
Online Learning versus Hands-On Learning of Basic Ocular Ultrasound Skills: A Randomized Controlled Non-Inferiority Trial

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
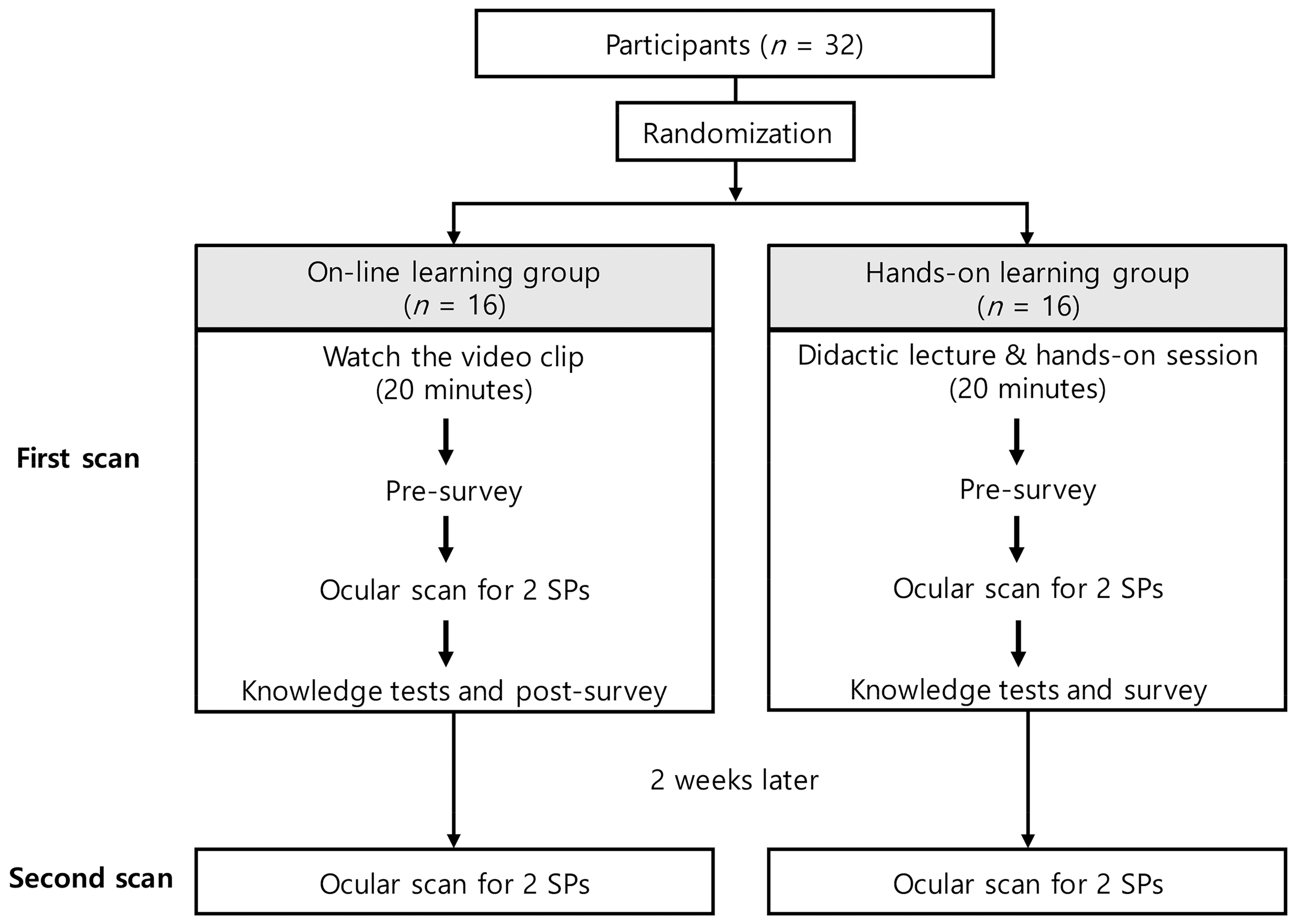
2.1. Study Design
2.2. Participants
2.3. Study Protocol
2.4. Ocular POCUS
2.5. Data Collection
2.6. Outcomes
2.7. Sample Size and Statistical Analysis
3. Results
3.1. Differences in Ocular POCUS Scores between Groups
3.2. Maintenance Evaluation of Ocular POCUS Skill after 2 Weeks
3.3. Time Taken to Scan
3.4. ONSD Measurement
3.5. Knowledge Test and Post-Survey
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Pre-Survey | |
| 1. How often do you usually use ultrasound in your work? (Frequency of POCUS use) | |
| Response set | Always–Often–Usually–Sometimes–Seldom |
| 2. Can you scan and interpret the views you want with ultrasound? (Confidence in POCUS scanning and interpretation) | |
| Response set | Strongly Disagree (1)–Disagree (2)–Neutral (3)–Agree (4)–Strongly Agree (5) |
| 3. How many ocular ultrasound scans have you performed? (Number of ocular ultrasound scans before education) | |
| Response set | 0 – 1–2 – 3–5 – 6–10 – >10 |
| Post-Survey | |
| 1. Do you agree that ocular ultrasound education is necessary? (Necessity of ocular ultrasound training) | |
| Response set | Strongly Disagree (1)–Disagree (2)–Neutral (3)–Agree (4)–Strongly Agree (5) |
| 2. How satisfied are you with the training method you received? (Subjective satisfactory of training method received) | |
| Response set | Strongly Disagree (1)–Disagree (2)–Neutral (3)–Agree (4)–Strongly Agree (5) |
| 3. What do you think about the training time you received? (Adequacy of training time) | |
| Response set | Very insufficient (1)–Insufficient (2)–Neutral (3)–Sufficient (4)–Very sufficient (5) |
| 4. Did your confidence in ocular ultrasound improve after the training? (Confidence improvement after training) | |
| Response set | Strongly Disagree (1)–Disagree (2)–Neutral (3)–Agree (4)–Strongly Agree (5) |
| SP1_Rt_eye | SP1_Lt_eye | SP2_Rt_eye | SP2_Lt_eye | ||
|---|---|---|---|---|---|
| Scan score (0–21) | |||||
| Setting (probe/gain/depth, 0–3) | |||||
| Transverse plane | |||||
| Mid-eye view (0–3) | |||||
| Tilting view (0–3) | |||||
| Four directions view (0–3) | |||||
| Sagittal plane | |||||
| Mid-eye view (0–3) | |||||
| Tilting view (0–3) | |||||
| Four directions view (0–3) | |||||
| ONSD score (0–4) | |||||
| Total score (0–25) | |||||
| First Scan | Second Scan | |||||
|---|---|---|---|---|---|---|
| Group O | Group H | p-Value | Group O | Group H | p-Value | |
| SP1_Rt_eye | ||||||
| Total score | 21.4 (1.99) | 21.1 (1.55) | 0.623 | 20.8 (2.59) | 20.3 (2.02) | 0.547 |
| Scan score | 18.5 (17–19.25) | 19 (17.25–19.75) | 0.491 | 17.9 (2.1) | 17.4 (1.86) | 0.481 |
| ONSD score | 3.75 (3, 4) | 3.25 (1, 3.5) | 0.065 | 3.25 (2, 4) | 3 (2.5, 4) | 0.923 |
| SP1_Lt_eye | ||||||
| Total score | 22.6 (1.38) | 21.9 (1.83) | 0.241 | 22 (21–23) | 21.75 (20.25–23) | 0.662 |
| Scan score | 18.8 (1.4) | 18.9 (1.71) | 0.737 | 18.75 (18–19) | 18.5 (17–19.25) | 0.646 |
| ONSD score | 4 (4–4) | 3.74 (2.5–4) | 0.038 * | 4 (3–4) | 4 (3.75–4) | 0.566 |
| SP2_Rt_eye | ||||||
| Total score | 20.7 (2.71) | 20.4 (1.95) | 0.795 | 20.9 (1.47) | 20.0 (2.31) | 0.227 |
| Scan score | 18.1 (2.02) | 18.2 (1.65) | 0.887 | 18 (1.14) | 17.6 (1.46) | 0.388 |
| ONSD score | 2.75 (2–3.25) | 2.75 (1–3.5) | 0.577 | 3 (2, 4) | 2.5 (1, 4) | 0.482 |
| SP2_Lt_eye | ||||||
| Total score | 22 (1.97) | 21.9 (1.49) | 0.920 | 22.5 (1.15) | 22.3 (1.59) | 0.659 |
| Scan score | 19.1 (1.28) | 18.9 (1.42) | 0.747 | 19.0 (0.94) | 19.1 (1.19) | 0.870 |
| ONSD score | 3.25 (2–4) | 3.5 (2.25–4) | 0.877 | 4 (3.25–4) | 3.5 (2.75–4) | 0.423 |
| First Scan | Second Scan | |||||
|---|---|---|---|---|---|---|
| Group O | Group H | p-Value | Group O | Group H | p-Value | |
| SP1_Rt_eye | 568 (171) | 486 (141) | 0.150 | 440 (133) | 429 (141) | 0.687 |
| SP1_Lt_eye | 349 (294–529) | 292 (239–377) | 0.147 | 261 (206–381) | 283 (248–299) | 0.651 |
| SP2_Rt_eye | 428 (383–476) | 391 (317–567) | 0.865 | 292 (252–364) | 435 (272–486) | 0.097 |
| SP2_Lt_eye | 317 (254–420) | 315 (235–373) | 0.895 | 241 (199–285) | 233 (204–270) | 0.763 |
| Total time | 1747 (1562–1994) | 1532 (1440–1634) | 0.07 | 1339 (463) | 1378 (378) | 0.791 |
| First Scan | Second Scan | |||||
|---|---|---|---|---|---|---|
| Estimate (SE) | 95% CI | p-Value | Estimate (SE) | 95% CI | p-Value | |
| Intercept | 486 (34.1) | (419–553) | <0.0001 | 420 (34.2) | (353–487) | <0.0001 |
| Group O vs. H | 81.9 (53.6) | (−23.2–187.1) | 0.127 | 19.8 (47.0) | (−72.3–112) | 0.674 |
| Scan sequence | ||||||
| 2 vs. 1 | −154 (31.6) | (−198–−110) | <0.0001 * | −121 (30.2) | (−162–−79) | <0.0001 * |
| 3 vs. 1 | −27.1 (56.3) | (−105–50.7) | >0.999 | −6.13 (28.3) | (−45.2–33.0) | >0.999 |
| 4 vs. 1 | −147 (40.6) | (−203–−91) | 0.0009 * | −176 (39.8) | (−231–−121) | <0.0001 * |
| ONSD Values (mm) (Reference Value) | First Scan | Second Scan | ||||
|---|---|---|---|---|---|---|
| Group O | Group H | p-Value | Group O | Group H | p-Value | |
| SP1_Rt_eye (4.7) | 4.79 ± 0.66 | 4.63 ± 0.94 | 0.585 | 4.39 ± 0.98 | 4.81 ± 0.74 | 0.199 |
| SP1_Lt_eye (5) | 5.18 ± 0.63 | 4.81 ± 0.65 | 0.128 | 5.15 [4.6–5.65] | 4.9 [4.5–5.4] | 0.488 |
| SP2_Rt_eye (5.3) | 5.27 ± 1.2 | 5.74 ± 1.52 | 0.345 | 5.16 ± 1.02 | 5.49 ± 1.03 | 0.377 |
| SP2_Lt_eye (5) | 5.16 ± 0.9 | 5.3 ± 1.19 | 0.705 | 5.29 ± 0.84 | 5.45 ± 0.91 | 0.620 |
| p-Value | First Scan | Second Scan | ||
|---|---|---|---|---|
| Group O | Group H | Group O | Group H | |
| SP1_Rt_eye | 0.580 | 0.788 | 0.232 | 0.586 |
| SP1_Lt_eye | 0.271 | 0.302 | 0.874 | 0.836 * |
| SP2_Rt_eye | 0.919 | 0.281 | 0.599 | 0.478 |
| SP2_Lt_eye | 0.496 | 0.345 | 0.198 | 0.073 |
| All eyes | 0.559 † | 0.776 † | 0.198 † | 0.564 † |
References
- Whitson, M.R.; Mayo, P.H. Ultrasonography in the emergency department. Crit. Care 2016, 20, 227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frasure, S.E.; Saul, T.; Lewiss, R.E. Bedside ultrasound diagnosis of vitreous hemorrhage and traumatic lens dislocation. Am. J. Emerg. Med. 2013, 31, 1002.e1–1002.e2. [Google Scholar] [CrossRef] [PubMed]
- Shinar, Z.; Chan, L.; Orlinsky, M. Use of ocular ultrasound for the evaluation of retinal detachment. J. Emerg. Med. 2011, 40, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Shiver, S.A.; Lyon, M.; Blaivas, M. Detection of metallic ocular foreign bodies with handheld sonography in a porcine model. J. Ultrasound Med. 2005, 24, 1341–1346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blaivas, M.; Theodoro, D.; Sierzenski, P.R. Elevated intracranial pressure detected by bedside emergency ultrasonography of the optic nerve sheath. Acad. Emerg. Med. 2003, 10, 376–381. [Google Scholar] [CrossRef]
- Tayal, V.S.; Neulander, M.; Norton, H.J.; Foster, T.; Saunders, T.; Blaivas, M. Emergency department sonographic measurement of optic nerve sheath diameter to detect findings of increased intracranial pressure in adult head injury patients. Ann. Emerg. Med. 2007, 49, 508–514. [Google Scholar] [CrossRef]
- Blaivas, M.; Theodoro, D.; Sierzenski, P.R. A study of bedside ocular ultrasonography in the emergency department. Acad. Emerg. Med. 2002, 9, 791–799. [Google Scholar] [CrossRef] [Green Version]
- Kilker, B.A.; Holst, J.M.; Hoffmann, B. Bedside ocular ultrasound in the emergency department. Eur. J. Emerg. Med. 2014, 21, 246–253. [Google Scholar] [CrossRef]
- Lazarow, F.; Deal, A.K.; Shaves, S.C.; Knapp, B.; Byars, D.; Goodmurphy, C.W.; Trace, A.P.; Nunez, D.; Elzie, C.A. Evaluation of a point-of-care ultrasound curriculum and ocular phantom in residency training. J. Ultrasound 2021, 25, 259–263. [Google Scholar] [CrossRef]
- Physicians ACoE. Emergency ultrasound guidelines. Ann. Emerg. Med. 2009, 53, 550–570. [Google Scholar] [CrossRef]
- Eke, O.F.; Henwood, P.C.; Wanjiku, G.W.; Fasina, A.; Kharasch, S.J.; Shokoohi, H. Global point-of-care ultrasound education and training in the age of COVID-19. Int. J. Emerg. Med. 2021, 14, 12. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, A.J.; Eke, O.F.; Alhassan Al Saud, A.; Al Mulhim, A.; Kharasch, S.; Huang, C.; Liteplo, A.S.; Shokoohi, H. Remodeling Point-of-care Ultrasound Education in the Era of COVID-19. AEM Educ. Train. 2020, 4, 321–324. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.D. A Virtual Point-of-care Ultrasound Course During the COVID-19 Pandemic. AEM Educ. Train. 2020, 5, 102–104. [Google Scholar] [CrossRef] [PubMed]
- MacKenzie, J.D.; Greenes, R.A. The World Wide Web: Redefining medical education. JAMA 1997, 278, 1785–1786. [Google Scholar] [CrossRef]
- Simone, R.; Josh, G.; Abbas, H. Free open access medical education for point of care ultrasound: Content discovery and resource evaluation. Clin. Exp. Emerg. Med. 2021, 8, 71–73. [Google Scholar] [CrossRef]
- Chenkin, J.; Lee, S.; Huynh, T.; Bandiera, G. Procedures can be learned on the Web: A randomized study of ultrasound-guided vascular access training. Acad. Emerg. Med. 2008, 15, 949–954. [Google Scholar] [CrossRef]
- Edrich, T.; Stopfkuchen-Evans, M.; Scheiermann, P.; Heim, M.; Chan, W.; Stone, M.B.; Dankl, D.; Aichner, J.; Hinzmann, D.; Song, P.; et al. A Comparison of Web-Based with Traditional Classroom-Based Training of Lung Ultrasound for the Exclusion of Pneumothorax. Anesth. Analg. 2016, 123, 123–128. [Google Scholar] [CrossRef] [Green Version]
- Krishnan, S.; Kuhl, T.; Ahmed, W.; Togashi, K.; Ueda, K. Efficacy of an online education program for ultrasound diagnosis of pneumothorax. Anesthesiology 2013, 118, 715–721. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, B.; Schafer, J.M.; Dietrich, C.F. Emergency Ocular Ultrasound—Common Traumatic and Non-Traumatic Emergencies Diagnosed with Bedside Ultrasound. Ultraschall Med. 2020, 41, 618–645. [Google Scholar] [CrossRef]
- Soni, N.J.; Arntfield, R.; Kory, P. Point-of-Care Ultrasound; Elsevier Saunders: Philadelphia, PA, USA, 2015; pp. 245–253. [Google Scholar]
- Yamamoto, K.; Inagaki, Y.; Iwata, C.; Tada, M.; Tateoka, K.; Sasakawa, T. Ultrasound-guided internal jugular venipuncture using pocket-sized versus standard ultrasound devices: A prospective non-inferiority trial. J. Med. Ultrason. 2021, 48, 639–644. [Google Scholar] [CrossRef]
- Lahham, S.; Shniter, I.; Thompson, M.; Le, D.; Chadha, T.; Mailhot, T.; Kang, T.L.; Chiem, A.; Tseeng, S.; Fox, J.C. Point-of-Care Ultrasonography in the Diagnosis of Retinal Detachment, Vitreous Hemorrhage, and Vitreous Detachment in the Emergency Department. JAMA Netw. Open 2019, 2, e192162. [Google Scholar] [CrossRef] [PubMed]
- Ojaghi Haghighi, S.; Morteza Begi, H.; Sorkhabi, R.; Tarzamani, M.; Kamali Zonouz, G.; Mikaeilpour, A.; Rahmani, F. Diagnostic Accuracy of Ultrasound in Detection of Traumatic Lens Dislocation. Emergency 2014, 2, 121–124. [Google Scholar] [PubMed]
- Reznick, R.K.; MacRae, H. Teaching Surgical Skills—Changes in the Wind. N. Engl. J. Med. 2006, 355, 2664–2669. [Google Scholar] [CrossRef] [Green Version]
- Winder, C.B.; LeBlanc, S.J.; Haley, D.B.; Lissemore, K.D.; Godkin, M.A.; Duffield, T.F. Comparison of online, hands-on, and a combined approach for teaching cautery disbudding technique to dairy producers. J. Dairy Sci. 2018, 101, 840–849. [Google Scholar] [CrossRef]
- Fatonia Arifiatib, N.; Nurkhayatic, E.; Nurdiawatid, E.; Fidziahe Pamungkasf, G.; Adha, S.; Irawan Agus, P.; Octoberry, J. University Students Online Learning System During Covid-19 Pandemic: Advantages, Constraints and Solutions. Sys. Rev. Pharm. 2020, 11, 570–576. [Google Scholar]
- Keis, O.; Grab, C.; Schneider, A.; Ochsner, W. Online or face-to-face instruction? A qualitative study on the electrocardiogram course at the University of Ulm to examine why students choose a particular format. BMC Med. Educ. 2017, 17, 194. [Google Scholar] [CrossRef]
- Mukhtar, K.; Javed, K.; Arooj, M.; Sethi, A. Advantages, Limitations and Recommendations for online learning during COVID-19 pandemic era. Pak. J. Med. Sci. 2020, 36, S27–S31. [Google Scholar] [CrossRef]
- Kim, J.; Cho, Y.; Kim, Y.; Ha, Y.; Kang, B.; Chung, H.; Park, Y.; An, J.; Do, H.; Hong, H. Development of an Emergency Abdominal Ultrasound Course in Korea 1-year Experience. J. Korean Soc. Emerg. Med. 2010, 21, 382–387. [Google Scholar]
- Sim, W.S.; Lee, S.H.; Yun, S.J.; Ryu, S.; Choi, S.W.; Kim, H.J.; Kang, T.K.; Oh, S.C.; Cho, S.J. Comparative and retrospective evaluation of the predictive performance of optic nerve sheath thickness and optic nerve sheath diameter for traumatic brain injury using facial computed tomography. Clin. Exp. Emerg. Med. 2020, 7, 122–130. [Google Scholar] [CrossRef]
- Hassen, G.W.; Bruck, I.; Donahue, J.; Mason, B.; Sweeney, B.; Saab, W.; Weedon, J.; Patel, N.; Perry, K.; Matari, H.; et al. Accuracy of optic nerve sheath diameter measurement by emergency physicians using bedside ultrasound. J. Emerg. Med. 2015, 48, 450–457. [Google Scholar] [CrossRef]
- Potgieter, D.W.; Kippin, A.; Ngu, F.; Mckean, C. Can accurate ultrasonographic measurement of the optic nerve sheath diameter (a non-invasive measure of intracranial pressure) be taught to novice operators in a single training session? Anaesth. Intensive Care 2011, 39, 95–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]


| Online Group (Group O, n = 16) | Hands-On Group (Group H, n = 16) | p-Value | |
|---|---|---|---|
| Physician-grade interns/EM 1/EM 2/EM 3/EM 4 | 7(45)/4(25)/2(12)/2(12)/1(6) | 8(50)/-/2(12)/3(19)/3(19) | 0.301 |
| Age (mean, SD) | 29 (3) | 30 (3) | 0.283 |
| Male | 8 | 6 | 0.476 |
| Frequency of POCUS use | |||
| Seldom/sometimes/usually/often-always | 2(12)/4(25)/3(19)/7(44) | 5(31)/5(31)/1(7)/5(31) | 0.662 |
| Confidence of POCUS scan | |||
| 1/2/3/4/5 (Likert Scale) | -/4(25)/7(44)/5(31)/- | -/3(19)/7(43)/3(19)/3(19) | 0.392 |
| Number of previous ocular POCUS scan | |||
| 0/1–5/6–10/>10 | 11(69)/4(25)/1(6)/- | 10(63)/5(31)/1(6)/- | 0.499 |
| Group O | Group H | Non-Inferiority Margin (Δ) | Difference of Group Least Squares Means (95% CI) (Group O Minus Group H) | ||
|---|---|---|---|---|---|
| First scan | |||||
| Total score | 21.7 (0.35) | 21.3 (0.25) | −2 |  | 0.35 (−0.48 to 1.17) |
| Scan score | 18.5 (0.28) | 18.6 (0.27) | −2 |  | −0.13 (−1.00 to 0.74) |
| ONSD score | 3.19 (0.14) | 2.67 (0.24) | −1 |  | 0.53 (−0.10 to 1.16) |
| Second scan | |||||
| Total score | 21.5 (0.34) | 21.0 (0.32) | −2 |  | 0.49 (−0.63 to 1.61) |
| Scan score | 18.3 (0.22) | 18.1 (0.23) | −2 |  | 0.23 (−0.54 to 1.01) |
| ONSD score | 3.18 (0.16) | 2.99 (0.26) | −1 |  | 0.20 (−0.60 to 0.99) |
| First Scan | Second Scan | Difference of Group Least Squares Means (95% CI) (Second Minus First Scan) | ||
|---|---|---|---|---|
| Total score | 21.4 (0.22) | 21.5 (0.26) |  | 0.03 (−0.70 to 0.76) |
| Scan score | 18.5 (0.20) | 18.3 (0.12) |  | −0.26 (−0.73 to 0.21) |
| ONSD score | 2.93 (0.14) | 3.08 (0.15) |  | 0.16 (−0.10 to 0.41) |
| Group O | Group H | p-Value | |
|---|---|---|---|
| Knowledge test | 16 (15, 18) | 17 (16, 18) | 0.347 |
| Necessity of ocular ultrasound training | |||
| 1–2/3/4–5 | -/2(12)/14(88) | -/1(6)/15(94) | 0.776 |
| Subjective satisfaction with training method received | |||
| 1–2/3/4–5 | 1(6)/3(19)/12(75) | -/-/16(100) | <0.001 * |
| Adequacy of training time | |||
| 1–2/3/4–5 | 3(19)/5(31)/8(50) | 1(6)/4(25)/11(69) | 0.781 |
| Confidence improvement after training | |||
| 1–2/3/4–5 | -/3(19)/13(81) | -/2(12)/14(88) | 0.084 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, S.-Y.; Yoo, J.; Park, S.; Jo, I.-J.; Kim, S.; Cho, H.; Lee, G.; Park, J.-E.; Kim, T.; Lee, S.-U.; et al. Online Learning versus Hands-On Learning of Basic Ocular Ultrasound Skills: A Randomized Controlled Non-Inferiority Trial. Medicina 2022, 58, 960. https://doi.org/10.3390/medicina58070960
Kang S-Y, Yoo J, Park S, Jo I-J, Kim S, Cho H, Lee G, Park J-E, Kim T, Lee S-U, et al. Online Learning versus Hands-On Learning of Basic Ocular Ultrasound Skills: A Randomized Controlled Non-Inferiority Trial. Medicina. 2022; 58(7):960. https://doi.org/10.3390/medicina58070960
Chicago/Turabian StyleKang, Soo-Yeon, Jonghoon Yoo, Sookyung Park, Ik-Joon Jo, Seonwoo Kim, Hyun Cho, Guntak Lee, Jong-Eun Park, Taerim Kim, Se-Uk Lee, and et al. 2022. "Online Learning versus Hands-On Learning of Basic Ocular Ultrasound Skills: A Randomized Controlled Non-Inferiority Trial" Medicina 58, no. 7: 960. https://doi.org/10.3390/medicina58070960