Prepectoral Prosthesis after Radiotherapy. Plast. Reconstr. Surg. Glob. Open 2020, 26, e2659. [Google Scholar] [CrossRef]
- Salgarello, M.; Visconti, G.; Barone-Adesi, L. Fat grafting and breast reconstruction with implant: Another option for irradiated breast cancer patients. Plast. Reconstr. Surg. 2012, 129, 317–329. [Google Scholar] [CrossRef]
- Hammond, D.C.; O’Connor, E.A.; Scheer, J.R. Total envelope fat grafting: A novel approach in breast reconstruction. Plast. Reconstr. Surg. 2015, 135, 691–694. [Google Scholar] [CrossRef]
- Sarfati, I.; Ihrai, T.; Kaufman, G.; Nos, C.; Clough, K.B. Adipose-tissue grafting to the post-mastectomy irradiated chest wall: Preparing the ground for implant reconstruction. J. Plast. Reconstr. Aesthet. Surg. 2011, 64, 1161–1166. [Google Scholar] [CrossRef]
- Serra-Renom, J.M.; Muñoz-Olmo, J.L.; Serra-Mestre, J.M. Fat grafting in postmastectomy breast reconstruction with expanders and prostheses in patients who have received radiotherapy: Formation of new subcutaneous tissue. Plast. Reconstr. Surg. 2010, 125, 12–18. [Google Scholar] [CrossRef]
- Stillaert, F.B.J.L.; Lannau, B.; Van Landuyt, K.; Blondeel, P.N. The Prepectoral, Hybrid Breast Reconstruction: The Synergy of Lipofilling and Breast Implants. Plast. Reconstr. Surg. Glob. Open 2020, 23, e2966. [Google Scholar] [CrossRef] [PubMed]
- Cogliandro, A.; Barone, M.; Tenna, S.; Morelli Coppola, M.; Persichetti, P. The Role of Lipofilling After Breast Reconstruction: Evaluation of Outcomes and Patient Satisfaction with BREAST-Q. Aesthetic Plast Surg. 2017, 41, 1325–1331. [Google Scholar] [CrossRef]
- Patel, A.A.; Martin, S.A.; Cheesborough, J.E.; Lee, G.K.; Nazerali, R.S. The safety and efficacy of autologous fat grafting during second stage breast reconstruction. J. Plast. Reconstr. Aesthet. Surg. 2021, 74, 792–799. [Google Scholar] [CrossRef] [PubMed]
- Cigna, E.; Ribuffo, D.; Sorvillo, V.; Atzeni, M.; Piperno, A.; Calò, P.G.; Scuderi, N. Secondary lipofilling after breast reconstruction with implants. Eur. Rev. Med. Pharmacol. Sci. 2012, 16, 1729–1734. [Google Scholar] [PubMed]
- Persichetti, P.; Barone, M.; Salzillo, R.; Cogliandro, A.; Brunetti, B.; Ciarrocchi, S.; Bonetti, M.A.; Tenna, S.; Sorotos, M.; Di Pompeo, F.S. Impact on Patient’s Appearance Perception of Autologous and Implant Based Breast Reconstruction Following Mastectomy Using BREAST-Q. Aesth. Plast. Surg. 2022, in press. [Google Scholar] [CrossRef]
- Toyserkani, N.M.; Jørgensen, M.G.; Tabatabaeifar, S.; Damsgaard, T.; Sørensen, J.A. Autologous versus implant-based breast reconstruction: A systematic review and meta-analysis of Breast-Q patient-reported outcomes. J. Plast. Reconstr. Aesthet. Surg. 2020, 73, 278–285. [Google Scholar] [CrossRef]
- Di Pompeo, F.S.; Barone, M.; Salzillo, R.; Cogliandro, A.; Brunetti, B.; Ciarrocchi, S.; Alessandri Bonetti, M.; Tenna, S.; Sorotos, M.; Persichetti, P. Predictive Factors of Satisfaction Following Breast Reconstruction: Do they Influence Patients? Aesth. Plast. Surg. 2022, 46, 610–618. [Google Scholar] [CrossRef]
- Albornoz, C.R.; Bach, P.B.; Mehrara, B.J.; Disa, J.J.; Pusic, A.L.; McCarthy, C.M.; Cordeiro, P.G.; Matros, E. A paradigm shift in U.S. Breast reconstruction: Increasing implant rates. Plast. Reconstr. Surg. 2013, 131, 15–23. [Google Scholar] [CrossRef]
- Krueger, E.A.; Wilkins, E.G.; Strawderman, M.; Cederna, P.; Goldfarb, S.; Vicini, F.A.; Pierce, L.J. Complications and patient satisfaction following expander/implant breast reconstruction with and without radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2001, 49, 713–721. [Google Scholar] [CrossRef]
- Jhaveri, J.D.; Rush, S.C.; Kostroff, K.; Derisi, D.; Farber, L.A.; Maurer, V.E.; Bosworth, J.L. Clinical outcomes of postmastectomy radiation therapy after immediate breast reconstruction. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 859–865. [Google Scholar] [CrossRef]
- Lipa, J.E.; Qiu, W.; Huang, N.; Alman, B.A.; Pang, C.Y. Pathogenesis of radiation-induced capsular contracture in tissue expander and implant breast reconstruction. Plast. Reconstr. Surg. 2010, 125, 437–445. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, S.R.; Fletcher, D.R.D.; Isom, C.D.; Isik, F.F. True incidence of all complications following immediate and delayed breast reconstruction. Plast. Reconstr. Surg. 2008, 122, 19–28. [Google Scholar] [CrossRef]
- Tallet, A.V.; Salem, N.; Moutardier, V.; Ananian, P.; Braud, A.C.; Zalta, R.; Cowen, D.; Houvenaeghel, G. Radiotherapy and immediate two-stage breast reconstruction with a tissue expander and implant: Complications and esthetic results. Int. J. Radiat. Oncol. Biol. Phys. 2003, 57, 136–142. [Google Scholar] [CrossRef]
- Benediktsson, K.; Perbeck, L. Capsular contracture around saline-filled and textured subcutaneously-placed implants in irradiated and non-irradiated breast cancer patients: Five years of monitoring of a prospective trial. J. Plast. Reconstr. Aesthet. Surg. 2006, 59, 27–34. [Google Scholar] [CrossRef]
- Behranwala, K.A.; Dua, R.S.; Ross, G.M.; Ward, A.; A’hern, R.; Gui, G.P. The influence of radiotherapy on capsule formation and aesthetic outcome after immediate breast reconstruction using biodimensional anatomical expander implants. J. Plast. Reconstr. Aesthet. Surg. 2006, 59, 1043–1051. [Google Scholar] [CrossRef]
- Debald, M.; Pech, T.; Kaiser, C.; Keyver-Paik, M.D.; Walgenbach-Bruenagel, G.; Kalff, J.C.; Kuhn, W.; Walgenbach, K.J. Lipofilling effects after breast cancer surgery in post-radiation patients: An analysis of results and algorithm proposal. Eur. J. Plast. Surg. 2017, 40, 447–454. [Google Scholar] [CrossRef]
- Ribuffo, D.; Atzeni, M.; Guerra, M.; Bucher, S.; Politi, C.; Deidda, M.; Atzori, F.; Dessi, M.; Madeddu, C.; Lay, G. Treatment of irradiated expanders: Protective lipofilling allows immediate prosthetic breast reconstruction in the setting of postoperative radiotherapy. Aesth. Plast. Surg. 2013, 37, 1146–1152. [Google Scholar] [CrossRef]
- De Blacam, C.; Momoh, A.O.; Colakoglu, S.; Tobias, A.M.; Lee, B.T. Evaluation of clinical outcomes and aesthetic results after autologous fat grafting for contour deformities of the reconstructed breast. Plast. Reconstr. Surg. 2011, 128, 411e–418e. [Google Scholar] [CrossRef]
- Rigotti, G.; Marchi, A.; Galiè, M.; Baroni, G.; Benati, D.; Krampera, M.; Pasini, A.; Sbarbati, A. Clinical treatment of radiotherapy tissue damage by lipoaspirate transplant: A healing process mediated by adipose-derived adult stem cells. Plast. Reconstr. Surg. 2007, 119, 1409–1422. [Google Scholar] [CrossRef]
- De Lorenzi, F.; Borelli, F.; Sala, P.; Loschi, P.; Naninato, P.; Vento, A.R.; Rossi, E.M.C.; Veronesi, P. Multistage Latissimus Dorsi Flap with Implant for Complex Post-Mastectomy Reconstruction: An Old but Still Current Technique. Breast Care. 2021, 16, 396–401. [Google Scholar] [CrossRef]
- Kim, H.Y.; Jung, B.K.; Lew, D.H.; Lee, D.W. Autologous Fat Graft in the Reconstructed Breast: Fat Absorption Rate and Safety based on Sonographic Identification. Arch. Plast. Surg. 2014, 41, 740–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caviggioli, F.; Maione, L.; Klinger, F.; Lisa, A.; Klinger, M. Autologous Fat Grafting Reduces Pain in Irradiated Breast: A Review of Our Experience. Stem. Cells. Int. 2016, 2016, 2527349. [Google Scholar] [CrossRef] [PubMed]
- Tukiama, R.; Vieira, R.A.C.; Moura, E.C.R.; Oliveira, A.G.C.; Facina, G.; Zucca-Matthes, G.; Neto, J.N.; de Oliveira, C.M.B.; Leal, P.D.C. Oncologic safety of breast reconstruction with autologous fat grafting: A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2022, 48, 727–735. [Google Scholar] [CrossRef] [PubMed]
- Piccotti, F.; Rybinska, I.; Scoccia, E.; Morasso, C.; Ricciardi, A.; Signati, L.; Triulzi, T.; Corsi, F.; Truffi, M. Lipofilling in Breast Oncological Surgery: A Safe Opportunity or Risk for Cancer Recurrence? Int. J. Mol. Sci. 2021, 22, 3737. [Google Scholar] [CrossRef]
- Li, M.; Shi, Y.; Li, Q.; Guo, X.; Han, X.; Li, F. Oncological Safety of Autologous Fat Grafting in Breast Reconstruction: A Meta-analysis Based on Matched Cohort Studies. Aesth. Plast. Surg. 2022, in press. [Google Scholar] [CrossRef]
- Silva, M.M.A.; Kokai, L.E.; Donnenberg, V.S.; Fine, J.L.; Marra, K.G.; Donnenberg, A.D.; Neto, M.S.; Rubin, J.P. Oncologic Safety of Fat Grafting for Autologous Breast Reconstruction in an Animal Model of Residual Breast Cancer. Plast. Reconstr. Surg. 2019, 143, 103–112. [Google Scholar] [CrossRef]
- Vaienti, L.; Amendola, F.; Borelli, F.; Zaccaria, G.; Cottone, G. Perineural fat grafting in end-neuroma pain treatment: Long-term outcomes. Eur. J. Plast. Surg. 2020, 44, 249–254. [Google Scholar] [CrossRef]
- Herly, M.; Ørholt, M.; Glovinski, P.V.; Pipper, C.B.; Broholm, H.; Poulsgaard, L.; Fugleholm, K.; Thomsen, C.; Drzewiecki, K.T. Quantifying Long-Term Retention of Excised Fat Grafts: A Longitudinal, Retrospective Cohort Study of 108 Patients Followed for Up to 8.4 Years. Plast. Reconstr. Surg. 2017, 139, 1223–1232. [Google Scholar] [CrossRef]
- Papadopoulos, S.; Vidovic, G.; Neid, M.; Abdallah, A. Using Fat Grafting to Treat Breast Implant Capsular Contracture. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1969. [Google Scholar] [CrossRef]
- Komorowska-Timek, E.; Jaźwiec, A.; Adams, N.S.; Fahrenkopf, M.P.; Davis, A.T. Peri-prosthetic Fat Grafting Decreases Collagen Content, Density, and Fiber Alignment of Implant Capsules. Plast. Reconstr. Surg. Glob. Open 2021, 9, e3687. [Google Scholar] [CrossRef]
- Pagliara, D.; Vitagliano, S.; Mangialardi, M.L.; Pino, V.; Santoro, A.; Mulè, A.; Barone Adesi, L.; Salgarello, M. The role of fat grafting on contracted breast implant capsules: A retrospective comparative histological and immunohistochemical study. J. Plast. Reconstr. Aesthet. Surg. 2022, 75, 1083–1093. [Google Scholar] [CrossRef]
- Calabrese, S.; Zingaretti, N.; De Francesco, F.; Riccio, M.; De Biasio, F.; Massarut, S.; Almesberger, D.; Parodi, P.C. Long-term impact of lipofilling in hybrid breast reconstruction: Retrospective analysis of two cohorts. Eur. J. Plast. Surg 2020, 43, 257–268. [Google Scholar] [CrossRef]
- Calabrese, S.; Zingaretti, N.; Zanin, C.; Fin, A.; Mura, S.; Parodi, P. Hybrid Breast Reconstruction: Preliminary Report. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1660. [Google Scholar] [CrossRef]
- Crawford, K.; Endara, M. Lipotransfer strategies and techniques to achieve successful breast reconstruction in the radiated breast. Medicina 2022, 56, 516. [Google Scholar] [CrossRef]
- Schop, S.J.; Joosen, M.E.M.; Wolswijk, T.; Heuts, E.M.; van der Hulst, R.R.W.J.; Piatkowski de Grzymala, A.A. Quality of life after autologous fat transfer additional to prosthetic breast reconstruction in women after breast surgery: A systematic review. Eur. J. Surg. Oncol. 2021, 47, 772–777. [Google Scholar] [CrossRef]
- Hammond, J.B.; Kosiorek, H.E.; Cronin, P.A.; Rebecca, A.M.; Casey, W.J., 3rd; Wong, W.W.; Vargas, C.E.; Vern-Gross, T.Z.; McGee, L.A.; Pockaj, B.A. Capsular contracture in the modern era: A multidisciplinary look at the incidence and risk factors after mastectomy and implant-based breast reconstruction. Am. J. Surg. 2021, 221, 1005–1010. [Google Scholar] [CrossRef]


{kind=link}
| Authors | Type of Study | N pts | N Breasts | Age | Follow-Up (Months) | Demolitive Surgery | Reconstruction Modalities | RT |
|---|---|---|---|---|---|---|---|---|
| Stillaert FBJL et al. (2020) [21] | Case series (single surgeon’s experience) | 33 | 56 | 42 (21–77) | 24.1 | 36 prophylactic mastectomies brca, 7 mastectomies for breast ca, 13 secondary reconstructions | step1 te; step2 (8 weeks) fat grafting; step3 prepectoral implant | pmrt in 1/33 patients |
| Razzouk K et al. (2019) [15] | Case Series | 32 | 32 | 50.6 (9.7) | 22 | 32 radical mastectomies followed by pmrt | step1: lipofilling (3 months post rt), step2 prepectoral implant reconstruction | 32/32 pmrt |
| Sommeling CE et al. (2017) [14] | Case series | 15 | 23 | 46 (24–64) | 33 | 8pts (16) bilateral prophylactic mastectomies brca, 6 secondary reconstructions, 1 primary mastectomy | step 1: te, step 2 lipofilling (8 weeks post te or 6 months after pmrt in 6 pts), step3 prepectoral implant | 6/23 pmrt |
| Razzouk K et al. (2020) [16] | multicenter retrospective study (radical mastectomy) | 136 | 136 | 52 (33–72) | 32.4 | all modified radical mastectomies and external chest wall irradiation | step1: lipofilling (>3 months post rt), step2: prepectoral implant | 136/136 pmrt |
| Sarfati I et al. (2011) [19] | Case series (mastectomy + radiotherapy) | 28 | 28 | 45 (29–61) | 17 | all mastectomies for invasive breast ca and external chest wall rt | step1: lipofilling (>6, mean 9 months post rt), step2: (after mean 6.7 months.) dual plane implant reconstruction implant | 28/28 pmrt |
| Salgarello M et al. (2012) [17] | Case series (radiotherapy + implant based reconstruction) | 16 | 16 | 41 (29–58) | 23.6 | 5 quadrantectomy/lumpectomy 2 mastectomy and pmrt, 9 bresat conserving surgeryall underwent external chest irradiation | step 1: fat grafting (all > 6 months post rt) step 2: 5 bilateral breast aug dual plane11 implant-reconstruction dual plane | 16/16 pmrt |
| Serra-Renom JM et al. (2010) [20] | Case serie mastectomy + radiotherapy | 65 | 65 | 65 (34–62) | 6 | all mastectomies for invasive breast ca and external chest wall rt | step1: subpectoral te and fat grafting (>1 year after radiation)step2: implant reconstruction and fat grafting | 65/65 pmrt |
| Cigna E et al. (2012) [24] | Case series (nipple sparing) | 20 | 20 | 65 (29–72) | 12 | nipple sparing, skin sparing and skin reducing mastectomies. | step1 implant reconstructionstep 2 fat grafting | no pmrt |
| Cogliandro A et al. (2017) [22] | case-control (implant based vs hybrid reconstruction) | 46 | 46 | 41 (24–70) | 30 | mastectomy +/− external chest wall rt | step1 implant based reconstrction step 2 lipofilling (1 year after reconstruction) | 34/46 pmrt |
| Hammond DC (2015) [18] | Case series | 22 | 36 | 47 (29–66) | 11 | mastectomy | step 1: using te and adm step 2: fat grafting and implant | nd |
| Patel AA et al. (2020) [23] | Case-control (126 immediate FG, 31 delayed FG) | 157 (126 IFG,31 DFG) | 270 (225IFG) 45 (DFG) | 46.9/49.5 | 48.5 | ifg group (nsm 199, ssm 22 or modified rm 4)dfg goup (nsm 33, ssm 33, mrm 5) | 270 breasts implant based reconstruction and immediate fat grafting45 implant reconstruction and delayed fat grafting | ifg group 20 prior rt, 28 pmrtdfggroup 9 prior rt, 4 pmrt |
| Gronovich Y et al. (2021) [11] | case series single surgeon (prospective) | 15 | 25 | 44 (32–66) | 12 | mastectomywith immediate prepectoraldirect-to-implant (10 ssm 15 nsm) | all immediate implant based reconstruction with adm and immediate fat grafting | 4/25 pmrt |
| Authors | Timing of Fat Grafting | Technique | Mean Volume Per Session (mL) | Lipofilling Sessions Mean (Range) | Time between Sessions (Months) |
|---|---|---|---|---|---|
| Stillaert FBJL et al. (2020) [21] | 8 weeks after onset of Tissue Expansion (or 6 months after post mastectomy RT PMRT in 1 patient) | Coleman | 262 | 2.7 (1–5) | 3 |
| Razzouk K et al. (2019) [15] | >3 months after RT (all patients underwent PMRT) | The fat was then centrifuged 30 s at 3000 RPM | 151 | 1.15 (1–3) | ND |
| Sommeling CE et al. (2017) [14] | 8 weeks after onset of Tissue Expansion (or 6 months after PMRT in 6 patients) | Coleman | 313 | 3.2 (2–5) | 3 |
| Razzouk K et al. (2020) [16] | Average time between end of radiotherapy and first lipofilling was 19.6 months | Centrifuged 30 s at 3000 revolutions | 220 | 1.6 (1–3) | 3 |
| Sarfati I et al. (2011) [19] | Mean time was 9 months after radiotherapy.(all patients underwent PMRT) | Centrifuged speed of 3000 rpm for 3 min. | 115 | 2 (1–3) | Mean 3.3 range (1–14) |
| Salgarello M et al. (2012) [17] | At least 6 months after completion of PMRT and 3 months after mastectomy if previously irradiated. | Coleman | 95.7 | 2.4 (2–3) | >/=3 |
| Serra-Renom JM et al. (2010) [20] | at least 1 y after mastectomy + RT. (Implant reconstruction at same time of Fat grafting) | Coleman | 140 | 2.4 (1–4) | 3 |
| Cigna E. et al. (2012) [24] | ND | Coleman | ND | 1 | ND |
| Cogliandro A et al. (2017) [22] | 1 y after implant based reconstruction (34 patients had PMRT) | Coleman | 110 | 2.2 (1–3) | ND |
| Hammond DC (2015) [18] | Step 1: Using TE and ADM Step 2: Fatgrafting and implant (timing clearly stated) | The fat was strained manually of fluid | 134 | 1.4 (1–2) | ND |
| Patel AA et al. (2020) [23] | 126 immediate FG with Implant reconstruction, 31 delayed FG | Coleman | 94 | 1.3 (1–2) | ND |
| Gronovich Y et al. (2021) [11] | At time 0 associated to prepectoral implant placement with ADM | K Vac sysrtem | 59.8 | 1 (1) | ND |
| Authors | N of Breast | Previous Radio Therapy | Total Complications | Minor Complications | Major Complications | Capsular Contracture |
|---|---|---|---|---|---|---|
| Stillaert FBJL et al. (2020) [21] | 56 | Prior RT ND, Postop adjuvant RT 1 case | 4 (1 hematoma, 1 expander infection,2 implant infection) | 1 (1 hematoma) | 3 (1 TE infection, 2 implant infection) | 0/56 |
| Razzouk K et al. (2019) [15] | 32 | All patients underwent PMRT | 5(1 implant infection, 4 cystic fat necrosis.) | 4 (4cystic fat necrosis) | 1 (1 Implant infection) | nd |
| Sommeling CE et al. (2017) [14] | 23 | PMRT in 6 patients Neoadjuvant ND | 1 (1 severe infection with skin necrosis necessitated removal of the implant) | 0 | 1 (1 implant infection with fat necrosis) | nd |
| Razzouk K et al. (2020) [16] | 136 | All patients underwent RT prior to Fat Grafting (mean 19.6 months) | 11 (7 cystic seroma, 1 minor pnx, 1 infection (implant explantation), 2 skin necrosis(implant explantation) | 7 (cystic seromas) | 3 (1implant infection, 2 skin necrosis) | 15/136 |
| Sarfati I et al. (2011) [19] | 28 | All patients underwent RT prior to Fat Grafting (mean 9 months) | 4 (4 seromas, of whom 1 patient nedeed implant explantation) | 3 (minor seromas) | 1 (severe seroma needing implant removal) | 0/28 |
| Salgarello M et al. (2012) [17] | 16 | All patients underwent RT prior to Fat Grafting (>6 months) | No complication | 0 | 0 | 0/16 |
| Serra-Renom JM et al. (2010) [20] | 65 | All patients underwent RT prior to Fat Grafting (>1 year) | No complications | 0 | 0 | 0/65 |
| Cigna E. et al. (2012) [24] | 20 | No postoperative RT (previous irradiation ND) | 1 (1 fat necrosis) | 1 (1 fat necrosis) | 0 | nd |
| Cogliandro A et al. (2017) [22] | 46 | 34 PMRT | 2 (1 infection, 1 implant rupture) | 0 | 2 (1 infection, 1 implant rupture) | nd |
| Hammond DC (2015) [18] | 36 | RT ND (step 1 TE + ADM step2 FG + Implant) | 7 (3 capsular contracture, 1 oil cyst, 1 fat necrosis, 1 red breast, 1 dehiscence) | 3 (2 fat necrosis, 1 dehiscence) | 1 (1 red breast) | 3/36 |
| Patel AA et al. (2020) [23] | 270 | 29 previous RT, 32 PMRT | 20 (4 infection, 6 dehiscence, 4 seromas, 3 skin necrosis, 1 fat necrosis, 2 implant malposition) | 13 (6 dehiscence, 4 seromas, 1 fat necrosis, 2 implant malposition) | 7 (4 infection, 3 skin necrosis) | nd |
| Gronovich Y et al. (2021) [11] | 25 | No preop RT, 4 Postop RT | (5) infection 1, seroma 2, dehiscence1, flap necrosis 1 | 3 (2 seromas, 1 dehiscence) | 2 (1 infection, 1 flap necrosis) | nd |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alessandri Bonetti, M.; Carbonaro, R.; Borelli, F.; Amendola, F.; Cottone, G.; Mazzocconi, L.; Mastroiacovo, A.; Zingaretti, N.; Parodi, P.C.; Vaienti, L. Outcomes in Hybrid Breast Reconstruction: A Systematic Review. Medicina 2022, 58, 1232. https://doi.org/10.3390/medicina58091232
Alessandri Bonetti M, Carbonaro R, Borelli F, Amendola F, Cottone G, Mazzocconi L, Mastroiacovo A, Zingaretti N, Parodi PC, Vaienti L. Outcomes in Hybrid Breast Reconstruction: A Systematic Review. Medicina. 2022; 58(9):1232. https://doi.org/10.3390/medicina58091232
Chicago/Turabian StyleAlessandri Bonetti, Mario, Riccardo Carbonaro, Francesco Borelli, Francesco Amendola, Giuseppe Cottone, Luca Mazzocconi, Alessandro Mastroiacovo, Nicola Zingaretti, Pier Camillo Parodi, and Luca Vaienti. 2022. "Outcomes in Hybrid Breast Reconstruction: A Systematic Review" Medicina 58, no. 9: 1232. https://doi.org/10.3390/medicina58091232