
Incidence of Hip Fractures among Patients with Chronic Otitis Media: The Real-World Data


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
- ✓
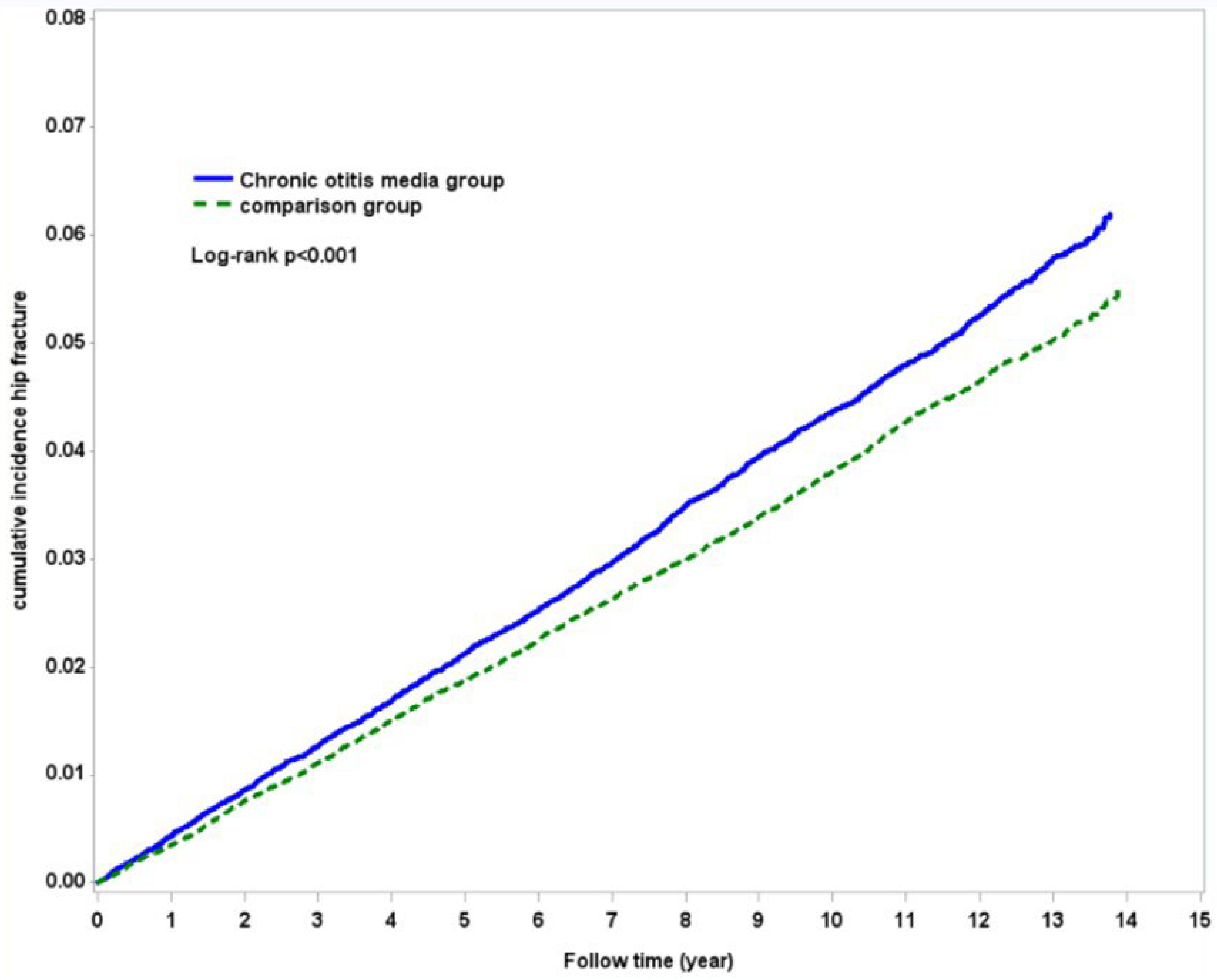
- The incidence of hip fracture was 4.48 and 3.92 per 1000 person-years for comparison and COM cohorts respectively. After adjustment for gender, age, and comorbidities, the COM patients had a 1.11-fold (aHR = 1.11; 95% CI = 1.05–1.17) risk of hip fracture than the control subjects.
- ✓
- The cumulative incidence of hip fracture is higher in the COM cohort (p < 0.001) than in the comparison cohort.
- ✓
- Among the COM patients, a history of hearing loss is associated with higher (aHR = 1.21; 95% CI = 1.20–1.42) fracture risk.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Park, M.; Lee, J.S.; Lee, J.H.; Oh, S.H.; Park, M.K. Prevalence and risk factors of chronic otitis media: The Korean National Health and Nutrition Examination Survey 2010–2012. PLoS ONE 2015, 10, e0125905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nadol, J.B., Jr. Revision mastoidectomy. Otolaryngol. Clin. N. Am. 2006, 39, 723–740. [Google Scholar] [CrossRef] [PubMed]
- Straub, R.H.; Cutolo, M.; Pacifici, R. Evolutionary medicine and bone loss in chronic inflammatory diseases—A theory of inflammation-related osteopenia. Semin. Arthritis Rheum. 2015, 45, 220–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segade, F.; Daly, K.A.; Allred, D.; Hicks, P.J.; Cox, M.; Brown, M.; Hardisty-Hughes, R.E.; Brown, S.D.; Rich, S.S.; Bowden, D.W. Association of the FBXO11 gene with chronic otitis media with effusion and recurrent otitis media: The Minnesota COME/ROM Family Study. Arch. Otolaryngol. Head Neck Surg. 2006, 132, 729–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rye, M.S.; Wiertsema, S.P.; Scaman, E.S.; Oommen, J.; Sun, W.; Francis, R.W.; Ang, W.; Pennell, C.E.; Burgner, D.; Richmond, P.; et al. FBXO11, a regulator of the TGFbeta pathway, is associated with severe otitis media in Western Australian children. Genes Immun. 2011, 12, 352–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Kua, H.Y.; Hu, Y.; Guo, K.; Zeng, Q.; Wu, Q.; Ng, H.H.; Karsenty, G.; de Crombrugghe, B.; Yeh, J.; et al. p53 functions as a negative regulator of osteoblastogenesis, osteoblast-dependent osteoclastogenesis, and bone remodeling. J. Cell Biol. 2006, 172, 115–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metcalfe, D. The pathophysiology of osteoporotic hip fracture. McGill J. Med. 2008, 11, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Carpintero, P.; Caeiro, J.R.; Carpintero, R.; Morales, A.; Silva, S.; Mesa, M. Complications of hip fractures: A review. World J. Orthop. 2014, 5, 402–411. [Google Scholar] [CrossRef] [PubMed]
- Lai, S.W.; Liao, K.F.; Lin, C.L.; Lin, C.C.; Lin, C.H. Longitudinal data of multimorbidity and polypharmacy in older adults in Taiwan from 2000 to 2013. Biomedicine 2020, 10, 1–4. [Google Scholar] [CrossRef]
- Lai, S.W.; Liao, K.F.; Lin, C.L.; Lin, C.H. Association between Parkinson’s disease and proton pump inhibitors therapy in older people. Biomedicine 2020, 10, 1–4. [Google Scholar] [CrossRef]
- Chiang, C.H.; Li, C.Y.; Hu, K.C.; Fu, Y.H.; Chiu, C.C.; Hsia, C.C.; Kuo, S.J.; Hung, C.H. The Association between Iron-Deficiency Anemia (IDA) and Septic Arthritis (SA): The Real-World Data. Medicina 2022, 58, 617. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.C.; Lin, C.C.; Lin, C.D.; Chung, H.K.; Wang, C.Y.; Tsai, M.H.; Kao, C.H. Increased Acquired Cholesteatoma Risk in Patients with Osteoporosis: A Retrospective Cohort Study. PLoS ONE 2015, 10, e0132447. [Google Scholar] [CrossRef] [PubMed]
- Amar, M.S.; Wishahi, H.F.; Zakhary, M.M. Clinical and biochemical studies of bone destruction in cholesteatoma. J. Laryngol. Otol. 1996, 110, 534–539. [Google Scholar] [CrossRef] [PubMed]
- Kuczkowski, J.; Sakowicz-Burkiewicz, M.; Izycka-Swieszewska, E. Expression of the receptor activator for nuclear factor-kappaB ligand and osteoprotegerin in chronic otitis media. Am. J. Otolaryngol. 2010, 31, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.Y.; Chole, R.A. Bone resorption in chronic otitis media: The role of the osteoclast. ORL J. Otorhinolaryngol. Relat. Spec. 2002, 64, 95–107. [Google Scholar] [CrossRef]
- Rye, M.S.; Blackwell, J.M.; Jamieson, S.E. Genetic susceptibility to otitis media in childhood. Laryngoscope 2012, 122, 665–675. [Google Scholar] [CrossRef]
- Bhutta, M.F.; Lambie, J.; Hobson, L.; Goel, A.; Hafren, L.; Einarsdottir, E.; Mattila, P.S.; Farrall, M.; Brown, S.; Burton, M.J. A mouse-to-man candidate gene study identifies association of chronic otitis media with the loci TGIF1 and FBXO11. Sci. Rep. 2017, 7, 12496. [Google Scholar] [CrossRef] [Green Version]
- Fennen, M.; Pap, T.; Dankbar, B. Smad-dependent mechanisms of inflammatory bone destruction. Arthritis Res. Ther. 2016, 18, 279. [Google Scholar] [CrossRef] [Green Version]
- Tateossian, H.; Hardisty-Hughes, R.E.; Morse, S.; Romero, M.R.; Hilton, H.; Dean, C.; Brown, S.D. Regulation of TGF-beta signalling by Fbxo11, the gene mutated in the Jeff otitis media mouse mutant. Pathogenetics 2009, 2, 5. [Google Scholar] [CrossRef] [Green Version]
- Abida, W.M.; Nikolaev, A.; Zhao, W.; Zhang, W.; Gu, W. FBXO11 promotes the Neddylation of p53 and inhibits its transcriptional activity. J. Biol. Chem. 2007, 282, 1797–1804. [Google Scholar] [CrossRef] [Green Version]
- Tateossian, H.; Morse, S.; Parker, A.; Mburu, P.; Warr, N.; Acevedo-Arozena, A.; Cheeseman, M.; Wells, S.; Brown, S.D. Otitis media in the Tgif knockout mouse implicates TGFbeta signalling in chronic middle ear inflammatory disease. Hum. Mol. Genet. 2013, 22, 2553–2565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlick, C.; Schniepp, R.; Loidl, V.; Wuehr, M.; Hesselbarth, K.; Jahn, K. Falls and fear of falling in vertigo and balance disorders: A controlled cross-sectional study. J. Vestib. Res. 2016, 25, 241–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, J.I.; Park, K.S.; Seo, S.H.; Park, H.W. Osteoporosis and hearing loss: Findings from the Korea National Health and Nutrition Examination Survey 2009–2011. Braz. J. Otorhinolaryngol. 2020, 86, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Kahveci, O.K.; Demirdal, U.S.; Yucedag, F.; Cerci, U. Patients with osteoporosis have higher incidence of sensorineural hearing loss. Clin. Otolaryngol. 2014, 39, 145–149. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| COM Cohort | Comparison Cohort | ||||
|---|---|---|---|---|---|
| n = 53,977 | n = 107,865 | p-Value * | |||
| n | % | n | % | ||
| Gender | 0.820 | ||||
| Female | 27,443 | 50.8 | 54,885 | 50.9 | |
| Male | 26,554 | 49.2 | 52,980 | 49.1 | |
| Age | 0.999 | ||||
| <20 | 26,132 | 48.4 | 52,135 | 48.3 | |
| 20–44 | 12,896 | 23.8 | 25,792 | 23.9 | |
| 45–64 | 10,154 | 18.8 | 20,308 | 18.8 | |
| ≥65 | 4815 | 8.92 | 9630 | 8.93 | |
| mean(SD) † | 27.84 (86.0) | 28.11 (84.4) | <0.001 | ||
| Comorbidities | |||||
| Hypertension | 11,988 | 22.2 | 21,349 | 19.7 | <0.001 |
| Diabetes | 7024 | 13.0 | 12,033 | 11.1 | <0.001 |
| Epilepsy | 453 | 0.84 | 638 | 0.59 | <0.001 |
| Ischemic heart disease | 3854 | 7.14 | 6120 | 5.67 | <0.001 |
| COPD | 10,639 | 20.3 | 14,314 | 13.2 | <0.001 |
| Stroke | 2392 | 4.43 | 3899 | 3.61 | <0.001 |
| Liver cirrhosis | 5576 | 10.3 | 8724 | 8.09 | <0.001 |
| Osteoporosis | 1712 | 3.17 | 3422 | 3.17 | 0.983 |
| End-stage renal disease | 0 | 0 | 0 | 0 | - |
| Variable | Hip Fracture | Crude HR (95%CI) | # Adjusted HR (95%CI) | ||
|---|---|---|---|---|---|
| Hip Fracture | PY | IR | |||
| Chronic otitis media | |||||
| No | 3997 | 1,018,072 | 3.92 | 1 (reference) | 1 (reference) |
| Yes | 2298 | 512,483 | 4.48 | 1.14 (1.08–1.20) *** | 1.11 (1.05–1.17) *** |
| Gender | |||||
| Female | 3175 | 777,192 | 4.08 | 1 (reference) | 1 (reference) |
| Male | 3120 | 753,363 | 4.14 | 1.01 (0.96–1.06) | 1.07 (1.02–1.13) ** |
| Age | |||||
| <20 | 2148 | 858,051 | 2.50 | 1 (reference) | 1 (reference) |
| 20–44 | 1113 | 332,276 | 3.34 | 1.37 (1.27–1.47) *** | 1.32 (1.23–1.43) *** |
| 45–64 | 1653 | 245,380 | 6.73 | 2.78 (2.61–2.96) *** | 2.21 (2.04–2.39) *** |
| ≥65 | 1381 | 94,848 | 14.5 | 6.14 (5.74–6.58) *** | 4.10 (3.72–4.52) *** |
| Comorbidities | |||||
| Hypertension | |||||
| No | 3826 | 1,259,598 | 3.03 | 1 (reference) | 1 (reference) |
| Yes | 2469 | 270,957 | 9.11 | 3.08 (2.88–3.19) *** | 1.21 (1.12–1.30) *** |
| Diabetes | |||||
| No | 4793 | 1,376,069 | 3.48 | 1 (reference) | 1 (reference) |
| Yes | 1502 | 154,486 | 9.72 | 2.82 (2.66–2.98) *** | 1.22 (1.14–1.31) *** |
| Epilepsy | |||||
| No | 6240 | 1,522,127 | 4.09 | 1 (reference) | 1 (reference) |
| Yes | 55 | 8428 | 6.52 | 1.60 (1.23–2.09) *** | 1.44 (1.10–1.88) ** |
| Ischemic heart disease | |||||
| No | 5538 | 1,463,746 | 3.78 | 1 (reference) | 1 (reference) |
| Yes | 757 | 66,809 | 11.3 | 3.06 (2.84–3.31) *** | 0.98 (0.89–1.07) |
| COPD | |||||
| No | 4994 | 1,317,988 | 3.78 | 1 (reference) | 1 (reference) |
| Yes | 1301 | 212,567 | 6.12 | 1.62 (1.53–1.73) *** | 1.19 (1.11–1.27) *** |
| Stroke | |||||
| No | 5767 | 1,491,279 | 3.86 | 1 (reference) | 1 (reference) |
| Yes | 528 | 39,276 | 13.4 | 3.56 (3.25–3.89) *** | 1.24 (1.12–1.37) *** |
| Liver cirrhosis | |||||
| No | 5502 | 1,428,513 | 3.85 | 1 (reference) | 1 (reference) |
| Yes | 793 | 102,042 | 7.77 | 2.05 (1.90–2.21) *** | 1.00 (0.92–1.09) |
| Osteoporosis | |||||
| No | 5808 | 1,495,082 | 3.88 | 1 (reference) | 1 (reference) |
| Yes | 487 | 35,473 | 13.7 | 3.60 (3.28–3.95) *** | 1.49 (1.34–1.65) *** |
| End-stage renal disease | |||||
| No | 6295 | 1,530,555 | 4.11 | 1 (reference) | 1 (reference) |
| Yes | -- | -- | -- | -- | -- |
| Variable | Chronic Otitis Media | Crude HR (95%CI) | # Adjusted HR (95%CI) | |||||
|---|---|---|---|---|---|---|---|---|
| No | Yes | |||||||
| Hip Fracture | PY | IR | Hip Fracture | PY | IR | |||
| Gender | ||||||||
| Female | 1980 | 517,377 | 3.82 | 1195 | 259,815 | 4.59 | 1.20 (1.11–1.29) *** | 1.17 (1.09–1.26) *** |
| Male | 2017 | 500,695 | 4.02 | 1103 | 252,668 | 4.36 | 1.08 (1.00–1.16) * | 1.05 (0.97–1.13) |
| Age | ||||||||
| <20 | 1389 | 570,608 | 2.43 | 759 | 287,443 | 2.64 | 1.08 (0.99–1.18) | 1.07 (0.98–1.17) |
| 20–44 | 675 | 220,884 | 3.05 | 438 | 111,392 | 3.93 | 1.28 (1.14–1.45) *** | 1.23 (1.09–1.39) *** |
| 45–64 | 1045 | 163,603 | 6.38 | 608 | 81,777 | 7.43 | 1.16 (1.05–1.28) ** | 1.12 (1.01–1.24) * |
| ≥65 | 888 | 62,977 | 14.10 | 493 | 31,871 | 15.46 | 1.09 (0.98–1.22) | 1.06 (0.95–1.19) |
| Comorbidity | ||||||||
| Hypertension | ||||||||
| No | 2492 | 844,254 | 2.95 | 1334 | 415,344 | 3.21 | 1.08 (1.01–1.16) * | 1.08 (1.01–1.16) * |
| Yes | 1505 | 173,818 | 8.65 | 964 | 97,139 | 9.92 | 1.14 (1.05–1.24) *** | 1.14 (1.05–1.24) ** |
| Diabetes | ||||||||
| No | 3106 | 920,361 | 3.37 | 1687 | 455,708 | 3.70 | 1.09 (1.03–1.16) ** | 1.08 (1.02–1.15) ** |
| Yes | 891 | 97,711 | 9.11 | 611 | 56,775 | 10.7 | 1.18 (1.06–1.30) ** | 1.19 (1.07–1.32) *** |
| Epilepsy | ||||||||
| No | 3964 | 1,013,163 | 3.91 | 2276 | 508,964 | 4.47 | 1.14 (1.08–1.20) *** | 1.11 (1.05–1.17) *** |
| Yes | 33 | 4909 | 6.72 | 22 | 3519 | 6.25 | 0.93 (0.54–1.60) | 1.02 (0.59–1.77) |
| IHD | ||||||||
| No | 3559 | 977,529 | 3.64 | 1979 | 486,216 | 4.07 | 1.11 (1.05–1.18) *** | 1.10 (1.04–1.16) *** |
| Yes | 438 | 40,543 | 10.8 | 319 | 26,267 | 12.1 | 1.12 (0.97–1.29) | 1.15 (1.00–1.33) * |
| COPD | ||||||||
| No | 3287 | 900,652 | 3.64 | 1707 | 417,335 | 4.09 | 1.12 (1.05–1.18) *** | 1.10 (1.04–1.17) *** |
| Yes | 710 | 117,420 | 6.04 | 591 | 95,148 | 6.21 | 1.02 (0.92–1.14) | 1.14 (1.02–1.27) * |
| Stroke | ||||||||
| No | 3675 | 994,043 | 3.69 | 2092 | 497,236 | 4.20 | 1.13 (1.07–1.20) *** | 1.11 (1.05–1.17) *** |
| Yes | 322 | 24,029 | 13.4 | 206 | 15,247 | 13.5 | 1.00 (0.84–1.20) | 1.04 (0.87–1.24) |
| Liver cirrhosis | ||||||||
| No | 3531 | 956,226 | 3.69 | 1971 | 472,287 | 4.17 | 1.12 (1.06–1.19) *** | 1.11 (1.05–1.18) *** |
| Yes | 466 | 61,846 | 7.53 | 327 | 40,196 | 8.13 | 1.08 (0.93–1.24) | 1.08 (0.93–1.24) |
| Osteoporosis | ||||||||
| No | 3688 | 994,420 | 3.70 | 2120 | 500,661 | 4.23 | 1.14 (1.08–1.20) *** | 1.10 (1.05–1.16) *** |
| Yes | 309 | 23,652 | 13.0 | 178 | 11,822 | 15.05 | 1.15 (0.95–1.38) | 1.14 (0.94–1.37) |
| ESRD | ||||||||
| No | 3997 | 1,018,072 | 3.92 | 2298 | 512,483 | 4.48 | 1.14 (1.08–1.20) *** | 1.11 (1.05–1.17) *** |
| Yes | 0 | 0 | 0 | 0 | 0 | 0 | -- | -- |
| Hip Fracture | PY | IR | Crude HR | # Adjusted HR | |
|---|---|---|---|---|---|
| n = 2298 | (95%CI) | (95%CI) | |||
| Gender | |||||
| Female | 1195 | 259,815 | 4.59 | 1 (reference) | 1 (reference) |
| Male | 1103 | 252,668 | 4.36 | 0.94 (0.87–1.03) | 1.19 (1.05–1.34) ** |
| Age | |||||
| <20 | 759 | 287,443 | 2.64 | 1 (reference) | 1 (reference) |
| 20–44 | 438 | 111,392 | 3.93 | 1.53 (1.36–1.72) *** | 1.45 (1.22–1.71) *** |
| 45–64 | 608 | 81,777 | 7.43 | 2.91 (2.61–3.24) *** | 1.83 (1.44–2.33) *** |
| ≥65 | 493 | 31,871 | 15.46 | 6.19 (5.52–6.94) *** | 2.85 (2.13–3.80) *** |
| Outpatient frequencies | |||||
| ≤3 (times) | 1157 | 270,863 | 4.27 | 1 (reference) | 1 (reference) |
| >3 | 1141 | 241,620 | 4.72 | 1.10 (1.01–1.19) * | 0.93 (0.82–1.04) |
| Hospitalization frequencies | |||||
| <1(times) | 1953 | 449,444 | 4.34 | 1 (reference) | 1 (reference) |
| ≥1 | 345 | 63,039 | 5.47 | 1.25 (1.11–1.40) *** | 1.12 (0.94–1.33) |
| Hearing loss | |||||
| No | 1885 | 468,142 | 4.02 | 1 (reference) | 1 (reference) |
| Yes | 413 | 44,341 | 9.31 | 2.32 (2.08–2.58) *** | 1.21 (1.20–1.42) * |
| Vertigo | |||||
| No | 1832 | 456,977 | 4.00 | 1 (reference) | 1 (reference) |
| Yes | 466 | 55,506 | 8.39 | 2.10 (1.90–2.33) *** | 1.00 (0.85–1.18) |
| Tinnitus | |||||
| No | 1851 | 459,547 | 4.02 | 1 (reference) | 1 (reference) |
| Yes | 447 | 52,936 | 8.44 | 2.11 (1.90–2.34) *** | 1.02 (0.86–1.20) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, P.-S.; Chiu, C.-C.; Fu, Y.-H.; Hsia, C.-C.; Yang, Y.-C.; Lee, K.-F.; Hsieh, S.-L.; Kuo, S.-J. Incidence of Hip Fractures among Patients with Chronic Otitis Media: The Real-World Data. Medicina 2022, 58, 1138. https://doi.org/10.3390/medicina58081138
Liao P-S, Chiu C-C, Fu Y-H, Hsia C-C, Yang Y-C, Lee K-F, Hsieh S-L, Kuo S-J. Incidence of Hip Fractures among Patients with Chronic Otitis Media: The Real-World Data. Medicina. 2022; 58(8):1138. https://doi.org/10.3390/medicina58081138
Chicago/Turabian StyleLiao, Pei-Shao, Ching-Chih Chiu, Yi-Hsiu Fu, Chia-Chun Hsia, Yu-Cih Yang, Kun-Feng Lee, Shang-Lin Hsieh, and Shu-Jui Kuo. 2022. "Incidence of Hip Fractures among Patients with Chronic Otitis Media: The Real-World Data" Medicina 58, no. 8: 1138. https://doi.org/10.3390/medicina58081138