
Iron Status in Pregnant Women in Latvia: An Epidemiological, Cross-Sectional, Multicenter Study According to WHO and UK Criteria

 and
and
Abstract
:1. Introduction
2. Materials and Methods
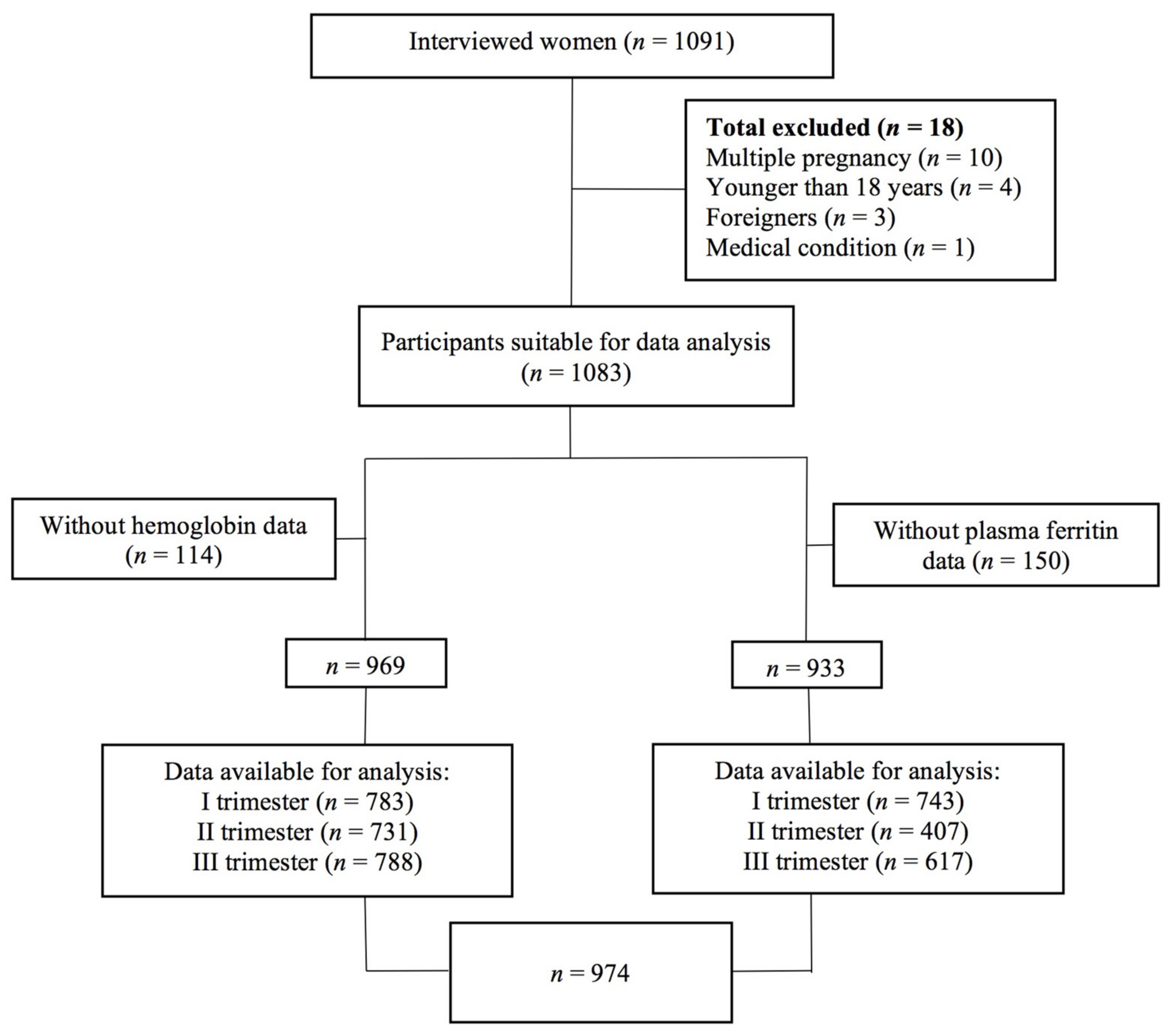
2.1. Study Design and Participants
2.2. Data Collection
2.3. Operational Definitions and Definitions of Terms
2.3.1. Iron Deficiency Anaemia in Pregnancy
2.3.2. Iron Deficiency in Pregnancy
2.4. Ethical Considerations
2.5. Data Analysis
3. Results
3.1. Iron Status in All Trimesters
3.2. Sociodemographic Characteristics
3.3. Associations between ID Anaemia and Sociodemographic Data
3.4. Dietary Iron Intake and Supplement Use
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization; Centres for Disease Control and Prevention. The Global Prevalence of Anaemia in 2011; WHO: Geneva, Switzerland, 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/177094/9789241564960_eng.pdf (accessed on 20 June 2021).
- Stevens, G.A.; Finucane, M.M.; De-Regil, L.M.; Paciorek, C.J.; Flaxman, S.R.; Branca, F.; Peña-Rosas, J.P.; Bhutta, Z.A.; Ezzati, M.; on behalf of Nutrition Impact Model Study Group (Anaemia). Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: A systematic analysis of population-representative data. Lancet Glob. Health 2013, 1, e16–e25. [Google Scholar] [CrossRef] [Green Version]
- Alwan, N.A.; Cade, J.E.; McArdle, H.J.; Greenwood, D.C.; Hayes, H.E.; Simpson, N.A.B. Maternal iron status in early pregnancy and birth outcomes: Insights from the Baby’s Vascular health and Iron in Pregnancy study. Br. J. Nutr. 2015, 113, 1985–1992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quezada-Pinedo, H.; Cassel, F.; Duijts, L.; Muckenthaler, M.; Gassmann, M.; Jaddoe, V.; Reiss, I.; Vermeulen, M. Maternal Iron Status in Pregnancy and Child Health Outcomes after Birth: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 2221. [Google Scholar] [CrossRef]
- Killip, S.; Bennett, J.M.; Chambers, M.D. Iron deficiency anemia. Am. Fam. Physician 2007, 75, 671–678. [Google Scholar] [PubMed]
- Markova, V.; Nørgaard, A.; Jørgensen, K.J.; Langhoff-Roos, J. Treatment for women with postpartum iron deficiency anaemia. Cochrane Database Syst. Rev. 2013, 8, CD010861. [Google Scholar] [CrossRef]
- Drukker, L.; Hants, Y.; Farkash, R.; Ruchlemer, R.; Samueloff, A.; Grisaru-Granovsky, S. Iron defi- ciency anemia at admission for labor and delivery is associated with an increased risk for Cesarean section and adverse maternal and neonatal outcomes. Transfusion 2015, 55, 2799–2806. [Google Scholar] [CrossRef]
- Zimmermann, M.B.; Burgi, H.; Hurrell, R.F. Iron deficiency predicts poor maternal thyroid status during pregnancy. J. Clin. Endocrinol. Metab. 2007, 92, 3436–3440. [Google Scholar] [CrossRef] [Green Version]
- Rogne, T.; Burgess, S.; Gill, D. Systemic iron status and maternal pregnancy complications: A Mendelian randomization study. Int. J. Epidemiol. 2022, 51, 1024–1027. [Google Scholar] [CrossRef]
- Scholl, T.O. Maternal iron status: Relation to fetal growth, length of gestation, and iron endowment of the neonate. Nutr. Rev. 2011, 69, S23–S29. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, K.M. Is There a Causal Relationship between Iron Deficiency or Iron-Deficiency Anemia and Weight at Birth, Length of Gestation and Perinatal Mortality? J. Nutr. 2001, 131, 590S–603S. [Google Scholar] [CrossRef] [Green Version]
- Shao, J.; Lou, J.; Rao, R.; Georgieff, M.K.; Kaciroti, N.; Felt, B.T.; Zhao, Z.-Y.; Lozoff, B. Maternal Serum Ferritin Concentration Is Positively Associated with Newborn Iron Stores in Women with Low Ferritin Status in Late Pregnancy. J. Nutr. 2012, 142, 2004–2009. [Google Scholar] [CrossRef] [PubMed]
- Lozoff, B.; Beard, J.; Connor, J.; Felt, B.; Georgieff, M.; Schallert, T. Long-Lasting Neural and Behavioral Effects of Iron Deficiency in Infancy. Nutr. Rev. 2006, 64, S34–S43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Congdon, E.L.; Westerlund, A.; Algarin, C.R.; Peirano, P.D.; Gregas, M.; Lozoff, B.; Nelson, C.A. Iron Deficiency in Infancy is Associated with Altered Neural Correlates of Recognition Memory at 10 Years. J. Pediatr. 2012, 160, 1027–1033. [Google Scholar] [CrossRef] [Green Version]
- WHO. Serum Ferritin Concentrations for the Assessment of Iron Status in Individuals and Populations: Technical Brief; World Health Organization: Geneva, Switzerland, 2020; License: CC BY-NC-SA 3.0 IGO. [Google Scholar]
- WHO. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience; World Health Organization: Geneva, Switzerland, 2016; p. 41. [Google Scholar]
- Pavord, S.; Daru, J.; Prasannan, N.; Robinson, S.; Stanworth, S.; Girling, J.; on behalf of the BSH Committee. UK guidelines on the management of iron deficiency in pregnancy. Br. J. Haematol. 2020, 188, 819–830. [Google Scholar] [CrossRef] [Green Version]
- Lejniece, S. Anēmija grūtniecības laikā. In Medicīnas Apgāds; Rezeberga, D., Dzemdniecība, R., Eds.; SIA: Hyderabad, India, 2016; pp. 609–621. [Google Scholar]
- Bivolarska, A.; Gatseva, P.D.; Maneva, A.I. The Role of Eating Habits on the Iron Status of Pregnant Women. J. Am. Coll. Nutr. 2015, 35, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Peña-Rosas, J.P.; De-Regil, L.M.; Garcia-Casal, M.N.; Dowswell, T. Daily oral iron supplementation during pregnancy. Cochrane Database Syst. Rev. 2015, 12, CD004736. [Google Scholar] [CrossRef] [Green Version]
- Ng, S.-W.; Norwitz, S.G.; Norwitz, E.R. The Impact of Iron Overload and Ferroptosis on Reproductive Disorders in Humans: Implications for Preeclampsia. Int. J. Mol. Sci. 2019, 20, 3283. [Google Scholar] [CrossRef] [Green Version]
- Means, R.T. Iron deficiency and iron deficiency anemia: Implications and impact in pregnancy, fetal development, and early childhood parameters. Nutrients 2020, 12, 447. [Google Scholar] [CrossRef] [Green Version]
- Meija, L.; Rezeberga, D. Proper Maternal Nutrition during Pregnancy Planning and Pregnancy: A Healthy Start in Life, 2017. Available online: https://www.euro.who.int/__data/assets/pdf_file/0003/337566/Maternal-nutrition-Eng.pdf (accessed on 20 June 2021).
- WHO Data on Prevalence of Anaemia in Pregnant Women Aged 15–49 Years (%). Available online: https://www.who.int/data/maternal-newborn-child-adolescent-ageing/indicator-explorer-new/mca/prevalence-of-anaemia-in-pregnant-women-aged-15-49-years-(-) (accessed on 1 July 2021).
- Statistikas Dati—Slimību Profilakses un Kontroles Centrs, 2020. Available online: https://statistika.spkc.gov.lv/pxweb/lv/Health/Health__Mates_berna_veseliba/MCH080_Mates_slimibas_sarezgijumi.px/table/tableViewLayout2/ (accessed on 14 January 2020).
- Pudule, I.; Villeruša, A.; Grinberga, D.; Velika, B.; Tilgale, N.; Dzerve, V.; Zile, S.; Konttinen, H.; Prättälä, R. Health Behaviour among Latvian Adult Population, 2016. Available online: https://www.spkc.gov.lv/lv/media/4300/download (accessed on 15 June 2021).
- NHS. Have a Healthy Diet in Pregnancy. Available online: https://www.nhs.uk/pregnancy/keeping-well/have-a-healthy-diet/ (accessed on 20 June 2021).
- Veselīga Uztura Ieteikumi Sievietēm Grūtniecības Laikā, 2017. Available online: https://www.vm.gov.lv/lv/media/3719/download (accessed on 15 June 2021).
- Cabinet of Ministers, 2017, Nr. 60 “Grozījumi Ministru Kabineta 2006. Gada 25. Jūlija Noteikumos Nr. 611 “Dzemdību Palīdzības Nodrošināšanas Kārtība”. Available online: https://likumi.lv/ta/id/288450 (accessed on 15 June 2021).
- Bergmann, R.L.; Gravens-Müller, L.; Hertwig, K.; Hinkel, J.; Andres, B.; Bergmann, K.E.; Dudenhausen, J.W. Iron deficiency is prevalent in a sample of pregnant women at delivery in Germany. Eur. J. Obstet. Gynecol. Reprod. Biol. 2002, 102, 155–160. [Google Scholar] [CrossRef]
- Hess, S.Y.; Zimmermann, M.B.; Brogli, S.; Hurrell, R.F. A National Survey of Iron and Folate Status in Pregnant Women in Switzerland. Int. J. Vitam. Nutr. Res. 2001, 71, 268–273. [Google Scholar] [CrossRef]
- Harvey, T.; Zkik, A.; Auges, M.; Clavel, T. Assessment of Iron Deficiency and Anemia in Pregnant Women: An Observational French Study. Women’s Health 2016, 12, 95–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milman, N.; Taylor, C.L.; Merkel, J.; Brannon, P.M. Iron status in pregnant women and women of reproductive age in Europe. Am. J. Clin. Nutr. 2017, 106, 1655S–1662S. [Google Scholar] [CrossRef] [PubMed]
- Churchill, D.; Nair, M.; Stanworth, S.J.; Knight, M. The change in haemoglobin concentration between the first and third trimesters of pregnancy: A population study. BMC Pregnancy Childbirth 2019, 19, 359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milman, N.; Bergholt, T.; Byg, K.-E.; Eriksen, L.; Graudal, N. Iron status and iron balance during pregnancy. A critical reappraisal of iron supplementation. Acta Obstet. Et Gynecol. Scand. 1999, 78, 749–757. [Google Scholar] [CrossRef]
- Tendean, H.; Suparman, E.; Lumentut, A. Ferritin Level in Second and Third Trimester of Pregnancy. J. Food Health 2021, 1, 102–107. [Google Scholar]
- Stoffel, N.U.; Zimmermann, M.B.; Cepeda-Lopez, A.C.; Cervantes-Gracia, K.; Llanas-Cornejo, D.; Zeder, C.; Tuntipopipat, S.; Moungmaithong, S.; Densupsoontorn, N.; Loetscher, K.Q.; et al. Maternal iron kinetics and maternal–fetal iron transfer in normal-weight and overweight pregnancy. Am. J. Clin. Nutr. 2021, 115, 1166–1179. [Google Scholar] [CrossRef]
- Moustarah, F.; Mohiuddin, S.S. Dietary Iron; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Ems, T.; St Lucia, K.; Huecker, M.R. Biochemistry, Iron Absorption; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Michels, A.J.; Frei, B. Vitamin C. In Biochemical, Physiological, and Molecular Aspects of Human Nutrition; Stipanuk, M.H., Caudill, M.A., Eds.; Elsevier/Saunders: St. Louis, MO, USA, 2012; pp. 626–654. [Google Scholar] [CrossRef]
- Dasa, F.; Abera, T. Factors affecting iron absorption and mitigation mechanisms: A review. Int. J. Agric. Sci. Food Technol. 2018, 4, 024–030. [Google Scholar]


{kind=link}
| Indicators | Hb, g/L | SF, µg/L | ||||
|---|---|---|---|---|---|---|
| I Trimester (n = 783) | II Trimester (n = 731) | III Trimester (n = 788) | I Trimester (n = 743) | II Trimester (n = 407) | III Trimester (n = 617) | |
| Median | 127.0 | 117.0 | 115.0 | 31.8 | 16.1 | 11.3 |
| IQR (Q1 to Q3) | 121.0–132.0 | 111.0–122.0 | 109.0–121.0 | 17.6–53.1 | 10.0–27.4 | 7.8–17.6 |
| Range | 95.0 to 184.0 | 84.0 to 270.0 | 76.0 to 150.0 | 4.2 to 187 | 1.1 to 157.0 | 2.3 to 201 |
| UK Recommendations | ||||||
|---|---|---|---|---|---|---|
| Indicators | ID anaemia | ID | ||||
| I trimester (n = 783) | II trimester (n = 731) | III trimester (n = 788) | I trimester (n = 743) | II trimester (n = 407) | III trimester (n = 617) | |
| n | 22 | 58 | 96 | 347 | 318 | 566 |
| % | 2.8 | 7.9 | 12.2 | 46.7 | 78.1 | 91.7 |
| 95% CI | 1.9 to 4.2 | 6.2 to 10.1 | 10.1 to 14.7 | 43.1 to 50.3 | 73.9 to 81.9 | 89.3 to 93.7 |
| WHO | ||||||
| Indicators | ID anaemia | ID | ||||
| I trimester (n = 783) | II trimester (n = 731) | III trimester (n = 788) | I trimester (n = 743) | II trimester (n = 407) | III trimester (n = 617) | |
| n | 22 | 58 | 213 | 136 | 184 | 406 |
| % | 2.8 | 7.9 | 27.0 | 18.3 | 45.2 | 65.8 |
| 95% CI | 1.9 to 4.2 | 6.2 to 10.1 | 24.1 to 30.2 | 15.7 to 21.3 | 40.4 to 50.1 | 62.0 to 69.4 |
| Demographic Characteristics or BMI | I Trimester (n = 783) | II Trimester (n = 731) | III Trimester (n = 788) | |||
|---|---|---|---|---|---|---|
| Anaemic * | Non-Anaemic | Anaemic * | Non-Anaemic | Anaemic * | Non-Anaemic | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Total | 22 (2.8) | 762 (97.2) | 58 (7.9) | 674 (92.1) | 213 (27.0) | 576 (73.0) |
| Age group | ||||||
| <20 | 0 (0.0) | 10 (100.0) | 2 (20.0) | 8 (80.0) | 6 (54.5) | 5 (45.5) |
| 20–24 | 5 (3.4) | 144 (96.6) | 13 (9.8) | 120 (90.2) | 43 (38.7) | 107 (71.3) |
| 25–29 | 4 (2.1) | 186 (97.9) | 11 (6.2) | 166 (93.8) | 51 (25.8) | 146 (74.2) |
| 30–34 | 7 (2.5) | 268 (97.5) | 21 (7.8) | 248 (92.2) | 77 (28.3) | 195 (71.7) |
| ≥35 | 6 (3.8) | 153 (96.2) | 11 (7.7) | 131 (92.3) | 36 (22.8) | 122 (77.2) |
| BMI before pregnancy | ||||||
| <18.5 | 0 (0.0) | 32 (100.0) | 2 (6.3) | 29 (93.7) | 11 (32.4) | 22 (67.6) |
| 18.5–24.9 | 16 (3.4) | 459 (96.6) | 4 (9.6) | 397 (90.4) | 120 (25.5) | 351 (74.5) |
| 25.0–29.9 | 4 (2.2) | 180 (97.8) | 10 (6.1) | 154 (93.9) | 60 (33.5) | 119 (66.5) |
| ≥30.0 | 1 (1.6) | 62 (98.4) | 2 (3.1) | 63 (96.9) | 15 (19.7) | 61 (80.3) |
| No data ** | 27 (3.4) | 32 (4.4) | 29 (3.7) | |||
| Education | ||||||
| Primary or unfinished secondary | 3 (6.5) | 43 (93.5) | 4 (9.1) | 40 (90.9) | 15 (31.9) | 32 (68.1) |
| General secondary | 2 (2.0) | 97 (98.0) | 8 (8.3) | 88 (91.7) | 28 (27.5) | 74 (72.5) |
| Vocational secondary | 6 (3.8) | 154 (96.2) | 13 (8.7) | 137 (91.3) | 48 (31.6) | 104 (68.4) |
| Higher or unfinished higher | 11 (2.3) | 467 (97.7) | 33 (7.5) | 408 (92.5) | 122 (25.0) | 365 (75.0) |
| Marital status | ||||||
| Married | 8 (1.6) | 496 (98.4) | 33 (7.0) | 440 (93.0) | 122 (24.0) | 395 (76.0) |
| Living in partnership | 13 (6.2) | 197 (93.8) | 20 (10.2) | 176 (89.8) | 63 (30.7) | 142 (69.3) |
| Single | 0 (0.0) | 59 (100.0) | 4 (7.5) | 49 (92.5) | 24 (36.9) | 41 (63.1) |
| Divorced or live separately, widow | 1 (11.1) | 8 (88.9) | 1 (12.5) | 7 (87.5) | 3 (30.0) | 7 (70) |
| No data ** | 1 (0.1) | 1 (0.1) | 1 (0.1) | |||
| Nationality | ||||||
| Latvian | 17 (3.0) | 541 (97.0) | 38 (7.4) | 476 (92.6) | 151 (26.9) | 410 (73.1) |
| Russian | 4 (2.3) | 170 (97.7) | 12 (7.0) | 159 (93.0) | 41 (22.9) | 138 (77.1) |
| Other | 1 (2.0) | 50 (98.0) | 8 (17.4) | 38 (82.6) | 21 (43.8) | 27 (56.3) |
| Residence | ||||||
| Riga | 12 (3.5) | 327 (96.5) | 34 (10.5) | 291 (89.5) | 90 (26.7) | 247 (73.3) |
| Another city in Latvia | 7 (2.1) | 320 (97.9) | 15 (5.0) | 284 (95.0) | 88 (26.9) | 238 (73.1) |
| Village/rural area | 3 (2.6) | 112 (97.4) | 9 (8.6) | 96 (91.4) | 35 (28.5) | 88 (71.5) |
| No data ** | 2 (0.3) | 2 (0.3) | 2 (0.3) | |||
| Number of births | ||||||
| 1 | 10 (2.7) | 367 (97.3) | 27 (7.4) | 339 (92.6) | 110 (27.7) | 287 (72.3) |
| 2 | 8 (3.1) | 249 (96.9) | 18 (7.8) | 212 (92.2) | 62 (24.4) | 192 (75.6) |
| ≥3 | 4 (2.7) | 145 (97.3) | 13 (9.6) | 122 (90.4) | 41 (29.9) | 96 (70.1) |
| Demographic Characteristics or BMI | OR (95% CI) | B * | S.E. * | Wald * | Exp(B) * | 95% C.I.for EXP(B) * | p * |
|---|---|---|---|---|---|---|---|
| Marital status | |||||||
| Married | (Ref) | ||||||
| Living in partnership | 1.40 (0.98 to 2.01) | 0.308 | 0.190 | 2.628 | 1.36 | 0.94 to 1.98 | 0.105 |
| Single | 1.85 (1.07 to 3.18) | 0.626 | 0.287 | 4.746 | 1.87 | 1.07 to 3.29 | 0.029 |
| Divorced or live separately, widow | 1.35 (0.34 to 5.31) | 0.016 | 0.815 | 0.000 | 1.02 | 0.21 to 5.01 | 0.984 |
| Nationality | |||||||
| Latvian | (Ref) | ||||||
| Russian | 0.81 (0.54 to 1.20) | −0.142 | 0.211 | 0.455 | 0.87 | 0.57 to 1.31 | 0.500 |
| Other | 2.11 (1.16 to 3.85) | 0.737 | 0.314 | 5.497 | 2.09 | 1.13 to 3.87 | 0.019 |
| BMI before pregnancy | |||||||
| 18.5–24.9 | (Ref) | ||||||
| <18.5 | 1.46 (0.69 to 3.11) | 0.336 | 0.387 | 0.753 | 1.40 | 0.66 to 2.99 | 0.386 |
| 25.0–29.9 | 1.48 (1.02 to 2.14) | 0.381 | 0.194 | 3.881 | 1.46 | 1.00 to 2.14 | 0.049 |
| >30 | 0.72 (0.39 to 1.31) | −0.283 | 0.310 | 0.833 | 0.75 | 0.411 to 1.38 | 0.362 |
| All n (%) | Anaemic n (%) | Non-Anaemic n (%) | p | |
|---|---|---|---|---|
| Meat (at least 3 portions a week) | ||||
| 0 portions | 20 (2.5) | 7 (35.0) | 13 (65.0) | 0.551 |
| <3 portions | 97 (12.3) | 29 (29.9) | 69 (70.1) | |
| 3+ portions | 671 (85.2) | 177 (26.4) | 494 (73.6) | |
| Fish (at least 3 portions a week) * | ||||
| 0 portions | 125 (15.9) | 38 (30.4) | 87 (69.6) | 0.326 |
| <2 portions | 540 (68.6) | 148 (27.4) | 392 (72.6) | |
| 2+ portions | 122 (15.5) | 27 (22.1) | 95 (77.9) | |
| Dairy products (3–4 times a day) ** | ||||
| 0 portions | 8 (1.0) | 3 (37.5) | 5 (62.5) | 0.292 |
| <3 portions | 494 (62.9) | 143 (28.9) | 351 (71.1) | |
| 3 to 4 portions | 160 (20.4) | 35 (21.9) | 125 (78.1) | |
| >4 portion | 123 (15.7) | 31 (25.2) | 92 (74.8) | |
| Vegetables (at least 3 portions a day) | ||||
| <3 portions | 778 (98.7) | 212 (27.2) | 566 (72.8) | 0.302 |
| 3+ portions | 10 (1.3) | 1 (10.0) | 9 (90.0) | |
| Fruits (at least 2 portions a day) | ||||
| <2 portions | 686 (87.1) | 182 (26.5) | 504 (73.5) | 0.413 |
| 2+ portions | 103 (12.9) | 31 (30.4) | 71 (69.6) | |
| Coffee (every day) * | ||||
| Never | 140 (17.8) | 44 (31.4) | 96 (68.6) | 0.339 |
| Sometimes | 233 (29.6) | 64 (27.5) | 169 (72.5) | |
| Every day | 414 (52.6) | 104 (25.1) | 310 (74.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rezgale, R.; Pudule, I.; Cauce, V.; Klaramunta Antila, K.; Bule, V.; Lazdane, G.; Rezeberga, D.; Meija, L. Iron Status in Pregnant Women in Latvia: An Epidemiological, Cross-Sectional, Multicenter Study According to WHO and UK Criteria. Medicina 2022, 58, 955. https://doi.org/10.3390/medicina58070955
Rezgale R, Pudule I, Cauce V, Klaramunta Antila K, Bule V, Lazdane G, Rezeberga D, Meija L. Iron Status in Pregnant Women in Latvia: An Epidemiological, Cross-Sectional, Multicenter Study According to WHO and UK Criteria. Medicina. 2022; 58(7):955. https://doi.org/10.3390/medicina58070955
Chicago/Turabian StyleRezgale, Roberta, Iveta Pudule, Vinita Cauce, Kristine Klaramunta Antila, Violeta Bule, Gunta Lazdane, Dace Rezeberga, and Laila Meija. 2022. "Iron Status in Pregnant Women in Latvia: An Epidemiological, Cross-Sectional, Multicenter Study According to WHO and UK Criteria" Medicina 58, no. 7: 955. https://doi.org/10.3390/medicina58070955