

A Comparative Analysis of Dental Measurements in Physical and Digital Orthodontic Case Study Models
 , ,
, ,
Abstract
:1. Introduction
- –
- the linear measurement values are not influenced by the method, the material, or the obtainment technique used in the case study models;
- –
- the lack of space is undisturbed by the obtained values using various measurement techniques and dental study models.
2. Materials and Methods
2.1. Patient Selection and Impression Recording
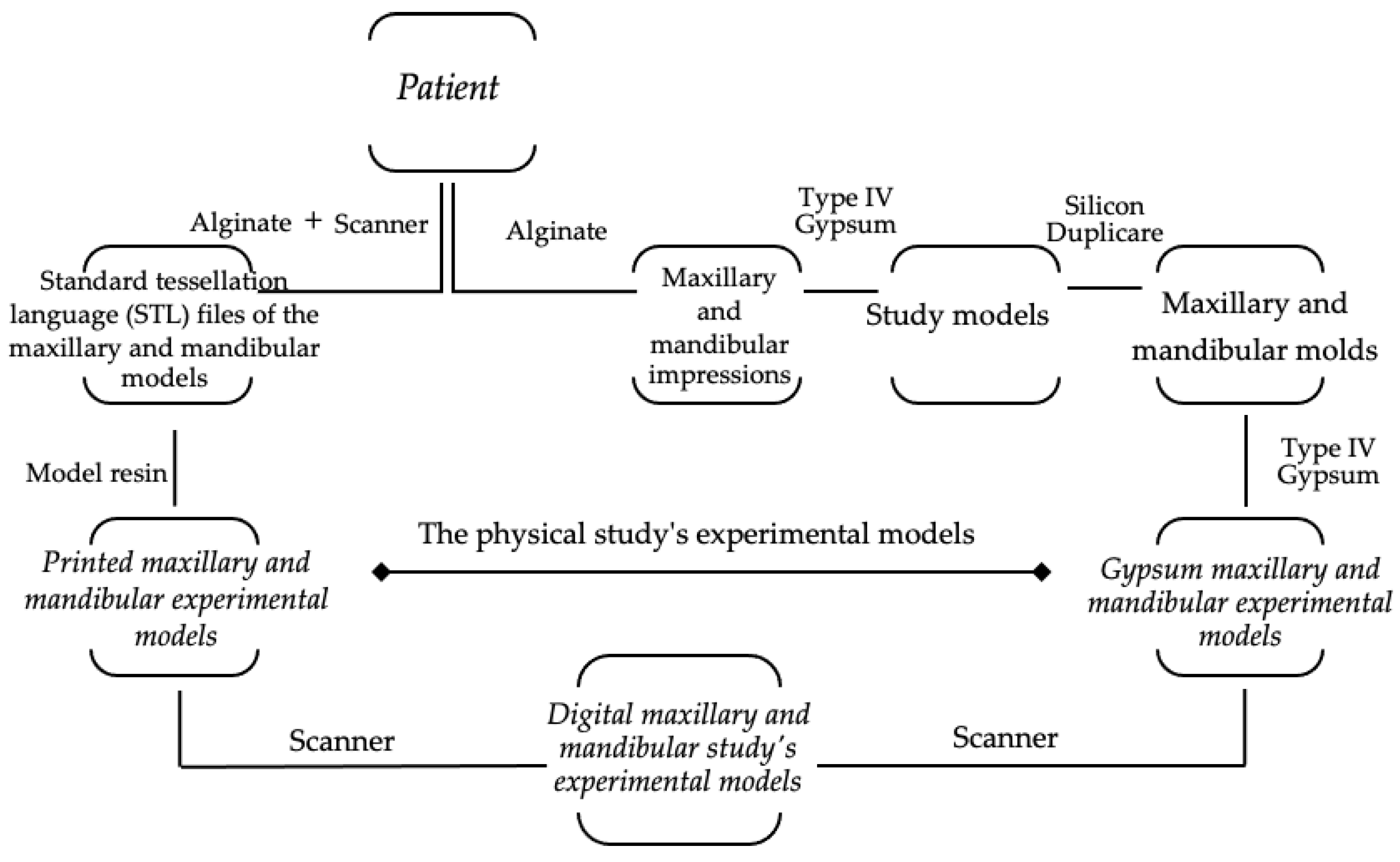
2.2. The Methods of Producing the Case Study Models
2.2.1. The Physical Models
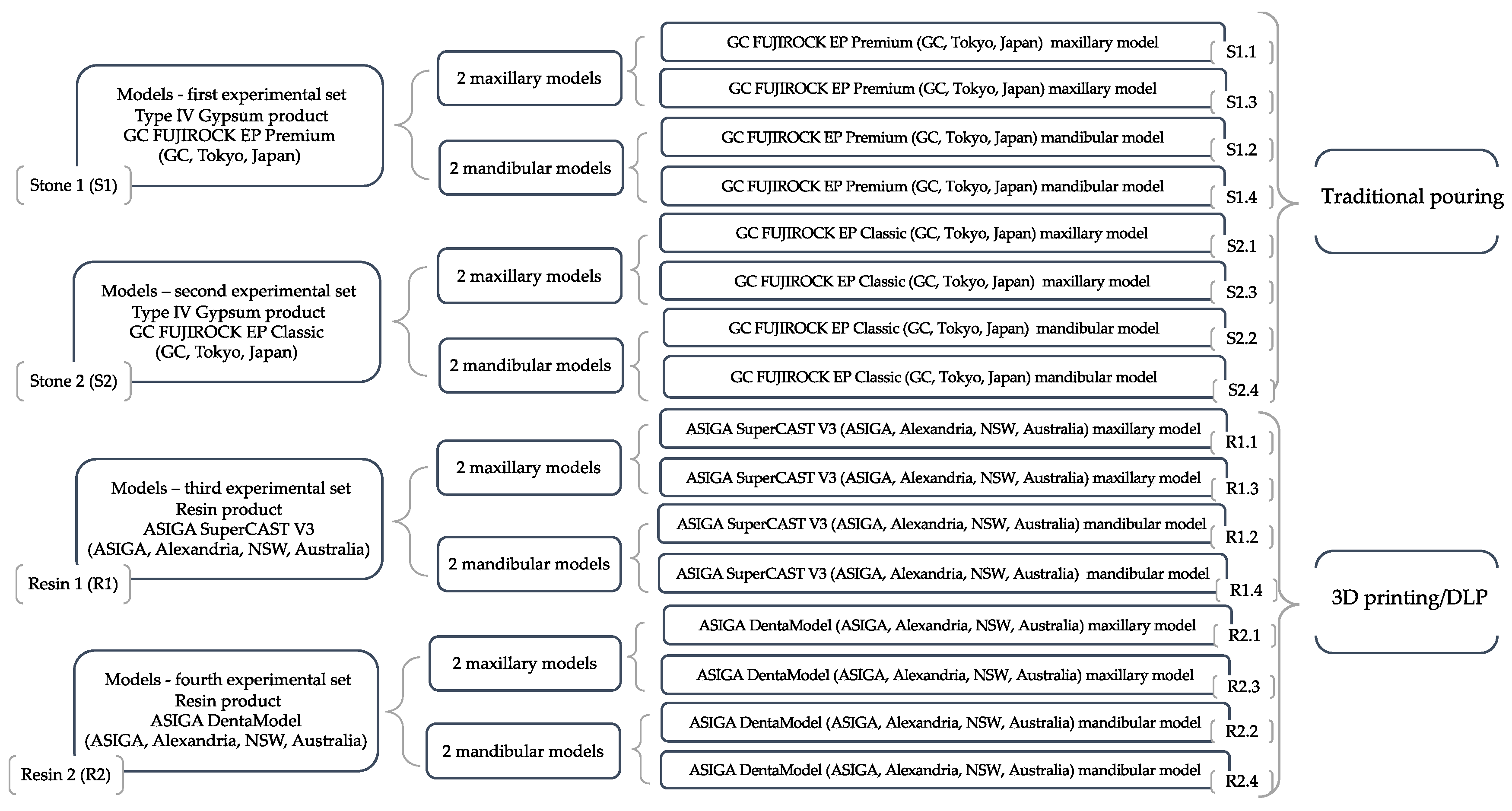
Dental Stone Models
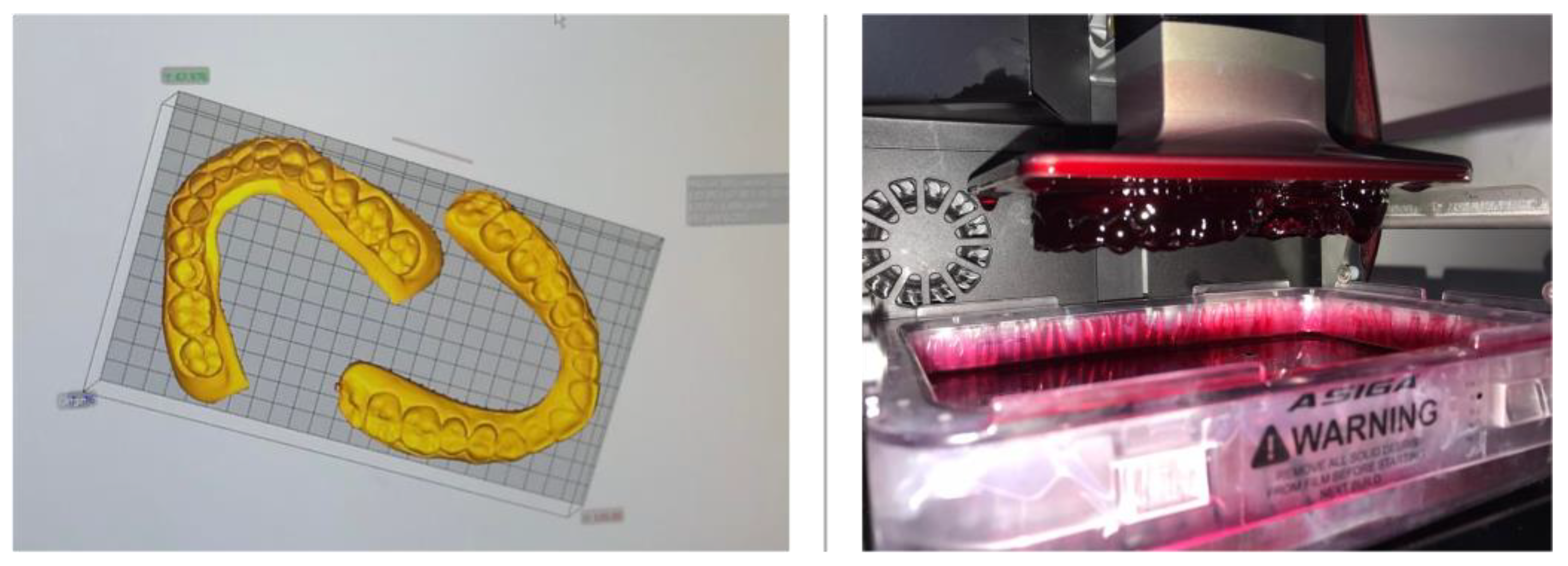
Three-Dimensionally Printed Models
- –
- Support scripts: contact with the model—0.5 mm; height leveling—2 mm; support spacing—2 mm; material strength—40×; and torsion tolerance—0.
- –
- Thickness layer—0.05 mm.
- –
- “Fast print” mode with separation detection and anti-aliasing.
2.2.2. The Digital Models
2.3. Dental Measurement
- –
- The upper arch interpremolar width was measured between central grooves on the occlusal surface of the first premolars.
- –
- The superior intermolar distance was measured between mesial pits on the occlusal surface of first molars.
- –
- The distance between the contact points of the lower premolars was assessed for the lower premolar diameter.
- –
2.3.1. Traditional Dental Measurement
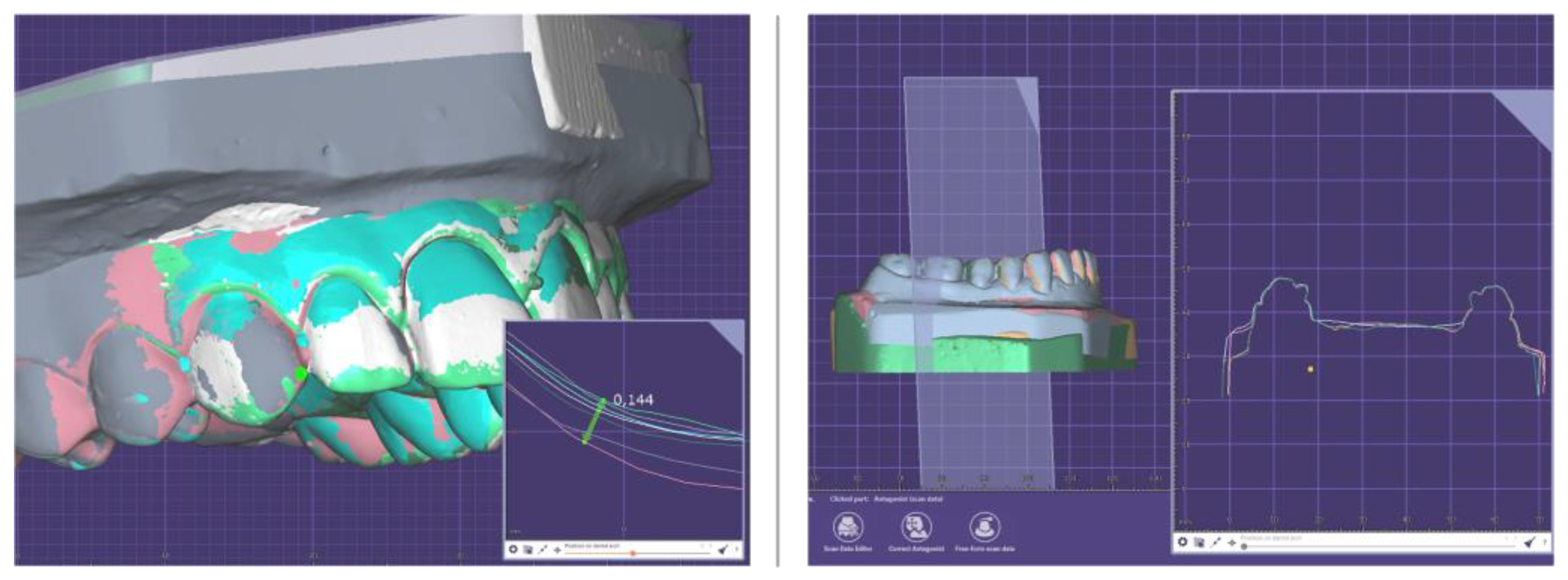
2.3.2. Modern Dental Measurement
2.4. Orthodontic Model Analysis
2.5. Statistical Analysis
3. Results
3.1. Evaluation of the First Hypothesis
- –
- The average values obtained by manual measurements of the mesiodistal widths of the incisors, canines, premolars, and first permanent molars, as well as the interpremolar and molar widths at the level of the traditionally models (type IV gypsum) versus 3D-printed models (resins).
- –
- The average values acquired by digital measurements of the mesiodistal widths of the incisors, canines, premolars, and first permanent molars, as well as the interpremolar and molar widths at the level of scanned models: type IV gypsum digital model versus resin (3D printing) digital model.
- –
- The average values produced by manual measures as opposed to digital measurements of the mesiodistal widths of the incisors, canines, premolars, and first permanent molars, as well as the interpremolar and molar widths at the level of the traditional models (type IV gypsum).
- –
- The average values obtained by manual measurements, as opposed to digital measurements, of the mesiodistal widths of the incisors, canines, premolars, and first permanent molars, as well as of the interpremolar and molar widths at the level of the additive processing models (resins).
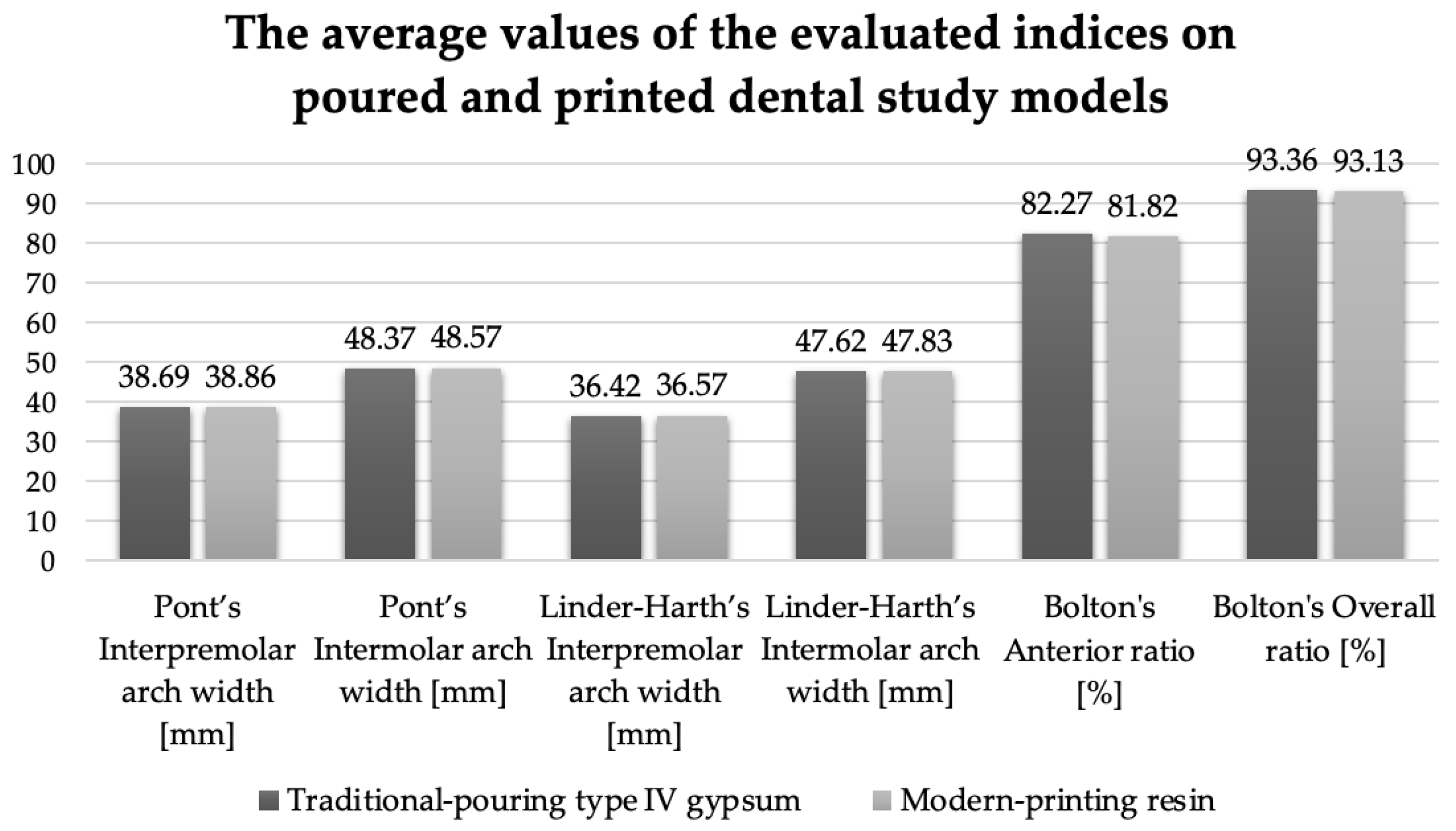
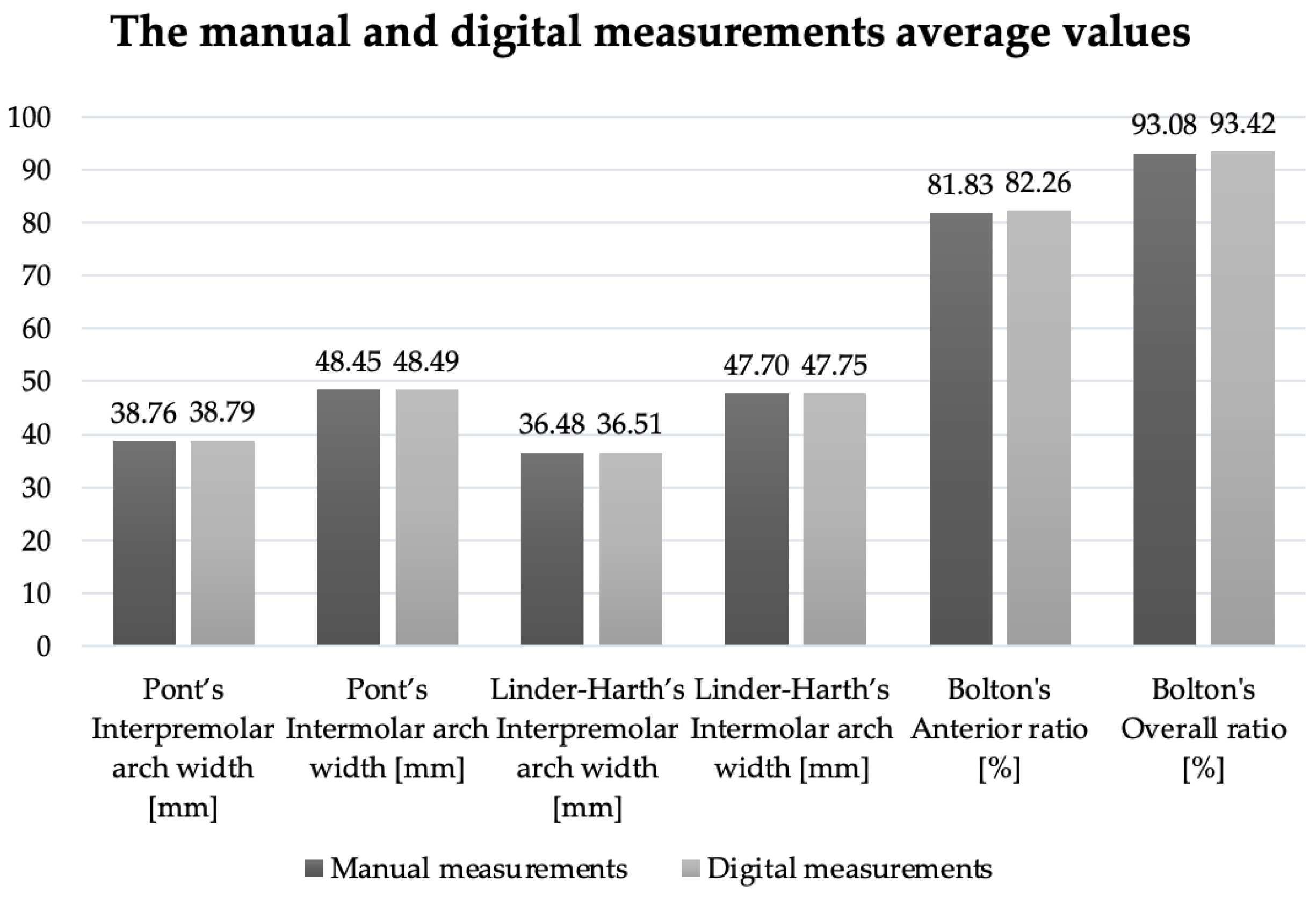
3.2. Evaluation of the Second Hypothesis
- –
- The values obtained by manual and digital measurements of the Pont index, the Linder–Harth index, and Bolton’s analysis on traditionally poured versus 3D-printed models.
- –
- The values obtained by manual versus digital measurements of the Pont index, the Linder–Harth index, and Bolton’s analysis on physical and digital models.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pachêco-Pereira, C.; De Luca Canto, G.; Major, P.W.; Flores-Mir, C. Variation of orthodontic treatment decision-making based on dental model type: A systematic review. Angle Orthod. 2015, 85, 501–509. [Google Scholar] [CrossRef]
- Marty, M.; Broutin, A.; Vergnes, J.N.; Vaysse, F. Comparison of student’s perceptions between 3D printed models versus series models in paediatric dentistry hands-on session. Eur. J. Dent. Educ. 2019, 23, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Pozzi, A.; Arcuri, L.; Lio, F.; Papa, A.; Nardi, A.; Londono, J. Accuracy of complete-arch digital implant impression with or without scanbody splinting: An in vitro study. J. Dent. 2022, 119, 104072. [Google Scholar] [CrossRef] [PubMed]
- De Francesco, M.; Stellini, E.; Granata, S.; Mazzoleni, S.; Ludovichetti, F.S.; Monaco, C.; Di Fiore, A. Assessment of Fit on Ten Screw-Retained Frameworks Realized through Digital Full-Arch Implant Impression. Appl. Sci. 2021, 11, 5617. [Google Scholar] [CrossRef]
- Amin, S.; Weber, H.P.; Finkelman, M.; El Rafie, K.; Kudara, Y.; Papaspyridakos, P. Digital vs. conventional full-arch implant impressions: A comparative study. Clin. Oral Implant. Res. 2017, 28, 1360–1367. [Google Scholar] [CrossRef]
- Abizadeh, N.; Moles, D.R.; O’Neill, J.; Noar, J.H. Digital versus plaster study models: How accurate and reproducible are they? J. Orthod. 2012, 39, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Akdeniz, B.S.; Aykaç, V.; Turgut, M.; Çetin, S. Digital dental models in orthodontics: A review. J. Exp. Clin. Med. 2022, 39, 250–255. [Google Scholar]
- Gül Amuk, N.; Karsli, E.; Kurt, G. Comparison of dental measurements between conventional plaster models, digital models obtained by impression scanning and plaster model scanning. Int. Orthod. 2019, 17, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Horton, H.M.; Miller, J.R.; Gaillard, P.R.; Larson, B.E. Technique comparison for efficient orthodontic tooth measurements using digital models. Angle Orthod. 2010, 80, 254–261. [Google Scholar] [CrossRef]
- Goriuc, A.; Jităreanu, A.; Mârțu, I.; Dascălu, C.G.; Kappenberg-Niţescu, D.C.; Solomon, S.M.; Mârțu, A.; Foia, L.; Țapu, I.; Istrate, B.; et al. Experimental EDX analysis of different periodontal splinting systems. Exp. Ther. Med. 2021, 22, 1384. [Google Scholar] [CrossRef]
- Baciu, E.R.; Cimpoeșu, R.; Vițalariu, A.; Baciu, C.; Cimpoeșu, N.; Sodor, A.; Zegan, G.; Murariu, A. Surface Analysis of 3D (SLM) Co–Cr–W Dental Metallic Materials. Appl. Sci. 2021, 11, 255. [Google Scholar] [CrossRef]
- Mârțu, I.; Murariu, A.; Baciu, E.R.; Savin, C.N.; Foia, I.; Tatarciuc, M.; Diaconu-Popa, D. An Interdisciplinary Study Regarding the Characteristics of Dental Resins Used for Temporary Bridges. Medicina 2022, 58, 811. [Google Scholar] [CrossRef] [PubMed]
- Tancu, A.M.; Pantea, M.; Totan, A.; Tanase, M.; Imre, A. 3D Printed Dental Models-A comparative analysis, Rev. Mater. Plast. 2019, 56, 51–54. [Google Scholar] [CrossRef]
- Alharbi, N.; Wismeijer, D.; Osman, R.B. Additive manufacturing techniques in prosthodontics: Where do we currently stand? a critical review. Int. J. Prosthodont. 2017, 30, 474–484. [Google Scholar] [CrossRef] [PubMed]
- Hussein, M.O.; Hussein, L.A. Optimization of Digital Light Processing Three-Dimensional Printing of the Removable Partial Denture Frameworks; The Role of Build Angle and Support Structure Diameter. Materials 2022, 15, 2316. [Google Scholar] [CrossRef] [PubMed]
- Unkovskiy, A.; Schmidt, F.; Beuer, F.; Li, P.; Spintzyk, S.; Kraemer Fernandez, P. Stereolithography vs. Direct Light Processing for Rapid Manufacturing of Complete Denture Bases: An In Vitro Accuracy Analysis. J. Clin. Med. 2021, 10, 1070. [Google Scholar] [CrossRef] [PubMed]
- Tzivelekis, C.; Sgardelis, P.; Waldron, K.; Whalley, R.; Huo, D.; Dalgarno, K. Fabrication routes via projection stereolithography for 3D-printing of microfluidic geometries for nucleic acid amplification. PLoS ONE 2020, 15, e0240237. [Google Scholar] [CrossRef]
- Shaikh, S.; Nahar, P.; Ali, H.M. Current perspectives of 3d printing in dental applications. Braz. Dent. Sci. 2021, 24, 1–9. [Google Scholar] [CrossRef]
- Iliescu, A.A.; Perlea, P.; Iliescu, M.G.; Gorea, V.; Nicolau, G. Printarea 3D în tehnologia dentara-statusul actual. Med. Stomatol. 2017, 45, 9–13. [Google Scholar]
- Ender, A.; Mehl, A. Accuracy of complete-arch dental impressions: A new method of measuring trueness and precision. J. Prosthet. Dent. 2013, 109, 121–128. [Google Scholar] [CrossRef]
- Pantea, M.; Ciocoiu, R.; Tancu, A.M.C.; Nină, D.M.; Petre, A.; Antoniac, I.V.; Melescanu-Imre, M. Comparative Study on Two Methods Used in Obtaining 3D Printed Dental Models. Mater. Plast. 2019, 56, 812. [Google Scholar] [CrossRef]
- Joda, T.; Matthisson, L.; Zitzmann, N.U. Impact of Aging on the Accuracy of 3D-Printed Dental Models: An In Vitro Investigation. J. Clin. Med. 2020, 9, 1436. [Google Scholar] [CrossRef]
- Fernandez, C.C.A.; Pereira, C.V.C.A.; Luiz, R.R.; Vieira, A.R.; De Castro Costa, M. Dental anomalies in different growth and skeletal malocclusion patterns. Angle Orthod. 2018, 88, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Devi, L.B.; Keisam, A.; Singh, H.P. Malocclusion and occlusal traits among dental and nursing students of Seven North-East states of India. J. Oral Biol. Craniofac. Res. 2022, 12, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Uslu, O.; Akcam, M.O.; Evirgen, S.; Cebeci, I. Prevalence of dental anomalies in various malocclusions. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 328–335. [Google Scholar] [CrossRef]
- Rykman, A.; Smailiene, D. Application of Pont’s Index to Lithuanian Individuals: A Pilot Study. J. Oral Maxillofac. Res. 2015, 6, e4. [Google Scholar] [CrossRef]
- Domenyuk, D.A.; Vedeshina, E.G.; Dmitrienko, S.V. Mistakes in Pont (Linder-Harth) method used for diagnosing abnormal dental arches in transversal plane. Arch. Euromed. 2016, 6, 23–26. [Google Scholar]
- Bolton, W. The clinical application of a tooth-size analysis. Am. J. Orthod. 1962, 48, 504–529. [Google Scholar] [CrossRef]
- Mollabashi, V.; Soltani, M.K.; Moslemian, N.; Akhlaghian, M.; Akbarzadeh, M.; Samavat, H.; Abolvardi, M. Comparison of Bolton ratio in normal occlusion and different malocclusion groups in Iranian population. Int. Orthod. 2019, 17, 143–150. [Google Scholar] [CrossRef]
- Wadhwa, S.S.; Mehta, R.; Duggal, N.; Vasudeva, K. The effect of pouring time on the dimensional accuracy of casts made from different irreversible hydrocolloid impression materials. Contemp. Clin. Dent. 2013, 3, 313–318. [Google Scholar] [CrossRef]
- Millstein, P.L. Determining the accuracy of gypsum casts made from type IV dental stone. J. Oral Rehabil. 1992, 19, 239–243. [Google Scholar] [CrossRef]
- Shastry, S.; Park, J.H. Evaluation of the use of digital study models in postgraduate orthodontic programs in the United States and Canada. Angle Orthod. 2014, 84, 62–67. [Google Scholar] [CrossRef]
- Palmer, N.G.; Yacyshyn, J.R.; Northcott, H.C.; Nebbe, B.; Major, P.W. Perceptions and attitudes of Canadian orthodontists regarding digital and electronic technology. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, T.; Motohashi, N.; Tominaga, R.; Iwata, K. Three-dimensional dental cast analyzing system using laser scanning. Am. J. Orthod. Dentofac. Orthop. 1996, 110, 365–369. [Google Scholar] [CrossRef]
- Fleming, P.S.; Marinho, V.; Johal, A. Orthodontic measurements on digital study models compared with plaster models: A systematic review. Orthod. Craniofac. Res. 2011, 14, 1–16. [Google Scholar] [CrossRef]
- Luu, N.S.; Nikolcheva, L.G.; Retrouvey, J.M.; Flores-Mir, C.; El-Bialy, T.; Carey, J.P.; Major, P.W. Linear measurements using virtual study models. Angle Orthod. 2012, 82, 1098–1106. [Google Scholar] [CrossRef]
- Sousa, M.V.; Vasconcelos, E.C.; Janson, G.; Garib, D.; Pinzan, A. Accuracy and reproducibility of 3-dimensional digital model measurements. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Sayed, M.E.; Al-Mansour, H.; Alshehri, A.H.; Al-Sanabani, F.; Al-Makramani, B.M.A.; Mugri, M.H.; Ahmed, W.M.; Alqahtani, N.M.; Bukhary, D.M.; Alsurayyie, F.H.; et al. Accuracy of Master Casts Generated Using Conventional and Digital Impression Modalities: Part 2—The Full Arch Dimension. Appl. Sci. 2022, 12, 2148. [Google Scholar] [CrossRef]
- Nestler, N.; Wesemann, C.; Spies, B.C.; Beuer, F.; Bumann, A. Dimensional accuracy of extrusion- and photopolymerization-based 3D printers: In vitro study comparing printed casts. J. Prosthet. Dent. 2021, 125, 103–110. [Google Scholar] [CrossRef]
- Choi, W.J.; Lee, S.J.; Moon, C.H. Evaluation of accuracy of 3-dimensional printed dental models in reproducing intermaxillary relational measurements: Based on inter-operator differences. Korean J. Orthod. 2022, 52, 20–28. [Google Scholar] [CrossRef]
- Jin, S.J.; Kim, D.Y.; Kim, J.H.; Kim, W.C. Accuracy of Dental Replica Models Using Photopolymer Materials in Additive Manufacturing: In Vitro Three-Dimensional Evaluation. J. Prosthodont. 2019, 28, e557–e562. [Google Scholar] [CrossRef] [PubMed]
- Etemad-Shahidi, Y.; Qallandar, O.B.; Evenden, J.; Alifui-Segbaya, F.; Ahmed, K.E. Accuracy of 3-Dimensionally Printed Full-Arch Dental Models: A Systematic Review. J. Clin. Med. 2020, 9, 3357. [Google Scholar] [CrossRef] [PubMed]
- Tomassetti, J.J.; Taloumis, L.J.; Denny, J.M.; Fischer, M.S., Jr. A comparison of 3 computerized Bolton tooth-size analyses with a commonly used method. Angle Orthod. 2001, 71, 351–357. [Google Scholar] [PubMed]
- Zilberman, O.; Huggare, J.A.; Parikakis, K.A. Evaluation of the validity of tooth size and arch width measurements using conventional and three-dimensional virtual orthodontic models. Angle Orthod. 2003, 73, 301–306. [Google Scholar]
- O’Mahony, G.; Millett, D.T.; Barry, M.K.; McIntyre, G.T.; Cronin, M.S. Tooth size discrepancies in Irish orthodontic patients among different malocclusion group. Angle Orthod. 2011, 81, 130–133. [Google Scholar] [CrossRef]
- Zerouaoui, M.F.; Bahije, L.; Zaoui, F.; Regragui, S. Study of variations of the Bolton index in the Moroccan population depending on Angle malocclusion class. Int. Orthod. 2014, 12, 213–221. [Google Scholar] [CrossRef]
- Stevens, D.R.; Flores-Mir, C.; Nebbe, B.; Raboud, D.W.; Heo, G.; Major, P.W. Validity, reliability, and reproducibility of plaster vs. digital study models: Comparison of peer assessment rating and Bolton analysis and their constituent measurements. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 794–803. [Google Scholar] [CrossRef]
- Naidu, D.; Freer, T.J. Validity, reliability, and reproducibility of the iOC intraoral scanner: A comparison of tooth widths and Bolton ratios. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 304–410. [Google Scholar] [CrossRef]
- Bowes, M.; Dear, W.; Close, E.; Freer, T.J. Tooth width measurement using the Lythos digital scanner. Aust. Orthod. J. 2017, 33, 73–81. [Google Scholar] [CrossRef]
- Wan Hassan, W.N.; Yusoff, Y.; Mardi, N.A. Comparison of reconstructed rapid prototyping models produced by 3-dimensional printing and conventional stone models with different degrees of crowding. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 209–218. [Google Scholar] [CrossRef]
- Hirogaki, Y.; Sohmura, T.; Satoh, H.; Takahashi, J.; Takada, K. Complete 3-D reconstruction of dental cast shape using perceptual grouping. IEEE Trans. Med. Imaging 2001, 20, 1093–1101. [Google Scholar] [CrossRef]
- Bell, A.; Ayoub, A.F.; Siebert, P. Assessment of the accuracy of a three-dimensional imaging system for archiving dental study models. J. Orthod. 2003, 30, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; Chen, Y.-W.; AlShawaf, B.; Kang, K.; Finkelman, M.; Chronopoulos, V.; Weber, H.-P. Digital workflow: In vitro accuracy of 3D printed casts generated from complete-arch digital implant scans. J. Prosthet. Dent. 2020, 124, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Leifert, M.F.; Leifert, M.M.; Efstratiadis, S.S.; Cangialosi, T.J. Comparison of space analysis evaluations with digital models and plaster dental casts. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 16.e1–16.e4. [Google Scholar] [CrossRef]
- Cuperus, A.M.; Harms, M.C.; Rangel, F.A.; Bronkhorst, E.M.; Schols, J.G.; Breuning, K.H. Dental models made with an intraoral scanner: A validation study. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 308–313. [Google Scholar] [CrossRef]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C.L. Diagnostic accuracy and measurement sensitivity of digital models for orthodontic purposes: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 161–170. [Google Scholar] [CrossRef]
- Alrasheed, W.A.; Owayda, A.M.; Hajeer, M.Y.; Khattab, T.Z.; Almahdi, W.H. Validity and Reliability of Intraoral and Plaster Models’ Photographs in the Assessment of Little’s Irregularity Index, Tooth Size-Arch Length Discrepancy, and Bolton’s Analysis. Cureus 2022, 14, e23067. [Google Scholar] [CrossRef]
- Morton, J.; Derakhshan, M.; Kaza, S.; Li, C. Design of the Invisalign system performance. Semin. Orthod. 2017, 23, 3–11. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Methods | Equations |
|---|---|
| Pont index | Sum of incisors (SI) = sum of mesio-distal width of the maxillary incisors |
| Interpremolar arch widths | |
| Intermolar arch widths | |
| Linder–Harth index | Interpremolar arch widths |
| Intermolar arch widths | |
| Bolton’s analysis | Anterior ratio |
| Overall ratio |
| Pairwise Comparison | Mean Rank | p-Value a | |
|---|---|---|---|
| Type IV gypsum versus resin DigitalCalliper | S1.1 + S1.3 + S2.1 + S2.3 DigitalCalliper | 28.45 | 0.980 |
| R1.1 + R1.3 + R2.1 + R2.3 DigitalCalliper | 28.55 | ||
| Type IV gypsum versus resin Exocad | S1.1 + S1.3 + S2.1 + S2.3 Exocad | 28.75 | 0.909 |
| R1.1 + R1.3 + R2.1 + R2.3 Exocad | 28.25 | ||
| DigitalCalliper versus Exocad Type IV gypsum products | S1.1 + S1.3 + S2.1 + S2.3 DigitalCalliper | 28.50 | 1.000 |
| S1.1 + S1.3 + S2.1 + S2.3 Exocad | 28.50 | ||
| DigitalCalliper versus exocad Resins | R1.1 + R1.3 + R2.1 + R2.3 DigitalCalliper | 28.70 | 0.928 |
| R1.1 + R1.3 + R2.1 + R2.3 Exocad | 28.30 | ||
| Pairwise Comparison | Mean Rank | p-Value a | |
|---|---|---|---|
| Type IV gypsum versus resin DigitalCalliper | S1.2 + S1.4 + S2.2 + S2.4 DigitalCalliper | 28.71 | 0.922 |
| R1.2 + R1.4 + R2.2 + R2.4 DigitalCalliper | 28.29 | ||
| Type IV gypsum versus resin Exocad | S1.2 + S1.4 + S2.2 + S2.4 Exocad | 29.09 | 0.787 |
| R1.2 + R1.4 + R2.2 + R2.4 Exocad | 27.91 | ||
| DigitalCalliper versus Exocad Type IV gypsum products | S1.2 + S1.4 + S2.2 + S2.4 DigitalCalliper | 27.95 | 0.799 |
| S1.2 + S1.4 + S2.2 + S2.4 Exocad | 29.05 | ||
| DigitalCalliper versus Exocad Resins | R1.2 + R1.4 + R2.2 + R2.4 DigitalCalliper | 28.23 | 0.902 |
| R1.2 + R1.4 + R2.2 + R2.4 Exocad | 28.77 | ||
| Orthodontic Analysis | Traditional Pouring Versus 3D Printing | Mean Rank | p-Value a | |
|---|---|---|---|---|
| Pont index | Interpremolar arch widths | Traditional pouring | 2.50 | 0.020 * |
| 3D printing | 6.50 | |||
| Intermolar arch widths | Traditional pouring | 2.50 | 0.020 * | |
| 3D printing | 6.50 | |||
| The difference between the calculated and the measured interpremolar arch widths values | Traditional pouring | 6.00 | 0.083 | |
| 3D printing | 3.00 | |||
| The difference between the calculated and the measured intermolar arch widths values | Traditional pouring | 6.00 | 0.059 | |
| 3D printing | 3.00 | |||
| Linder–Harth index | Interpremolar arch widths | Traditional pouring | 2.50 | 0.021 * |
| 3D printing | 6.50 | |||
| Intermolar arch widths | Traditional pouring | 2.50 | 0.020 * | |
| 3D printing | 6.50 | |||
| The difference between the calculated and the measured interpremolar arch widths values | Traditional pouring | 6.00 | 0.083 | |
| 3D printing | 3.00 | |||
| The difference between the calculated and the measured intermolar arch widths values | Traditional pouring | 6.13 | 0.059 | |
| 3D printing | 2.88 | |||
| Bolton’s analysis | Anterior ratio | Traditional pouring | 5.75 | 0.149 |
| 3D printing | 3.25 | |||
| Overall ratio | Traditional pouring | 5.63 | 0.189 | |
| 3D printing | 3.38 | |||
| Orthodontic Analysis | Manual Versus Digital Measurements | Mean Rank | p-Value a | |
|---|---|---|---|---|
| Pont index | Interpremolar arch widths | Manual measurements | 4.50 | 1.000 |
| Digital measurements | 4.50 | |||
| Intermolar arch widths | Manual measurements | 4.50 | 1.000 | |
| Digital measurements | 4.50 | |||
| The difference between the calculated and the measured interpremolar arch widths values | Manual measurements | 5.75 | 0.149 | |
| Digital measurements | 3.25 | |||
| The difference between the calculated and the measured intermolar arch widths values | Manual measurements | 4.63 | 0.885 | |
| Digital measurements | 4.38 | |||
| Linder–Harth index | Interpremolar arch widths | Manual measurements | 4.50 | 0.885 |
| Digital measurements | 4.50 | |||
| Intermolar arch widths | Manual measurements | 4.50 | 1.000 | |
| Digital measurements | 4.50 | |||
| The difference between the calculated and the measured interpremolar arch widths values | Manual measurements | 5.75 | 0.149 | |
| Digital measurements | 3.25 | |||
| The difference between the calculated and the measured intermolar arch widths values | Manual measurements | 4.63 | 0.885 | |
| Digital measurements | 4.38 | |||
| Bolton’s analysis | Anterior ratio | Manual measurements | 3.00 | 0.083 |
| Digital measurements | 6.00 | |||
| Overall ratio | Manual measurements | 2.63 | 0.028 * | |
| Digital measurements | 6.38 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baciu, E.-R.; Budală, D.G.; Vasluianu, R.-I.; Lupu, C.I.; Murariu, A.; Gelețu, G.L.; Zetu, I.N.; Diaconu-Popa, D.; Tatarciuc, M.; Nichitean, G.; et al. A Comparative Analysis of Dental Measurements in Physical and Digital Orthodontic Case Study Models. Medicina 2022, 58, 1230. https://doi.org/10.3390/medicina58091230
Baciu E-R, Budală DG, Vasluianu R-I, Lupu CI, Murariu A, Gelețu GL, Zetu IN, Diaconu-Popa D, Tatarciuc M, Nichitean G, et al. A Comparative Analysis of Dental Measurements in Physical and Digital Orthodontic Case Study Models. Medicina. 2022; 58(9):1230. https://doi.org/10.3390/medicina58091230
Chicago/Turabian StyleBaciu, Elena-Raluca, Dana Gabriela Budală, Roxana-Ionela Vasluianu, Costin Iulian Lupu, Alice Murariu, Gabriela Luminița Gelețu, Irina Nicoleta Zetu, Diana Diaconu-Popa, Monica Tatarciuc, Giorgio Nichitean, and et al. 2022. "A Comparative Analysis of Dental Measurements in Physical and Digital Orthodontic Case Study Models" Medicina 58, no. 9: 1230. https://doi.org/10.3390/medicina58091230