
Systematic Review of Patient-Reported Outcome Measures for Patients with Exercise-Induced Leg Pain

 ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
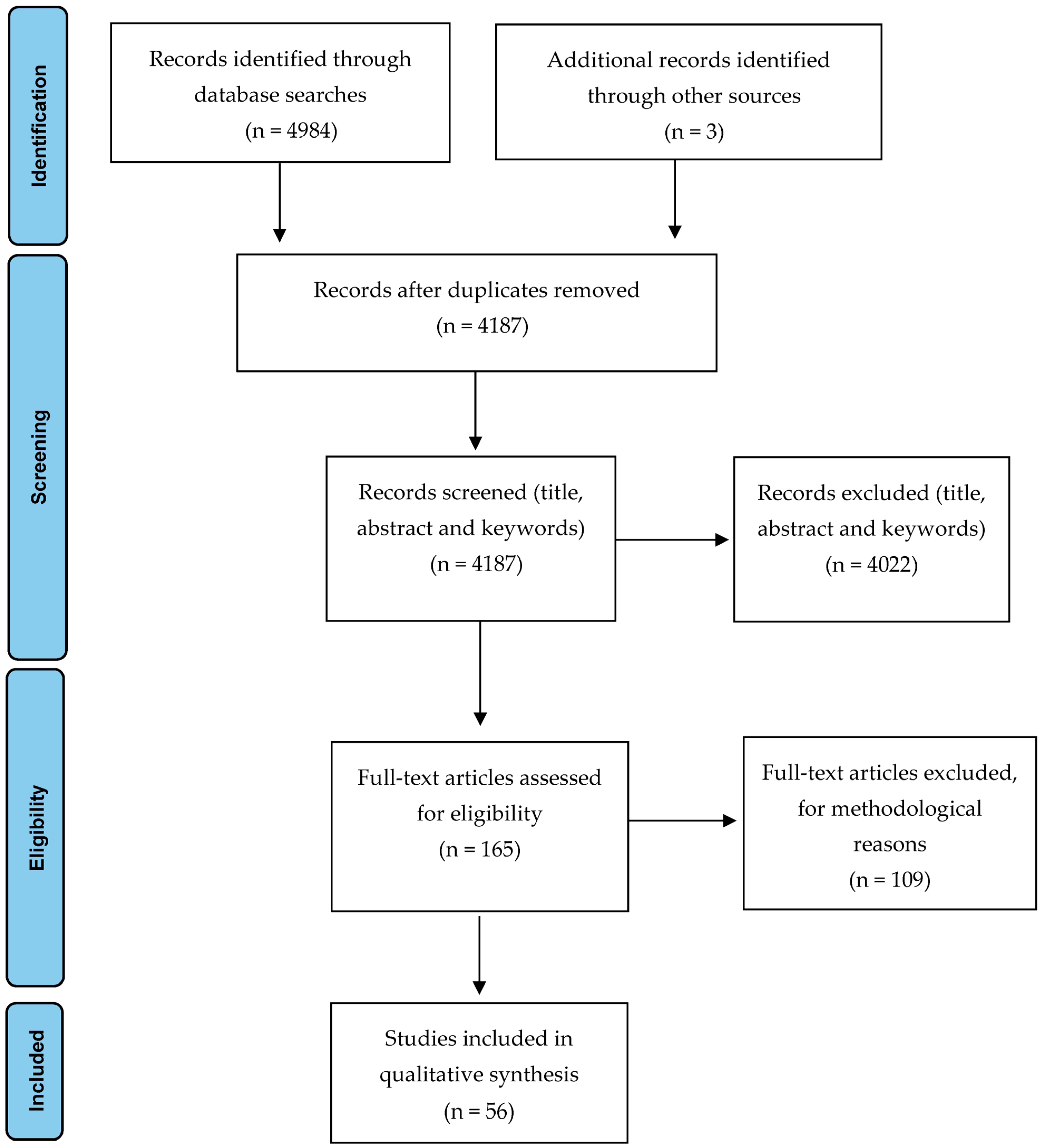
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Data Synthesis and Analysis
3. Results
3.1. Specific Patient-Reported Outcome Measures for Exercise-Induced Leg Pain
3.2. Psychometric Properties
3.2.1. Content Validity
3.2.2. Internal Consistency
3.2.3. Criterion Validity
3.2.4. Construct Validity
3.2.5. Reproducibility Agreement
3.2.6. Reproducibility Reliability
3.2.7. Responsiveness
3.2.8. Ceiling and Floor Effects
3.2.9. Interpretability
3.2.10. Cross-Cultural Adaptation
3.3. Methodological Quality
3.3.1. Structural Validity
3.3.2. Internal Consistency
3.3.3. Reliability
3.3.4. Measurement Error
3.3.5. Hypothesis Testing for Construct Validity
3.3.6. Cross-Cultural Validity/Measurement Invariance
3.3.7. Criterion Validity
3.3.8. Responsiveness
3.4. Methodological Quality Scores for Measurement Properties in Each Study
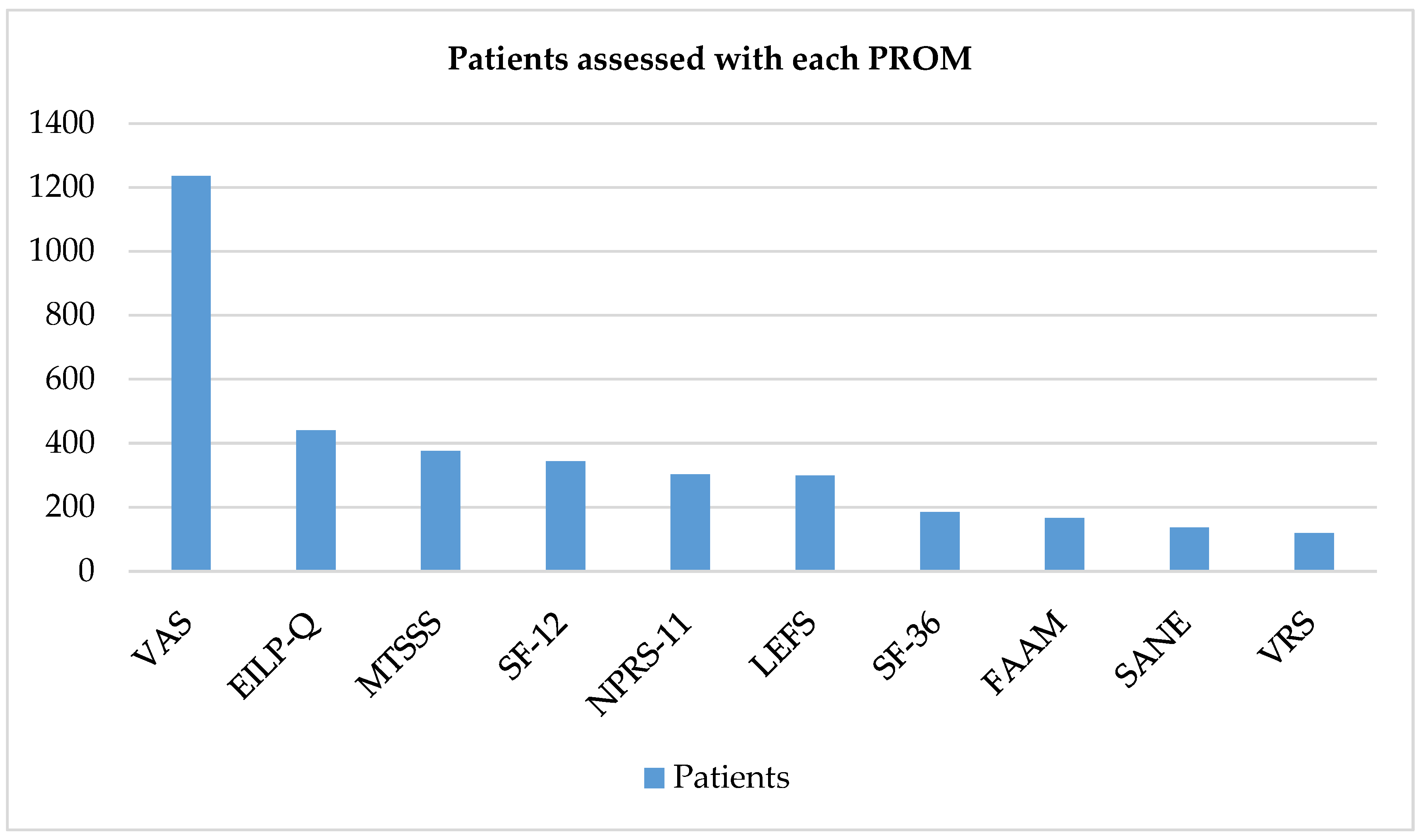
3.5. Frequency of Patient-Reported Outcome Measure Use in Exercise-Induced Leg Pain
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategy
References
- Lohrer, H.; Malliaropoulos, N.; Korakakis, V.; Padhiar, N. Exercise-induced leg pain in athletes: Diagnostic, assessment, and management strategies. Physician Sportsmed. 2018, 47, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Barnes, K.R.; Kilding, A.E. Running economy: Measurement, norms, and determining factors. Sports Med. Open 2015, 1, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, P.H.; Wright, M.L.; Hartman, J.F. A practical approach for the differential diagnosis of chronic leg pain in the athlete. Am. J. Sports Med. 2005, 33, 1241–1249. [Google Scholar] [CrossRef] [PubMed]
- Fortina, M.; Maniscalco, P.; Carulli, C.; Meccariello, L.; Colasanti, G.B.; Carta, S. Jockey injuries during the Siena “Palio”. A 72-year analysis of the oldest horse race in Italy. Injury 2018, 50, 365–368. [Google Scholar] [CrossRef]
- Orava, S.; Puranen, J. Athletes’ leg pains. Br. J. Sports Med. 1979, 13, 92–97. [Google Scholar] [CrossRef]
- Lopes, A.D.; Hespanhol, L.C.; Yeung, S.S.; Costa, L.O.P. What are the Main Running-Related Musculoskeletal Injuries? Sports Med. 2012, 42, 891–905. [Google Scholar] [CrossRef]
- Reinking, M.F. Exercise Related Leg Pain (ERLP): A Review of The Literature. N. Am. J. Sports Phys. Ther. 2007, 2, 170–180. [Google Scholar] [PubMed]
- Styf, J. Diagnosis of exercise-induced pain in the anterior aspect of the lower leg. Am. J. Sports Med. 1988, 16, 165–169. [Google Scholar] [CrossRef]
- Clanton, T.; Solcher, B. Chronic leg pain in the athlete. Clin. Sports Med. 1994, 13, 743–759. [Google Scholar] [CrossRef]
- Rajasekaran, S.; Kvinlaug, K.; Finnoff, J.T. Exertional Leg Pain in the Athlete. PM&R 2012, 4, 985–1000. [Google Scholar] [CrossRef]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; De Vet, H.C.W. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: An international Delphi study. Qual. Life Res. 2010, 19, 539–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castillo-Domínguez, A.; García-Romero, J.C.; Páez-Moguer, J.; Ponce-García, T.; Medina-Alcántara, M.; Alvero-Cruz, J.R. Relationship between Running Spatiotemporal Kinematics and Muscle Performance in Well-Trained Youth Female Athletes. A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 8869. [Google Scholar] [CrossRef] [PubMed]
- Winters, M.; Moen, M.H.; Zimmermann, W.O.; Lindeboom, R.; Weir, A.; Backx, F.J.; Bakker, E.W. The medial tibial stress syndrome score: A new patient-reported outcome measure. Br. J. Sports Med. 2015, 50, 1192–1199. [Google Scholar] [CrossRef] [PubMed]
- Binkley, J.M.; Stratford, P.W.; Lott, S.A.; Riddle, D.L. The Lower Extremity Functional Scale (LEFS): Scale development, measurement properties, and clinical application. Phys. Ther. 1999, 79, 371–383. [Google Scholar] [CrossRef]
- Nauck, T.; Lohrer, H.; Padhiar, N.; King, J.B. Development and validation of a questionnaire to measure the severity of functional limitations and reduction of sports ability in German-speaking patients with exercise-induced leg pain. Br. J. Sports Med. 2012, 49, 113–117. [Google Scholar] [CrossRef] [Green Version]
- Martin, R.R.L.; Irrgang, J.J.; Burdett, R.G.; Conti, S.F.; Van Swearingen, J.M. Evidence of validity for the Foot and Ankle Ability Measure (FAAM). Foot Ankle Int. 2005, 26, 968–983. [Google Scholar] [CrossRef]
- Koldenhoven, R.M.; Virostek, A.; DeJong, A.F.; Higgins, M.; Hertel, J. Increased Contact Time and Strength Deficits in Runners With Exercise-Related Lower Leg Pain. J. Athl. Train. 2020, 55, 1247–1254. [Google Scholar] [CrossRef]
- Bellamy, J.T.; Boissonneault, A.R.; Melquist, M.E.; Labib, S.A. Release of the Tibialis Posterior Muscle Osseofascial Sheath Improves Results of Deep Exertional Compartment Syndrome Surgery: A Comparative Analysis and Long-term Results. Orthop. J. Sports Med. 2020, 8, 2325967120942752. [Google Scholar] [CrossRef]
- Fredette, M.A.; Roy, J.-S.; Esculier, J.-F.; Perreault, K. Most Military Runners Report Recent Changes in Running Parameters Before Lower Limb Injury Onset. Mil. Med. 2020, 186, e1140–e1148. [Google Scholar] [CrossRef]
- McCall, C.E.; Koenig, R.C.; Winkelmann, Z.K.; Games, K.E. The Effects of Deep Oscillation Therapy for Individuals with The Effects of Deep Oscillation Therapy for Individuals with Lower-Leg Pain. J. Sports Med. Allied Health Sci. 2019, 4, 3. [Google Scholar]
- Nguyen, A.; Beasley, I.; Calder, J. Stress fractures of the medial malleolus in the professional soccer player demonstrate excellent outcomes when treated with open reduction internal fixation and arthroscopic spur debridement. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 2884–2889. [Google Scholar] [CrossRef] [PubMed]
- Naderi, A.; Degens, H.; Sakinepoor, A. Arch-support foot-orthoses normalize dynamic in-shoe foot pressure distribution in medial tibial stress syndrome. Eur. J. Sport Sci. 2018, 19, 247–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tam, J.P.H.; Gibson, A.G.F.; Murray, J.R.D.; Hassaballa, M. Fasciotomy for chronic exertional compartment syndrome of the leg: Clinical outcome in a large retrospective cohort. Eur. J. Orthop. Surg. Traumatol. 2018, 29, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N.; Loppini, M.; Spiezia, F.; D’Addona, A.; Maffulli, G.D. Single minimal incision fasciotomy for chronic exertional compartment syndrome of the lower leg. J. Orthop. Surg. Res. 2016, 11, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thein, R.; Tilbor, I.; Rom, E.; Herman, A.; Haviv, B.; Burstein, G.; Tenenbaum, S. Return to sports after chronic anterior exertional compartment syndrome of the leg: Conservative treatment versus surgery. J. Orthop. Surg. 2019, 27, 2309499019835651. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, J.; Isu, T.; Kim, K.; Iwamoto, N.; Yamazaki, K.; Isobe, M. Clinical features and surgical treatment of superficial peroneal nerve entrapment neuropathy. Neurol. Med. Chir. 2018, 58, 320–325. [Google Scholar] [CrossRef] [Green Version]
- Meulekamp, M.Z.; Sauter, W.; Buitenhuis, M.; Mert, A.; van Der Wurff, P. Short-term results of a rehabilitation program for service members with lower leg pain and the evaluation of patient characteristics. Mil. Med. 2016, 181, 1081–1087. [Google Scholar] [CrossRef] [Green Version]
- Farrugia, P.; Goldstein, C.; Petrisor, B.A. Measuring foot and ankle injury outcomes: Common scales and checklists. Injury 2011, 42, 276–280. [Google Scholar] [CrossRef]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Valderas, J.M.; Ferrer, M.; Alonso, J. Instrumentos de medida de calidad de vida relacionada con la salud y de otros resultados percibidos por los pacientes. Med. Clin. 2005, 125, 56–60. [Google Scholar] [CrossRef]
- Sánchez, R.; Echeverry, J. Validación de escalas de medición en salud. Rev. Salud Pública 2004, 6, 302–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Streiner, D.; Norman, G. Health Measurement Scales: A Practical Guide to their Development and Use, 2nd ed.; Oxford University Press: New York, NY, USA, 1995. [Google Scholar]
- Fava, G.A.; Tomba, E.; Sonino, N. Clinimetrics: The science of clinical measurements. Int. J. Clin. Pract. 2012, 66, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Feinstein, A.R.T. Duckett Jones Memorial Lecture. The Jones criteria and the challenges of clinimetrics. Circulation 1982, 66, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez Pedraza, R.; Gómez Restrepo, C. Conceptos básicos sobre validación de escalas. Rev. Colomb. Psiquiatr. 1998, XXVII, 121–130. [Google Scholar]
- Cronbach, L.J.; Meehl, P.E. Construct Validity in Psychological Tests; Pergamon Press Ltd.: Oxford, UK, 1966. [Google Scholar]
- Beaudart, C.; Hagelstein, T.; Van Beveren, J.; Godon, B.; Bruyère, O.; Kaux, J.F. French translation and validation of the exercise-induced leg pain Questionnaire. Disabil. Rehabil. 2018, 42, 857–862. [Google Scholar] [CrossRef]
- de Vet, H.C.; Terwee, C.B.; Ostelo, R.W.; Beckerman, H.; Knol, D.L.; Bouter, L.M. Minimal changes in health status questionnaires: Distinction between minimally detectable change and minimally important change. Health Qual. Life Outcomes 2006, 4, 54. [Google Scholar] [CrossRef] [Green Version]
- Roberts, A.; Franklyn-Miller, A. The validity of the diagnostic criteria used in chronic exertional compartment syndrome: A systematic review. Scand. J. Med. Sci. Sports 2012, 22, 585–595. [Google Scholar] [CrossRef]
- Winters, M.; Eskes, M.; Weir, A.; Moen, M.H.; Backx, F.J.G.; Bakker, E.W.P. Treatment of medial tibial stress syndrome: A systematic review. Sports Med. 2013, 43, 1315–1333. [Google Scholar] [CrossRef]
- Maher, J.M.; Brook, E.M.; Chiodo, C.; Smith, J.; Bluman, E.M.; Matzkin, E.G. Patient-Reported Outcomes Following Fasciotomy for Chronic Exertional Compartment Syndrome. Foot Ankle Spec. 2018, 11, 471–477. [Google Scholar] [CrossRef]
- Wright, A.A.; Taylor, J.B.; Ford, K.R.; Siska, L.; Smoliga, J.M. Risk factors associated with lower extremity stress fractures in runners: A systematic review with meta-analysis. Br. J. Sports Med. 2015, 49, 1517–1523. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 88, 105906. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terwee, C.B.; Jansma, E.P.; Riphagen, I.I.; De Vet, H.C.W. Development of a methodological PubMed search filter for finding studies on measurement properties of measurement instruments. Qual. Life Res. 2009, 18, 1115–1123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prinsen, C.A.C.; Mokkink, L.B.; Bouter, L.M.; Alonso, J.; Patrick, D.L.; de Vet, H.C.W.; Terwee, C.B. COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual. Life Res. 2018, 27, 1147–1157. [Google Scholar] [CrossRef] [Green Version]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Terwee, C.B.; Mokkink, L.B.; Knol, D.L.; Ostelo, R.W.J.G.; Bouter, L.M.; De Vet, H.C.W. Rating the methodological quality in systematic reviews of studies on measurement properties: A scoring system for the COSMIN checklist. Qual. Life Res. 2011, 21, 651–657. [Google Scholar] [CrossRef] [Green Version]
- Schepsis, A.A.; Martini, D.; Corbett, M. Surgical management of Exertional Compartment Syndrome of the Lower Leg. Long-term followup. Am. J. Sports Med. 1993, 21, 811–817. [Google Scholar] [CrossRef]
- Shazadeh Safavi, P.; Janney, C.; Jupiter, D.; Kunzler, D.; Bui, R.; Panchbhavi, V.K. A Systematic Review of the Outcome Evaluation Tools for the Foot and Ankle. Foot Ankle Spec. 2018, 12, 461–470. [Google Scholar] [CrossRef]
- Price, D.D.; McGrath, P.A.; Rafii, A.; Buckingham, B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain 1983, 17, 45–56. [Google Scholar] [CrossRef]
- De Nies, F.; Fidler, M.W. Visual analog scale for the assessment of total hip arthroplasty. J. Arthroplast. 1997, 12, 416–419. [Google Scholar] [CrossRef]
- Mangan, J.J.; Rogero, R.; Fuchs, D.J.; Raikin, S.M. Surgical Management of Chronic Exertional Compartment Syndrome of the Lower Extremity: Outcome Analysis and Return to Sport. Foot Ankle Orthop. 2019, 4, 2473011419S0005. [Google Scholar] [CrossRef]
- Lee, J.S.; Hobden, E.; Stiell, I.G.; Wells, G.A. Clinically important change in the visual analog scale after adequate pain control. Acad. Emerg. Med. 2003, 10, 1128–1130. [Google Scholar] [CrossRef]
- Beaton, D.E.; Boers, M.; Wells, G.A. Many faces of the minimal clinically important difference (MICD): A literature review and directions for future research. Curr. Opin. Rheumatol. 2002, 14, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Pua, Y.H.; Cowan, S.M.; Wrigley, T.V.; Bennell, K.L. The Lower Extremity Functional Scale could be an alternative to the Western Ontario and McMaster Universities Osteoarthritis Index physical function scale. J. Clin. Epidemiol. 2009, 62, 1103–1111. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-W.C.; Moseley, A.M.; Refshauge, K.M.; Bundy, A.C. The Lower Extremity Functional Scale Has Good Clinimetric Properties in People With Ankle Fracture. Phys. Ther. 2009, 89, 580–588. [Google Scholar] [CrossRef] [PubMed]
- Reid, A.; Birmingham, T.B.; Stratford, P.W.; Alcock, G.K.; Giffin, J.R. Hop Testing Provides a Reliable and Valid Outcome Measure During Rehabilitation After Anterior Cruciate Ligament Reconstruction. Phys. Ther. 2007, 87, 337–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moen, M.H.; Bongers, T.; Bakker, E.W.; Zimmermann, W.O.; Weir, A.; Tol, J.L.; Backx, F.J.G. Risk factors and prognostic indicators for medial tibial stress syndrome. Scand. J. Med. Sci. Sports 2010, 22, 34–39. [Google Scholar] [CrossRef]
- Moen, M.H.; Schmikli, S.L.; Weir, A.; Steeneken, V.; Stapper, G.; de Slegte, R.; Tol, J.L.; Backx, F.J.G. A prospective study on MRI findings and prognostic factors in athletes with MTSS. Scand. J. Med. Sci. Sports 2014, 24, 204–210. [Google Scholar] [CrossRef]
- Cacchio, A.; De Blasis, E.; Necozione, S.; Rosa, F.; Riddle, D.L.; di Orio, F.; De Blasis, D.; Santilli, V. The Italian version of the Lower Extremity Functional Scale was reliable, valid, and responsive. J. Clin. Epidemiol. 2010, 63, 550–557. [Google Scholar] [CrossRef]
- René, F.; Casimiro, L.; Tremblay, M.; Brosseau, L.; Lefebvre, A.; Beaudouin, M.; Belliveau, V.; Bergeron, L.P. Une version canadienne française du Lower Extremity Functional Scale (LEFS): L’Échelle fonctionnelle des membres infÉrieurs (ÉFMI), partie I. Physiother. Can. 2011, 63, 242–248. [Google Scholar] [CrossRef] [Green Version]
- Hoogeboom, T.J.; De Bie, R.A.; Den Broeder, A.A.; Van Den Ende, C.H.M. The Dutch Lower Extremity Functional Scale was highly reliable, valid and responsive in individuals with hip/knee osteoarthritis: A validation study. BMC Musculoskelet. Disord. 2012, 13, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Díaz, D.; Lomas-Vega, R.; Osuna-Pérez, M.C.; Hita-Contreras, F.; Fernández, Á.D.; Martínez-Amat, A. The Spanish lower extremity functional scale: A reliable, valid and responsive questionnaire to assess musculoskeletal disorders in the lower extremity. Disabil. Rehabil. 2014, 36, 2005–2011. [Google Scholar] [CrossRef] [PubMed]
- Stasi, S.; Papathanasiou, G.; Anagnostou, M.; Galanos, A.; Chronopoulos, E.; Baltopoulos, P.I.; Papaioannou, N.A. Lower Extremity Functional scale (LEFS): Cross-cultural adaption into Greek and reliability properties of the instrument. Health Sci. J. 2012, 6, 750–773. [Google Scholar]
- Metsavaht, L.; Leporace, G.; Riberto, M.; Sposito, M.M.M.; Del Castillo, L.N.C.; Oliveira, L.P.; Batista, L.A. Translation and cross-cultural adaptation of the Lower Extremity Functional Scale into a Brazilian Portuguese version and validation on patients with knee injuries. J. Orthop. Sports Phys. Ther. 2012, 42, 932–939. [Google Scholar] [CrossRef] [PubMed]
- Alnahdi, A.H.; Alrashid, G.I.; Alkhaldi, H.A.; Aldali, A.Z. Cross-cultural adaptation, validity and reliability of the Arabic version of the Lower Extremity Functional Scale. Disabil. Rehabil. 2015, 38, 897–904. [Google Scholar] [CrossRef]
- Zhang, C.; Liu, Y.; Yuan, S.; Yang, T.; Gao, Y.; Zhu, C.; Ding, Z. Cross-Cultural Adaptation and Validation of the Simplified Chinese Version of the Lower Extremity Functional Scale. BioMed Res. Int. 2020, 2020, 1421429. [Google Scholar] [CrossRef] [Green Version]
- Negahban, H.; Hessam, M.; Tabatabaei, S.; Salehi, R.; Sohani, S.M.; Mehravar, M. Reliability and validity of the Persian lower extremity functional scale (LEFS) in a heterogeneous sample of outpatients with lower limb musculoskeletal disorders. Disabil. Rehabil. 2013, 36, 10–15. [Google Scholar] [CrossRef]
- Mohd Yunus, M.A.; Musa, R.; Nazri, M.Y. Construct and criterion validity of the Malaysia version of Lower Extremity Functional Scale (LEFS). Asia-Pac. J. Sports Med. Arthrosc. Rehabil. Technol. 2017, 10, 8–11. [Google Scholar] [CrossRef]
- Paravlic, A.H.; Pisot, S.; Mitic, P.; Pisot, R. Validation of the Oxford Knee Score and Lower Extremity Functional Score questionnaires for use in Slovenia. Arch. Orthop. Trauma Surg. 2020, 140, 1515–1522. [Google Scholar] [CrossRef]
- Repo, J.P.; Tukiainen, E.J.; Roine, R.P.; Ilves, O.; Järvenpää, S.; Häkkinen, A. Reliability and validity of the Finnish version of the Lower Extremity Functional Scale (LEFS). Disabil. Rehabil. 2017, 39, 1228–1234. [Google Scholar] [CrossRef]
- Korakakis, V.; Malliaropoulos, N.; Baliotis, K.; Papadopoulou, S.; Padhiar, N.; Nauck, T.; Lohrer, H. Cross-cultural adaptation and validation of the exercise-induced leg pain questionnaire for English-and Greek-speaking individuals. J. Orthop. Sports Phys. Ther. 2015, 45, 485–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castillo-Domínguez, A.; Alvero-Cruz, J.R.; Páez-Moguer, J.; Nauck, T.; Lohrer, H.; Scheer, V.; García-Romero, J. Cross-Cultural adaptation and validation of the Exercise-Induced Leg Pain questionnaire for Spanish speaking patients. Clin. Rehabil. 2022, 36, 968–979. [Google Scholar] [CrossRef] [PubMed]
- McKenna, S.P.; Heaney, A. Setting and maintaining standards for patient-reported outcome measures: Can we rely on the COSMIN checklists? J. Med. Econ. 2021, 24, 502–511. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Acronym | Full Title | Number of Items | Dimensions (Items) | Score Range | Interpretation of Score | Type of Population It Validates |
|---|---|---|---|---|---|---|
| VAS | Visual Analog Scale | 20 | Pain (4), function (11) and others (5) | 0–100 mm | Longer distance indicates poorer outcome | Generic. Not specific to a disease or region |
| MTSSS | Medial Tibial Stress Syndrome Score | 4 | Severity of medial tibial stress syndrome (4) | 0–10 points | Lower score indicates better outcome | Medial tibial stress syndrome |
| EILP-Q | Exercise-Induced Leg Pain Questionnaire | 10 | Physical function and athletic ability (10) | 0–40 points | Higher score indicates better outcome | Patients with exercise-induced leg pain |
| NPRS | Numerical Rating Scale-11 | 11 | Pain (11) | 0–10 points | Higher score indicates greater pain intensity | Patients with rheumatic pain and other chronic conditions (pain > 6 months) |
| LEFS | Lower Extremity Functional Scale | 20 | Physical function (20) | 0–80 points | Higher score indicates better outcome | Adults with lower extremity dysfunction |
| FAAM | Foot and Ankle Ability Measure | 29 | Activities of daily living (21) and physical function (8) | 0%–100% | Higher percentage indicates better outcome | Chronic ankle instability |
| SANE | Single Assessment Numeric Evaluation | 1 | Overall function rating | 0–100 points | Higher score indicates better outcome | Patients with foot and ankle pathology |
| SF-12 | Short Form-12 | 12 | Physical component (12) and mental component (12) | 0–100 points for each component | Higher score indicates better outcome | Generic. Not specific to a disease or region |
| SF-36 | Short Form-36 | 36 | Physical function (10), physical role (4), bodily pain (2), general health (5), vitality (4), social function (2), emotional role (3), mental health (5) and health changes (1) | 0–100 each component (physical and mental) | Higher score indicates better outcome | Generic. Not specific to a disease or region |
| VRS-7 | Verbal Rating Scale | 7 | Pain (7) | 1–7 points | Higher score indicates poorer outcome | Generic. Not specific to a disease or region |
| Content Validity | Internal Consistency | Criterion Validity | Construct Validity | Reproducibility Agreement | Reproducibility Reliability | Responsiveness | Floor and Ceiling Effects | Interpretability | |
|---|---|---|---|---|---|---|---|---|---|
| MTSSS | + | − | − | + | + | + | − | + | ? |
| EILP-Q | + | + | ? | − | 0 | + | 0 | 0 | 0 |
| LEFS | + | − | 0 | + | + | + | ? | + | ? |
| Structural Validity | Internal Consistency | Reliability | Measurement Error | Hypothesis Testing for Construct Validity | Cross-Cultural Validity | Criterion Validity | Responsiveness | |
|---|---|---|---|---|---|---|---|---|
| MTSSS | − | − | + | + | + | ? | ? | + |
| EILP-Q | − | + | + | ? | ? | + | ? | ? |
| LEFS | − | + | + | + | + | + | ? | + |
| BOX A Internal Consistency | BOX B Reliability | BOX C Measurement Error | BOX D Content Validity | BOX E Structural Validity | BOX F Hypothesis Testing | BOX G Cross-Cultural Validity | BOX H Criterion Validity | BOX I Responsiveness | |
|---|---|---|---|---|---|---|---|---|---|
| MTSSS | GOOD | POOR | POOR | EXCELLENT | EXCELLENT | GOOD | POOR | GOOD | |
| EILP-Q | POOR | POOR | FAIR | EXCELLENT | POOR | POOR | POOR | POOR | |
| LEFS | FAIR | POOR | FAIR | EXCELLENT | POOR | FAIR | POOR | FAIR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castillo-Domínguez, A.; García-Romero, J.C.; Alvero-Cruz, J.R.; Ponce-García, T.; Benítez-Porres, J.; Páez-Moguer, J. Systematic Review of Patient-Reported Outcome Measures for Patients with Exercise-Induced Leg Pain. Medicina 2022, 58, 841. https://doi.org/10.3390/medicina58070841
Castillo-Domínguez A, García-Romero JC, Alvero-Cruz JR, Ponce-García T, Benítez-Porres J, Páez-Moguer J. Systematic Review of Patient-Reported Outcome Measures for Patients with Exercise-Induced Leg Pain. Medicina. 2022; 58(7):841. https://doi.org/10.3390/medicina58070841
Chicago/Turabian StyleCastillo-Domínguez, Alejandro, Jerónimo C. García-Romero, José Ramón Alvero-Cruz, Tomás Ponce-García, Javier Benítez-Porres, and Joaquín Páez-Moguer. 2022. "Systematic Review of Patient-Reported Outcome Measures for Patients with Exercise-Induced Leg Pain" Medicina 58, no. 7: 841. https://doi.org/10.3390/medicina58070841