
A Tension-Band Wiring Technique for Direct Fixation of a Chaput Tubercle Fracture: Technical Note

 , , ,
, , ,
Abstract
:1. Introduction
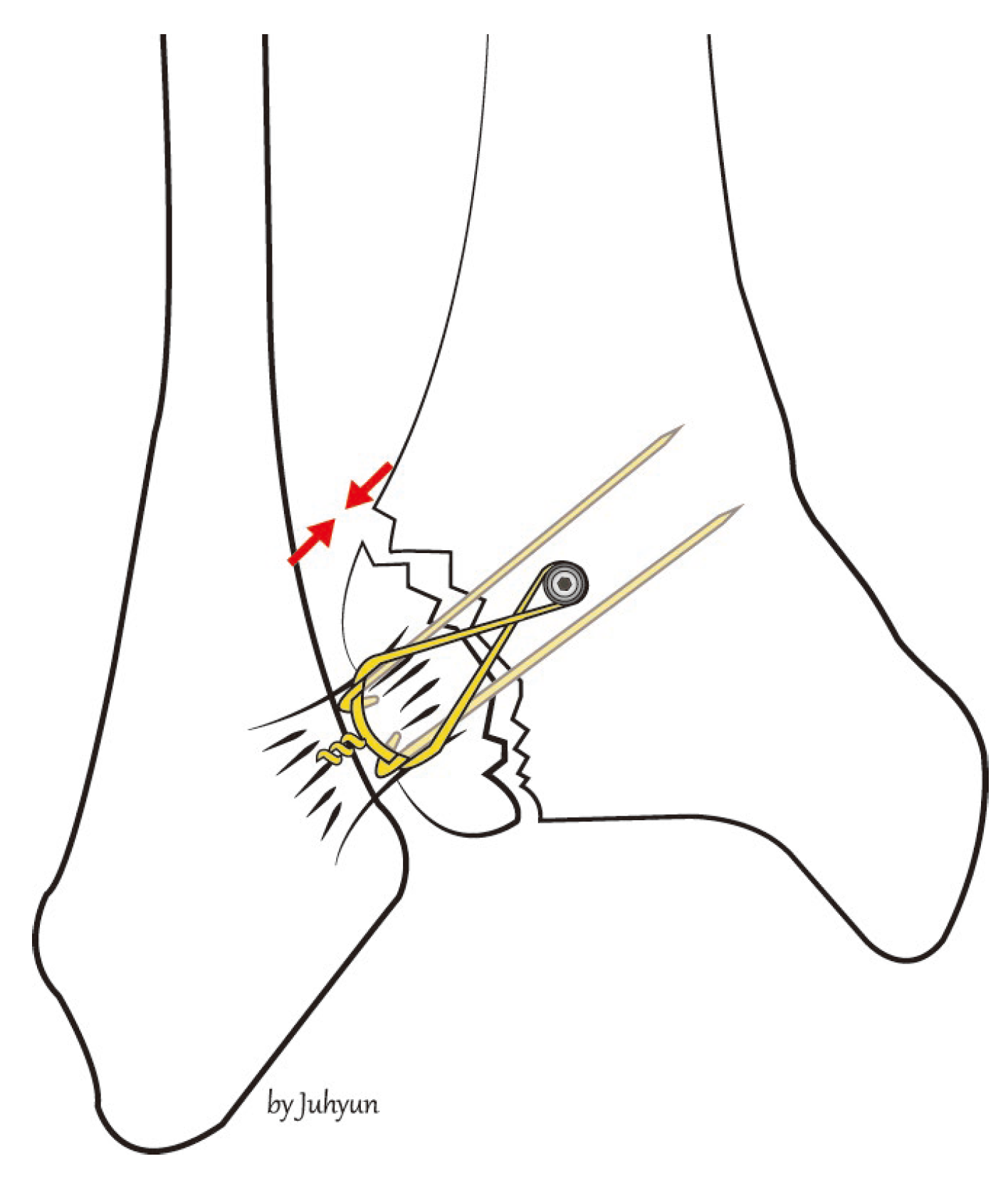
2. Surgical Technique
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AITFL | anterior inferior tibiofibular ligament |
| TBW | tension-band wiring |
| K | Kirschner |
| ROM | range-of-motion |
References
- Egol, K.A.; Pahk, B.; Walsh, M.; Tejwani, N.C.; Davidovitch, R.I.; Koval, K.J. Outcome after unstable ankle fracture: Effect of syndesmotic stabilization. J. Orthop. Trauma 2010, 24, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Van den Bekerom, M.P.; Lamme, B.; Hogervorst, M.; Bolhuis, H.W. Which ankle fractures require syndesmotic stabilization? J. Foot Ankle Surg. 2007, 46, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Court-Brown, C.M.; McBirnie, J.; Wilson, G. Adult ankle fractures: An increasing problem? Acta Orthop. Scand. 1998, 69, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Bartonícek, J. Anatomy of the tibiofibular syndesmosis and its clinical relevance. Surg. Radiol. Anat. 2003, 25, 379–386. [Google Scholar] [CrossRef]
- van Zuuren, W.J.; Schepers, T.; Beumer, A.; Sierevelt, I.; van Noort, A.; van den Bekerom, M.P.J. Acute syndesmotic instability in ankle fractures: A review. Foot Ankle Surg. 2017, 23, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Sagi, H.C.; Shah, A.R.; Sanders, R.W. The functional consequence of syndesmotic joint malreduction at a minimum 2-year follow-up. J. Orthop. Trauma 2012, 26, 439–443. [Google Scholar] [CrossRef]
- Ogilvie-Harris, D.J.; Reed, S.C. Disruption of the ankle syndesmosis: Diagnosis and treatment by arthroscopic surgery. Arthroscopy 1994, 10, 561–568. [Google Scholar] [CrossRef]
- Yuen, C.P.; Lui, T.H. Distal tibiofibular syndesmosis: Anatomy, biomechanics, injury and management. Open Orthop. J. 2017, 11, 670–677. [Google Scholar] [CrossRef] [Green Version]
- Chaput, H. Les Fractures Malléolaires du cou-de-pied et les Accidents du Travail; Masson et Cie: Paris, France, 1907. [Google Scholar]
- Chung, H.-J.; Bae, S.-Y.; Kim, M.-Y. Treatment of anteroinferior tibiofibular ligament avulsion fracture accompanied with ankle fracture. J. Korean Foot Ankle Soc. 2011, 15, 13–17. [Google Scholar]
- Bae, K.J.; Kang, S.B.; Kim, J.; Lee, J.; Go, T.W. Reduction and fixation of anterior inferior tibiofibular ligament avulsion fracture without syndesmotic screw fixation in rotational ankle fracture. J. Int Med. Res. 2020, 48, 300060519882550. [Google Scholar] [CrossRef] [Green Version]
- Gasparova, M.; Falougy, H.E.; Kubikova, E.; Almasi, J. Isolated “Tillaux” fracture in adulthood: Rarity where the key of success is not to miss it. Bratisl. Lek. Listy 2020, 121, 533–536. [Google Scholar] [CrossRef] [PubMed]
- Johnson, B.A.; Fallat, L.M. Comparison of tension-band wire and cancellous bone screw fixation for medial malleolar fractures. J. Foot Ankle Surg. 1997, 36, 284–289. [Google Scholar] [CrossRef]
- Haraguchi, N.; Toga, H.; Shiba, N.; Kato, F. Avulsion fracture of the lateral ankle ligament complex in severe inversion injury: Incidence and clinical outcome. Am. J. Sports Med. 2007, 35, 1144–1152. [Google Scholar] [CrossRef] [PubMed]
- Birnie, M.F.N.; van Schilt, K.L.J.; Sanders, F.R.K.; Kloen, P.; Schepers, T. Anterior inferior tibiofibular ligament avulsion fractures in operatively treated ankle fractures: A retrospective analysis. Arch. Orthop. Trauma Surg. 2019, 139, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Shu, H.; Li, W.; Liu, Y.; Shi, B.; Zheng, G. Clinical features and surgical effectiveness of ankle fractures involving Tillaux-Chaput in adults. Chin. J. Reparative Reconstr. Surg. 2015, 29, 288–291. [Google Scholar]
- Rammelt, S.; Bartoníček, J.; Kroker, L.; Neumann, A.P. Surgical fixation of quadrimalleolar fractures of the ankle. J. Orthop. Trauma 2021, 35, e216–e222. [Google Scholar] [CrossRef]
- Rammelt, S.; Boszczyk, A. Computed tomography in the diagnosis and treatment of ankle fractures: A critical analysis review. JBJS Rev. 2018, 6, e7. [Google Scholar] [CrossRef]
- Marx, C.; Schaser, K.D.; Rammelt, S. Early corrections after failed ankle fracture fixation. Z. Orthop. Unf. 2021, 159, 323–331. [Google Scholar] [CrossRef]
- Rammelt, S.; Bartoníček, J.; Schepers, T.; Kroker, L. Fixation of anterolateral distal tibial fractures: The anterior malleolus. Oper. Orthop. Traumatol. 2021, 33, 125–138. [Google Scholar] [CrossRef]
- Muller, M.; Allgower, M.; Schneider, R.; Willenegger, H. Screws and plates and their application. Man. Intern. Fixat. 1991, 3, 179–290. [Google Scholar]
- Kanakis, T.E.; Papadakis, E.; Orfanos, A.; Andreadakis, A.; Xylouris, E. Figure eight tension band in the treatment of fractures and pseudarthroses of the medial malleolus. Injury 1990, 21, 393–397. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pt. No. | Age | Sex | Cause | Lauge-Hansen Classification | Injury to Surgery Interval (hr) | * Procedure Time (min) | Injured Side | Follow-Up (mo) | OMAS | VAS Score | Interval to Union (wk) | Complications | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | |||||||||||
| 1 | 57 | F | S | SER IV | 138 | 19 | Left | 9 | 30 | 80 | 8 | 1 | 14 | None |
| 2 | 76 | F | S | SER IV | 118 | 20 | Left | 14 | 25 | 85 | 7 | 0 | 15 | None |
| 3 | 56 | F | S | SER II | 98 | 18 | Right | 6 | 30 | 90 | 8 | 0 | 14 | None |
| 4 | 39 | M | S | SER IV | 87 | 18 | Left | 13 | 35 | 95 | 8 | 0 | 12 | None |
| 5 | 58 | F | S | SER IV | 282 | 19 | Left | 12 | 0 | 80 | 9 | 1 | 14 | None |
| 6 | 79 | F | TA | PER IV | 97 | 17 | Left | 6 | 0 | 70 | 8 | 0 | 16 | None |
| 7 | 16 | M | TA | PER IV | 68 | 18 | Right | 4 | 40 | 95 | 8 | 0 | 13 | None |
| 8 | 17 | M | TA | PER II | 39 | 18 | Right | 4 | 30 | 90 | 7 | 0 | 12 | None |
| 9 | 53 | F | S | SER IV | 258 | 16 | Left | 3 | 0 | 60 | 9 | 0 | 14 | None |
| Mean | 50.1 | NA | NA | NA | 131.7 | 18.1 | NA | 7.9 | 21.1 | 82.8 | 8 | 0.2 | 13.8 | NA |
| SD | 22.5 | NA | NA | NA | 83.5 | 1.2 | NA | 4.2 | 164 | 11.8 | 0.7 | 0.4 | 1.3 | NA |
| p-value | 0.007 | 0.006 | ||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeo, E.-D.; Jung, K.-J.; Hong, Y.-C.; Hong, C.-H.; Lee, H.-S.; Won, S.-H.; Yoon, S.-J.; Kim, S.-H.; Ji, J.-Y.; Lee, D.-W.; et al. A Tension-Band Wiring Technique for Direct Fixation of a Chaput Tubercle Fracture: Technical Note. Medicina 2022, 58, 1005. https://doi.org/10.3390/medicina58081005
Yeo E-D, Jung K-J, Hong Y-C, Hong C-H, Lee H-S, Won S-H, Yoon S-J, Kim S-H, Ji J-Y, Lee D-W, et al. A Tension-Band Wiring Technique for Direct Fixation of a Chaput Tubercle Fracture: Technical Note. Medicina. 2022; 58(8):1005. https://doi.org/10.3390/medicina58081005
Chicago/Turabian StyleYeo, Eui-Dong, Ki-Jin Jung, Yong-Cheol Hong, Chang-Hwa Hong, Hong-Seop Lee, Sung-Hun Won, Sung-Joon Yoon, Sung-Hwan Kim, Jae-Young Ji, Dhong-Won Lee, and et al. 2022. "A Tension-Band Wiring Technique for Direct Fixation of a Chaput Tubercle Fracture: Technical Note" Medicina 58, no. 8: 1005. https://doi.org/10.3390/medicina58081005