
Changes Overtime in Perinatal Management and Outcomes of Extremely Preterm Infants in One Tertiary Care Romanian Center


Abstract
:1. Introduction
2. Materials and Methods
3. Results
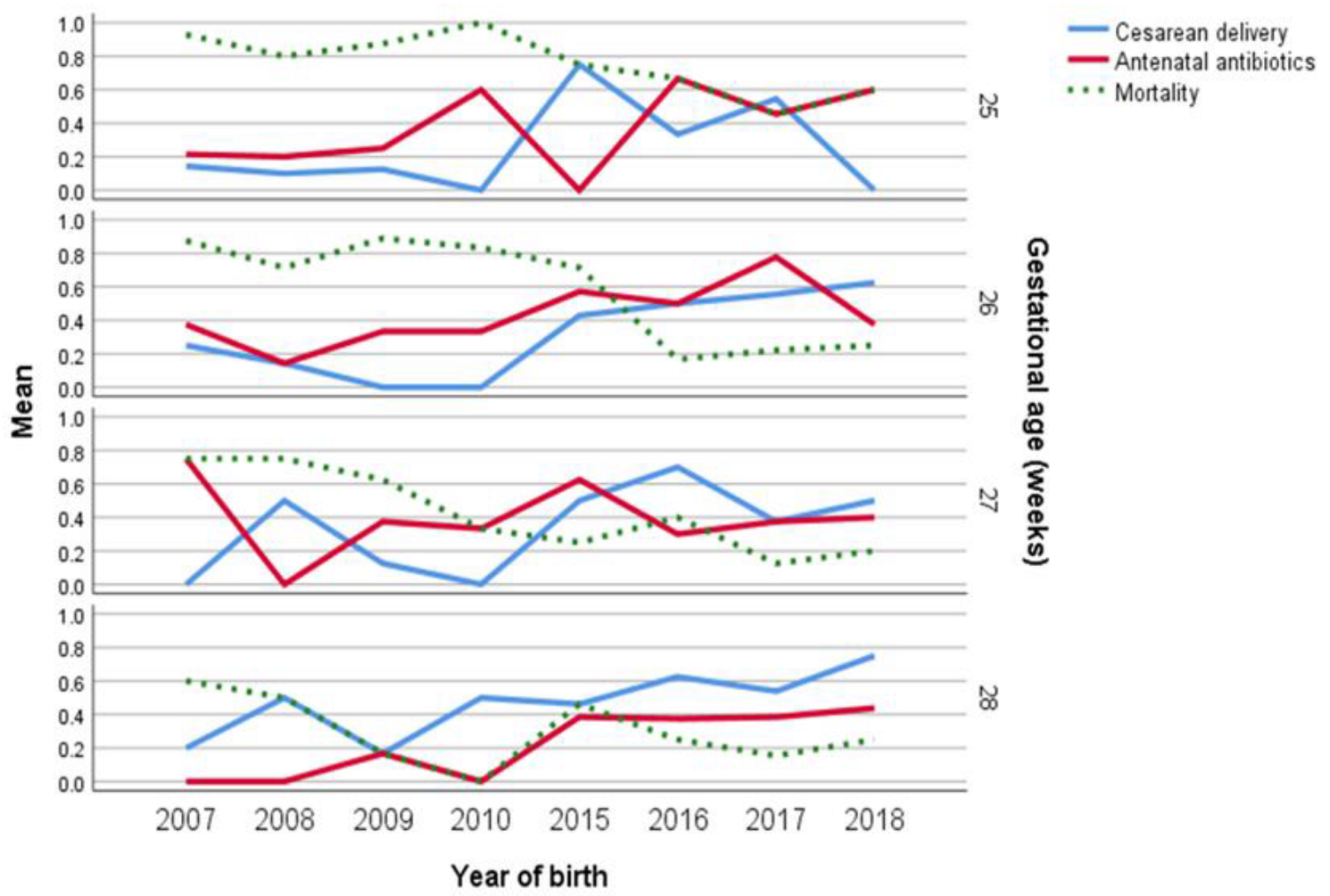
3.1. Study Population and Perinatal Interventions
3.2. Neonatal Characteristics
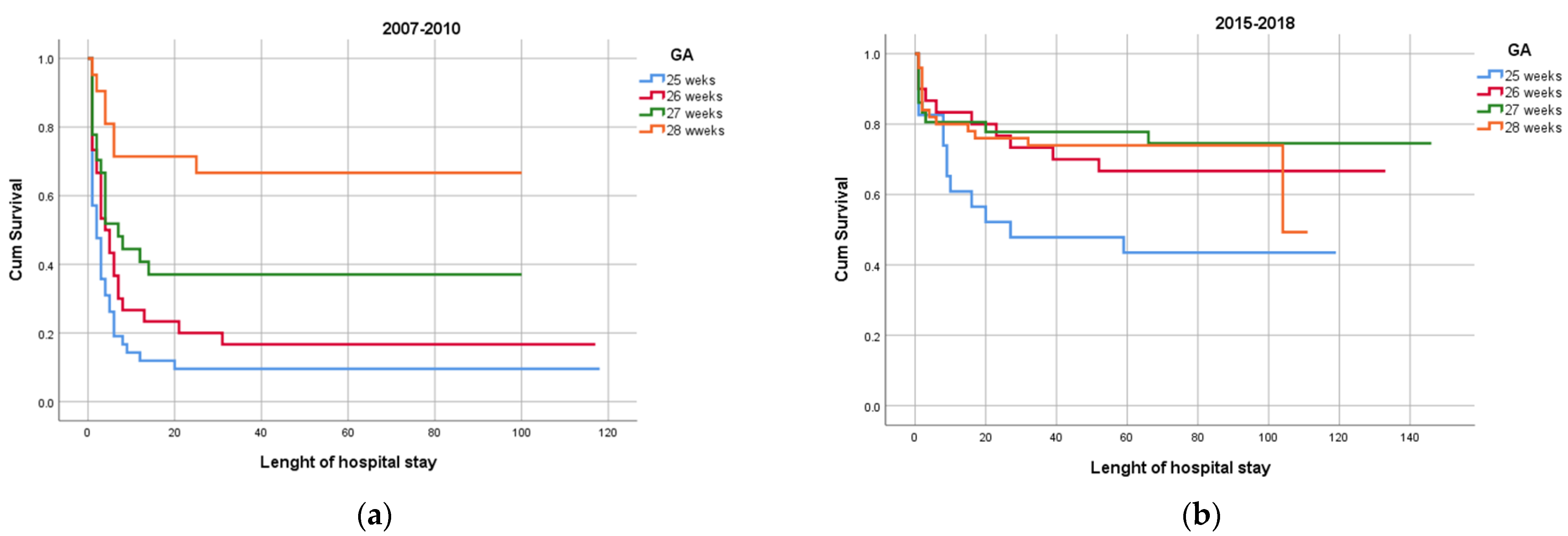
3.3. Neonatal Mortality
3.4. Neonatal Morbidities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Larroque, B.; Ancel, P.Y.; Marret, S.; Marchand, L.; André, M.; Arnaud, C.; Pierrat, V.; Rozé, J.C.; Messer, J.; Thiriez, G.; et al. Neurodevelopmental disabilities and special care of 5-year-old children born before 33 weeks of gestation (the EPIPAGE study): A longitudinal cohort study. Lancet 2008, 371, 813–820. [Google Scholar] [CrossRef]
- Ancel, P.Y.; Goffinet, F.; Kuhn, P.; Langer, B.; Matis, J.; Hernandorena, X.; Chabanier, P.; Joly-Pedespan, L.; Lecomte, B.; Vendittelli, F.; et al. Survival and morbidity of preterm children born at 22 through 34 weeks’ gestation in France in 2011: Results of the EPIPAGE-2 cohort study. JAMA Pediatr. 2015, 169, 230–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myrhaug, H.T.; Brurberg, K.G.; Hov, L.; Markestad, T. Survival and impairment of extremely premature infants: A meta-analysis. Pediatrics 2019, 143, e20180933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.B.; Narwal, R.; Adler, A.; Garcia, C.V.; Rohde, S.; Say, L.; et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012, 379, 2162–2172. [Google Scholar] [CrossRef] [Green Version]
- Stoll, B.J.; Hansen, N.I.; Bell, E.F.; Shankaran, S.; Laptook, A.R.; Walsh, M.C.; Hale, E.C.; Newman, N.S.; Schibler, K.; Carlo, W.A.; et al. Neonatal outcomes of extremely preterm infants from the NICHD Neonatal Research Network. Pediatrics 2010, 126, 443–456. [Google Scholar] [CrossRef] [Green Version]
- Younge, N.; Goldstein, R.F.; Bann, C.M.; Hintz, S.R.; Patel, R.M.; Smith, P.B.; Bell, E.F.; Rysavy, M.A.; Duncan, A.F.; Vohr, B.R.; et al. Eunice Kennedy Shriver National Institute of Child Health and Human Development neonatal research network. Survival and neurodevelopmental outcomes among periviable infants. N. Engl. J. Med. 2017, 376, 617–628. [Google Scholar] [CrossRef] [Green Version]
- Boland, R.A.; Cheong, J.L.; Doyle, L.W. Changes in long-term survival and neurodevelopmental disability in infants born extremely preterm in the post-surfactant era. Semin. Perinatol. 2021, 45, 151479. [Google Scholar] [CrossRef]
- Isayama, T. The clinical management and outcomes of extremely preterm infants in Japan: Past, present, and future. Transl Pediatr. 2019, 8, 199–211. [Google Scholar] [CrossRef]
- Helenius, K.; Sjörs, G.; Shah, P.S.; Modi, N.; Reichman, B.; Morisaki, N.; Kusuda, S.; Lui, K.; Darlow, B.A.; Bassler, D.; et al. Survival in very preterm infants: An international comparison of 10 national neonatal networks. Pediatrics 2017, 140, e20171264. [Google Scholar] [CrossRef] [Green Version]
- Jakuskiene, R.; Vollmer, B.; Saferis, V.; Daugeliene, D. Neonatal outcomes of very preterm infants admitted to a tertiary center in Lithuania between the years 2003 and 2005. Eur. J. Pediatr. 2011, 170, 1293–1303. [Google Scholar] [CrossRef]
- Toome, L.; Ringmets, I.; Andresson, P.; Saik, P.; Varendi, H.; Ilmoja, M.-L. Changes in care and short-term outcome for very preterm infants in Estonia. Acta Paediatr. 2012, 101, 390–396. [Google Scholar] [CrossRef]
- Suciu, L.M.; Puscasiu, L.; Cucerea, M.; Szabo, B.; Ognean, M.L.; Petrescu, O.; Sîmpălean, D.; Bell, E.F. Trends in outcomes of very preterm infants in Romania: A tale of three cities. Pediatr. Int. 2017, 59, 1157–1164. [Google Scholar] [CrossRef]
- Atwell, K.; Callander, E.; Lindsay, D.; Marshall, P.B.; Morris, S.A. Selection bias and outcomes for preterm neonates. Pediatrics 2018, 142, e20180470. [Google Scholar] [CrossRef] [Green Version]
- Smith, P.B.; Ambalavanan, N.; Li, L.; Cotten, C.M.; Laughon, M.; Walsh, M.C.; Das, A.; Bell, E.F.; Carlo, W.A.; Stoll, B.J.; et al. Approach to infants born at 22 to 24 weeks’ gestation: Relationship to outcomes of more-mature infants. Pediatrics 2012, 129, e1508–e1516. [Google Scholar] [CrossRef] [Green Version]
- Tchirikov, M.; Schlabritz-Loutsevitch, N.; Maher, J.; Buchmann, J.; Naberezhnev, Y.; Winarno, A.S.; Seliger, G. Mid-trimester preterm premature rupture of membranes (PPROM): Etiology, diagnosis, classification, international recommendations of treatment options and outcome. J. Perinat. Med. 2018, 46, 465–488. [Google Scholar] [CrossRef]
- Romero, R.; Chaemsaithong, P.; Korzeniewski, S.J.; Kusanovic, J.P.; Docheva, N.; Martinez-Varea, A.; Ahmed, A.I.; Yoon, B.H.; Hassan, S.S.; Chaiworapongsa, T.; et al. Clinical chorioamnionitis at term III: How well do clinical criteria perform in the identification of proven intra-amniotic infection? J. Perinat. Med. 2016, 44, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Fenton, T.R. A new growth chart for preterm babies: Babson and Benda’s chart updated with recent data and a new format. BMC Pediatr. 2003, 3, 13. [Google Scholar] [CrossRef] [Green Version]
- Jobe, A.H.; Bancalari, E. Bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef]
- Papile, L.A.; Munsick-Bruno, G.; Schaefer, A. Relationship of cerebral intraventricular hemorrhage and early childhood neurologic handicaps. J. Pediatrics 1983, 103, 273–277. [Google Scholar] [CrossRef]
- International Committee for the Classification of Retinopathy of Prematurity. The international classification of retinopathy of prematurity revisited. Arch. Ophthalmol. 2005, 123, 991–999. [Google Scholar] [CrossRef]
- Early Treatment for Retinopathy of Prematurity Cooperative Group. Revised indications for the treatment of retinopathy of prematurity: Results of the early treatment for retinopathy of prematurity randomized trial. Arch. Ophthalmol. 2003, 121, 1684–1694. [Google Scholar] [CrossRef] [Green Version]
- Lamau, M.C.; Ruiz, E.; Merrer, J.; Sibiude, J.; Huon, C.; Lepercq, J.; Goffinet, F.; Jarreau, P.H. A new individualized prognostic approach to the management of women at risk of extreme preterm birth in France: Effect on neonatal outcome. Arch. Pédiatrie. 2021, 28, 366–373. [Google Scholar] [CrossRef]
- Fischer, N.; Steurer, M.A.; Adams, M.; Berger, T.M. Survival rates of extremely preterm infants (gestational age < 26 weeks) in Switzerland: Impact of the Swiss guidelines for the care of infants born at the limit of viability. Arch. Dis. Child. Fetal Neonatal Ed. 2009, 94, F407–F413. [Google Scholar] [CrossRef] [Green Version]
- Rysavy, M.A.; Li, L.; Bell, E.F.; Das, A.; Hintz, S.R.; Stoll, B.J.; Vohr, B.R.; Carlo, W.A.; Shankaran, S.; Walsh, M.C.; et al. Between-hospital variation in treatment and outcomes in extremely preterm infants. N. Engl. J. Med. 2015, 372, 1801–1811. [Google Scholar] [CrossRef] [Green Version]
- Varga, P.; Berecz, B.; Gasparics, Á.; Dombi, Z.; Varga, Z.; Jeager, J.; Magyar, Z.; Rigó, J., Jr.; Joó, J.G.; Kornya, L. Morbidity and mortality trends in very–very low birth weight premature infants in light of recent changes in obstetric care. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 211, 134–139. [Google Scholar] [CrossRef] [Green Version]
- Stoelhorst, G.M.; Rijken, M.; Martens, S.E.; Brand, R.; den Ouden, A.L.; Wit, J.M.; Veen, S. Changes in neonatology: Comparison of two cohorts of very preterm infants (gestational age < 32 weeks): The Project On Preterm and Small for Gestational Age Infants 1983 and the Leiden Follow-Up Project on Prematurity 1996–1997. Pediatrics 2005, 115, 396–405. [Google Scholar] [CrossRef]
- Stoll, B.J.; Hansen, N.I.; Bell, E.; Walsh, M.C.; Carlo, W.A.; Shankaran, S.; Laptook, A.R.; Sánchez, P.J.; Van Meurs, K.P.; Wyckoff, M.H.; et al. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993–2012. JAMA 2015, 314, 1039–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boghossian, N.S.; Geraci, M.; Edwards, E.M.; Ehret, D.E.; Saade, G.R.; Horbar, J.D. Regional and racial–ethnic differences in perinatal interventions among periviable births. Obstet. Gynecol. 2020, 135, 885–895. [Google Scholar] [CrossRef] [PubMed]
- Ballot, D.; Ballot, N.S.; Rothberg, A.D. Reasons for failure to administer antenatal corticosteroids in preterm labour. S. Afr. Med. J. 1995, 85, 1005–1007. [Google Scholar] [PubMed]
- Ehret, D.E.Y.; Edwards, E.M.; Greenberg, L.T.; Bernstein, I.M.; Buzas, J.S.; Soll, R.F.; Horbar, J.D. Association of antenatal steroid exposure with survival among infants receiving postnatal life support at 22 to 25 weeks’ gestation. JAMA Netw. Open 2018, 1, e183235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McPherson, C.; Wambach, J.A. Prevention and treatment of respiratory distress syndrome in preterm neonates. Neonatal Netw. 2018, 37, 169–177. [Google Scholar] [CrossRef]
- Choi, Y.-B.; Lee, J.; Park, J.; Jun, Y.H. Impact of prolonged mechanical ventilation in very low birth weight infants: Results from a national cohort study. J. Pediatr. 2018, 194, 34–39. [Google Scholar] [CrossRef]
- Zysman-Colman, Z.; Tremblay, G.M.; Bandeali, S.; Landry, J.S. Bronchopulmonary dysplasia–trends over three decades. Paediatr. Child Health 2013, 18, 86–90. [Google Scholar] [CrossRef] [Green Version]
- Boghossian, N.S.; Geraci, M.; Lorch, S.A.; Phibbs, C.S.; Edwards, E.M.; Horbar, J.D. Racial and ethnic differences over time in outcomes of infants born less than 30 weeks’ gestation. Pediatrics 2019, 144, e20191106. [Google Scholar] [CrossRef]
- Budal, E.B.; Ebbing, C.; Kessler, J.; Bains, S.; Haugen, O.H.; Aukland, S.M.; Eide, G.E.; Halvorsen, T.; Bentsen, M.H.; Collett, K. Placental histology predicted adverse outcomes in extremely premature neonates in Norway—population-based study. Acta Paediatr. 2022, 111, 546–553. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Older Cohort N = 120 n (%) | Newer Cohort N = 139 n (%) | Overall N = 259 n (%) | p Value b |
|---|---|---|---|---|
| Maternal characteristics | ||||
| Maternal age mean (SD), years | 27.9 (6.7) | 29.1 (7.1) | 28.59 (7.0) | 0.1 |
| Maternal referral to tertiary care | 12 (9.0) | 0 | 12 (5.0) | 0.001 |
| Maternal hypertensive disorder a | 7 (6.0) | 10 (7.0) | 17 (7.0) | 0.6 |
| Gestational diabetes a | 0 | 1 (1.0) | 1 (0.1) | 0.3 |
| Chorioamnionitis | 23 (19.0) | 5 (4.0) | 28 (11.0) | 0.001 |
| Tocolysis | 22 (18.0) | 25 (18.0) | 47 (30.0) | 1.0 |
| Antenatal steroids | 35 (29.0) | 43 (31.0) | 78 (30.0) | 0.7 |
| Antenatal antibiotics | 33 (28.0) | 62 (45.0) | 95 (37.0) | 0.004 |
| PROM | 46 (38.0) | 50 (36.0) | 96 (37.0) | 0.2 |
| PROM latency interval, days Median (IQR) | 4 (12) | 1 (12) | 1 (12) | 0.6 |
| Cesarean section | 18 (15.0) | 75 (54.0) | 93 (36.0) | 0.001 |
| Newborn characteristics | ||||
| Male | 59 (49.0) | 76 (55.0) | 135 (52.0) | 0.3 |
| Fetal presentation vertex | 78 (65.0) | 81 (58.0) | 139 (53.6) | 0.2 |
| Twins | 22 (18.0) | 31 (22.0) | 53 (20.5) | 0.4 |
| Apgar score at 5 min < 7 | 92 (77.0) | 92 (66.0) | 184 (71.0) | 0.06 |
| Small for GA, <10th percentile on Fenton | 25 (21.0) | 29 (21.0) | 54 (21.0) | 0.9 |
| Blood cord pH < 7 | 30 (25.0) | 12 (8.6) | 42 (16.2) | 0.001 |
| Gestational age | 0.001 b | |||
| 25 weeks | 42 (35) | 23 (16.5) | 65 (25.1) | |
| 26 weeks | 30 (25) | 30 (21.6) | 60 (23.2) | |
| 27 weeks | 27 (22.5) | 36 (25.9) | 63 (24.3) | |
| 28 weeks | 21 (17.5) | 50 (35.9) | 71 (27.4) | |
| Gestational age at admission, median (IQR) | 26.2 (1.1) | 26.8 (1.1) | 26.0 (1.5) | 0.001 |
| Birth weight mean (SD), grams | 759.7 (162) | 951 (231) | 862 (223) | 0.001 |
| Newborn referral to tertiary care | 11 (9.0) | 20 (14.3) | 31 (12.0) | 0.1 |
| Surfactant administration | 26 (21.6) | 104 (75.0) | 130 (50.0) | 0.001 |
| Length of respiratory support, days, median (IQR) | 3 (5) | 10 (18) | 5 (10) | 0.001 |
| Length of NICU stay, days, median (IQR) | 4 (13) | 27 (35) | 14 (31) | 0.001 |
| Length of hospital stay, days, median (IQR) | 40 (62) | 71 (72) | 38 (81) | 0.001 |
| Variables | Older Cohort N = 120 n (%) | Newer Cohort N = 139 n (%) | Overall N = 259 n (%) | p Value a |
|---|---|---|---|---|
| IVH grade > III | 73 (60.9) | 36 (25.9) | 109 (42.0) | 0.001 |
| Mortality in the first 72 h age | 60 (50.0) | 24 (17.2) | 84 (32.4) | 0.001 |
| Mortality overall | ||||
| 25 weeks | 38/42 (90.5) | 13/23 (56.5) | 51/65 (78.0) | 0.001 |
| 26 weeks | 25/30 (83.3) | 10/30 (33.3) | 35/60 (58.3) | 0.28 |
| 27 weeks | 17/27 (62.9) | 9/36 (25.0) | 26/63 (41.2) | 0.08 |
| 28 weeks | 7/21 (33.3) | 14/50 (28.0) | 21/71 (29.5) | 0.001 |
| Infants who survived to discharged | 33 (27.5) | 93 (66.9) | 126 (48.7) | 0.001 |
| b BPD | 11 (33.3) | 31 (33.3) | 42 (33.3) | 0.9 |
| b ROP > III | 10 (33.3) | 26 (27.9) | 36 (28.6) | 0.4 |
| b NEC | 1 (3.03) | 16 (17.2) | 17 (13.5) | 0.001 |
| Mortality Older Cohort OR 95% CI | Mortality Newer Cohort OR 95% CI | IVH Grade > III Older Cohort OR 95% CI | IVH Grade > III Newer Cohort OR 95% CI | |
|---|---|---|---|---|
| 25 weeks | 5.62 (1.82–17.37) | 3.27 (1.31–8.18) | 2.88 (1.25–6.67) | 4.18 (1.64–10.63) |
| 26 weeks | 2.25 (0.78–6.51) | 1.01 (0.43–2.39) | 1.39 (0.58–3.32) | 0.84 (0.32–2.16) |
| 27 weeks | 0.55 (0.22–1.39) | 0.59 (0.25–1.39) | 0.75 (0.31–1.79) | 0.48 (0.18–1.28) |
| 28 weeks a | Reference | Reference | Reference | Reference |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ungureanu, D.; Boghossian, N.S.; Suciu, L.M. Changes Overtime in Perinatal Management and Outcomes of Extremely Preterm Infants in One Tertiary Care Romanian Center. Medicina 2022, 58, 1019. https://doi.org/10.3390/medicina58081019
Ungureanu D, Boghossian NS, Suciu LM. Changes Overtime in Perinatal Management and Outcomes of Extremely Preterm Infants in One Tertiary Care Romanian Center. Medicina. 2022; 58(8):1019. https://doi.org/10.3390/medicina58081019
Chicago/Turabian StyleUngureanu, Diana, Nansi S. Boghossian, and Laura Mihaela Suciu. 2022. "Changes Overtime in Perinatal Management and Outcomes of Extremely Preterm Infants in One Tertiary Care Romanian Center" Medicina 58, no. 8: 1019. https://doi.org/10.3390/medicina58081019