
Apocrine Hidrocystoma with IgG4 Plasma Cell Infiltration Presenting as Recurrent Chalazion: A Case Report

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
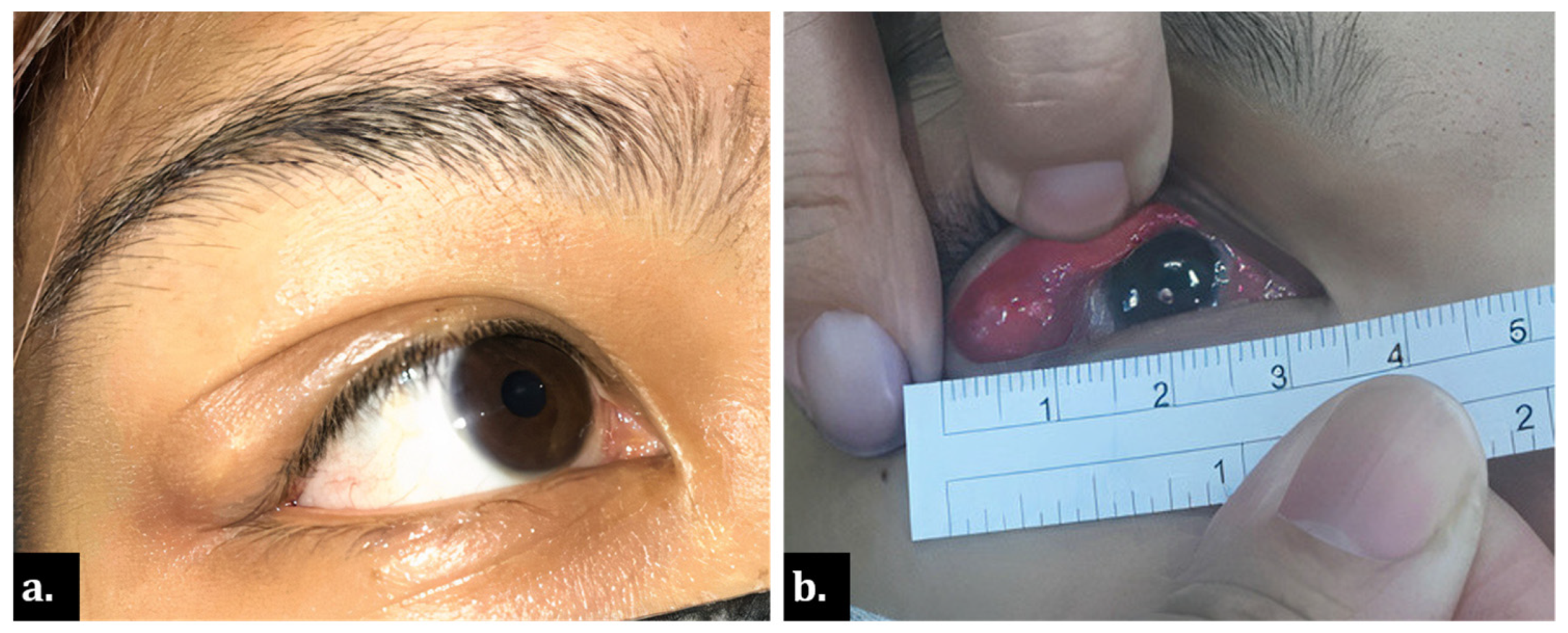
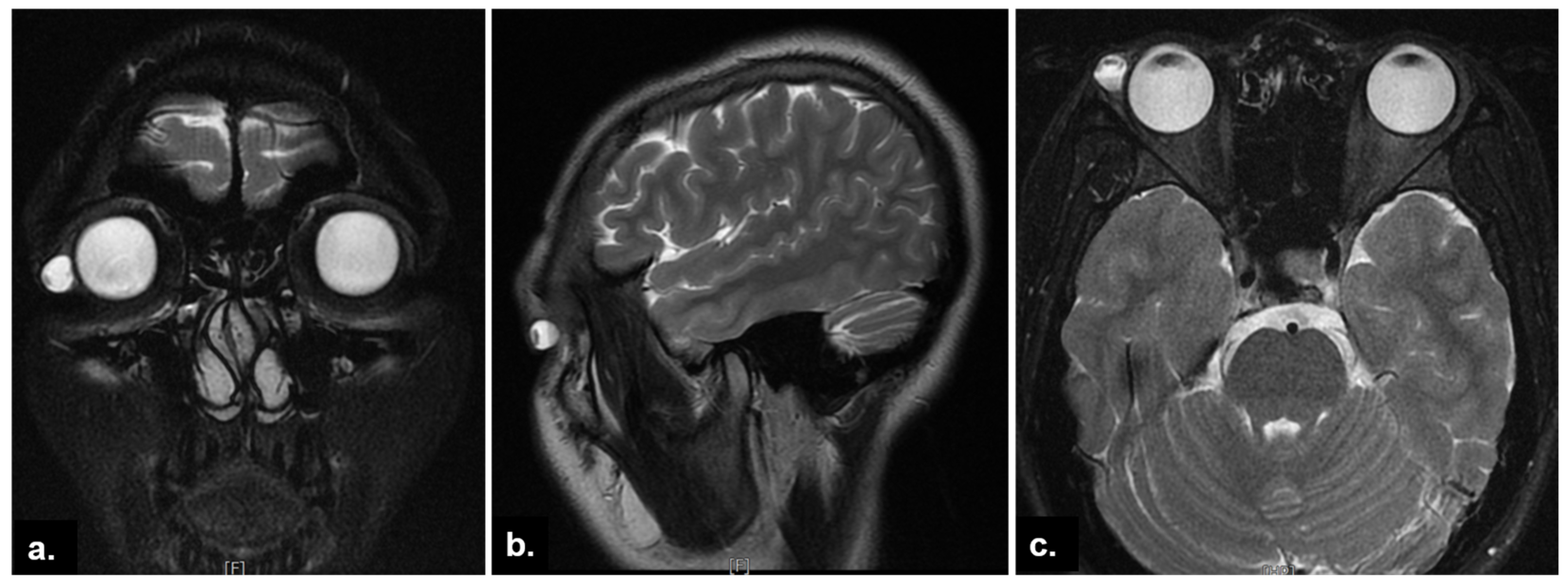
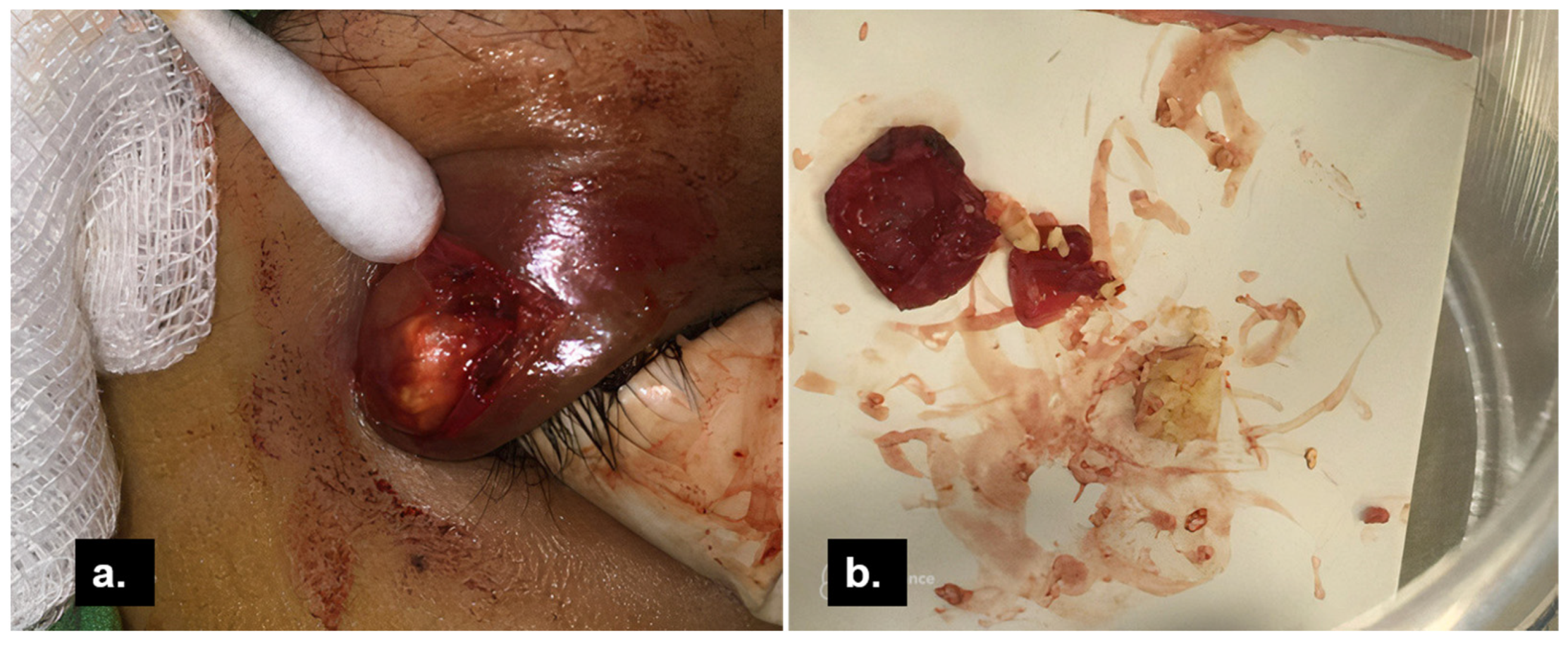
2. Case Presentation
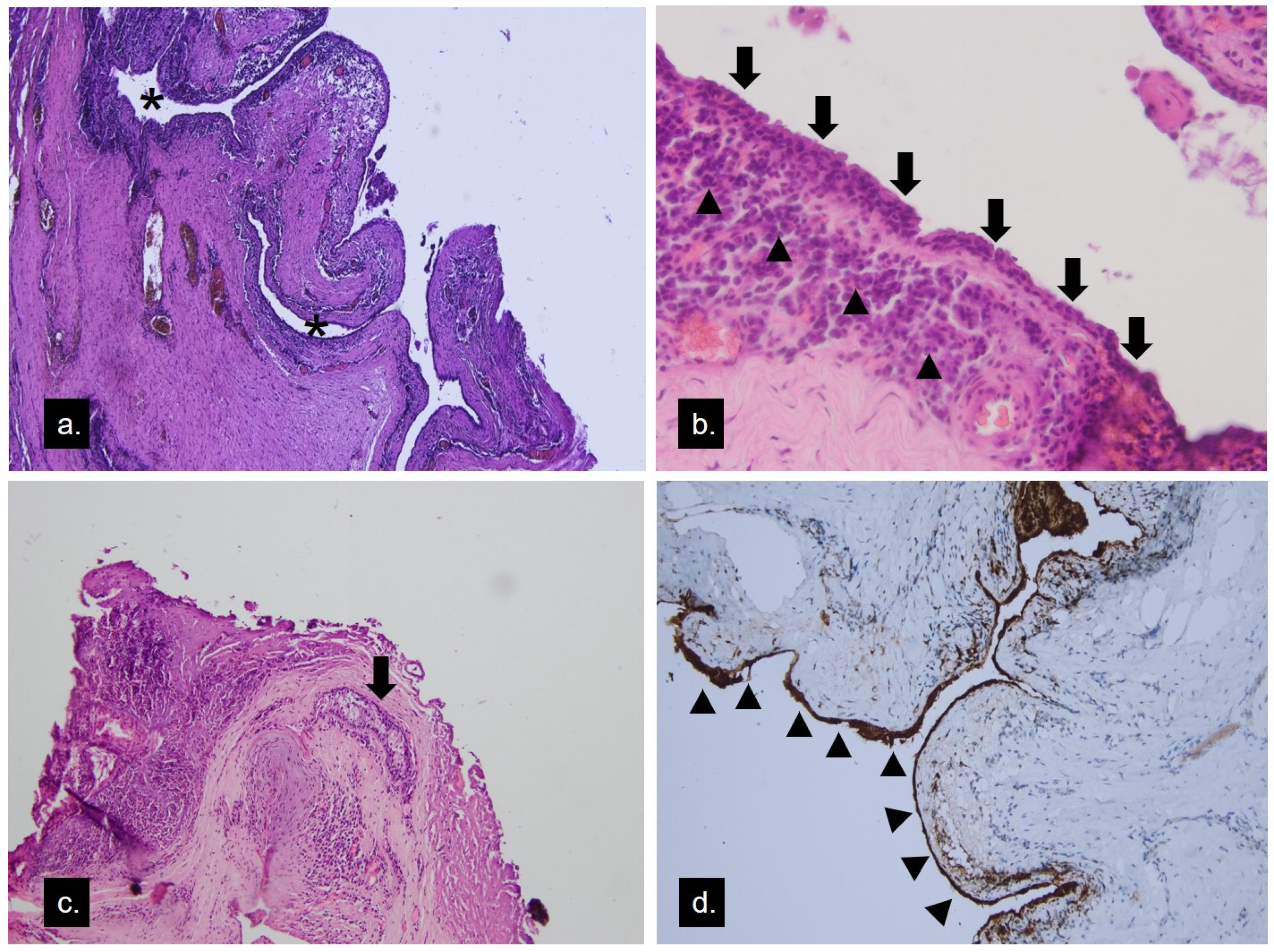
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mukherjee, B.; Desai, A.; Krishnakumar, S.; Biswas, J. A Giant Apocrine Hidrocystoma Presenting as Lacrimal Gland Mass. Orbit 2015, 34, 342–344. [Google Scholar] [CrossRef] [PubMed]
- McNab, A.A.; McKelvie, P. IgG4-Related Ophthalmic Disease. Part II: Clinical Aspects. Ophthalmic Plast. Reconstr. Surg. 2015, 31, 167–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goto, H.; Takahira, M.; Azumi, A. Diagnostic criteria for IgG4-related ophthalmic disease. JPN J. Ophthalmol. 2015, 59, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hafsi, W.; Badri, T.; Shah, F. Apocrine Hidrocystoma. In StatPearls; StatPearls Publishing LLC: Treasure Island, FL, USA, 2022. [Google Scholar]
- del Pozo, J.; García-Silva, J.; Peña-Penabad, C.; Fonseca, E. Multiple apocrine hidrocystomas: Treatment with carbon dioxide laser vaporization. J. Dermatol. Treat. 2001, 12, 97–100. [Google Scholar] [CrossRef]
- Ssi-Yan-Kai, I.C.; Pearson, A.R. Recurrent giant orbital apocrine hidrocystoma. Eye 2012, 26, 895–896. [Google Scholar] [CrossRef]
- Mehta, A.; Rao, A.; Khanna, A. Sudoriferous cyst of the orbit of adult origin after trauma. Indian J. Ophthalmol. 2008, 56, 235–237. [Google Scholar] [CrossRef]
- Barker-Griffith, A.E.; Streeten, B.W.; Charles, N.C. Moll gland neoplasms of the eyelid: A clinical and pathological spectrum in 5 cases. Arch. Ophthalmol. 2006, 124, 1645–1649. [Google Scholar] [CrossRef] [Green Version]
- Leivo, T.; Koskenmies, S.; Uusitalo, M.; Tynninen, O. IgG4-related disease mimicking chalazion in the upper eyelid with skin manifestations on the trunk. Int. Ophthalmol. 2015, 35, 595–597. [Google Scholar] [CrossRef]
- Mudhar, H.S.; Currie, Z.I.; Salvi, S.M. Lacrimal Gland Intra-Lobular Duct Cysts Associated with Focal Vasculitis. Ocul. Oncol. Pathol. 2015, 1, 225–230. [Google Scholar] [CrossRef] [Green Version]
- Umehara, H.; Okazaki, K.; Kawa, S.; Takahashi, H.; Goto, H.; Matsui, S.; Ishizaka, N.; Akamizu, T.; Sato, Y.; Kawano, M.; et al. The 2020 revised comprehensive diagnostic (RCD) criteria for IgG4-RD. Mod. Rheumatol. 2021, 31, 529–533. [Google Scholar] [CrossRef]
- Gan, L.; Luo, X.; Fei, Y.; Peng, L.; Zhou, J.; Li, J.; Lu, H.; Liu, Z.; Zhang, P.; Liu, X.; et al. Ophthalmic involvement disparities in clinical characteristics of IgG4-related disease: A retrospective study of 573 patients. BMC Ophthalmol. 2021, 21, 447. [Google Scholar] [CrossRef] [PubMed]
- Aziz, H.A.; Villa-Forte, A.; Plesec, T.P.; Singh, A.D. Isolated Conjunctival Inflammation Suggestive of IgG4-Related Disease. Ocul. Oncol. Pathol. 2015, 2, 51–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagai, T.; Yunoki, T.; Hayashi, A. A Case of IgG4-Related Bilateral Palpebral Conjunctivitis. Case Rep. Ophthalmol. 2019, 10, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.S.; Choi, W.; Kim, G.E.; Yoon, K.C. Case of Primary Isolated Subconjunctival IgG4-Related Disease. Cornea 2018, 37, 926–928. [Google Scholar] [CrossRef] [PubMed]
- Oles, K.; Skladzien, J.; Szczepanski, W.; Okon, K.; Leszczynska, J.; Bojanowska, E.; Bartus, K.; Mika, J. Immunoglobulin G4-related disease (IgG4-RD) in the orbit: Mucosa-associated lymphoid tissue (MALT)-type lymphomas. Med. Sci. Monit. 2015, 21, 1043–1050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strehl, J.D.; Hartmann, A.; Agaimy, A. Numerous IgG4-positive plasma cells are ubiquitous in diverse localised non-specific chronic inflammatory conditions and need to be distinguished from IgG4-related systemic disorders. J. Clin. Pathol. 2011, 64, 237–243. [Google Scholar] [CrossRef] [Green Version]
- Suimon, Y.; Kase, S.; Ishijima, K.; Kanno-Okada, H.; Ishida, S. Clinicopathological features of cystic lesions in the eyelid. Biomed. Rep. 2019, 10, 92–96. [Google Scholar] [CrossRef] [Green Version]
- Belaldavar, B.P.; Suranagi, V.; Kalakuntla, M.; Raj, B.; Tiwari, A. Apocrine Hidrocystoma: A Rare Case Report. Indian J. Otolaryngol. Head Neck Surg. 2019, 71, 59–61. [Google Scholar] [CrossRef]
- Cavanagh, M.; Pham, M.; Nguyen, J.; Tarbox, M. Postauricular apocrine hidrocystoma: A case and dermoscopy review. Derm. Online J. 2021, 27, 1–6. [Google Scholar] [CrossRef]
- Tachibana, T.; Sasaki, T.; Wani, Y.; Naoi, Y.; Kataoka, Y.; Nishizaki, K.; Ando, M. Apocrine Hidrocystoma of the External Auditory Canal in a Child. Otol. Neurotol. 2021, 42, e1181–e1183. [Google Scholar] [CrossRef]
- Requena, L.; Sánchez Yus, E. Follicular hybrid cysts. An expanded spectrum. Am. J. Dermatopathol. 1991, 13, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Serra, F.; Kaya, G. A New Case of Hybrid Epidermoid and Apocrine Cyst. Dermatopathology 2021, 8, 442–445. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, S.-Y.; Huang, J.-W.; Lee, Y.-C.; Chang, F.-L.; Li, M.-H.; Chen, N. Apocrine Hidrocystoma with IgG4 Plasma Cell Infiltration Presenting as Recurrent Chalazion: A Case Report. Medicina 2022, 58, 840. https://doi.org/10.3390/medicina58070840
Wu S-Y, Huang J-W, Lee Y-C, Chang F-L, Li M-H, Chen N. Apocrine Hidrocystoma with IgG4 Plasma Cell Infiltration Presenting as Recurrent Chalazion: A Case Report. Medicina. 2022; 58(7):840. https://doi.org/10.3390/medicina58070840
Chicago/Turabian StyleWu, Shang-Yen, Jin-Wei Huang, Yuan-Chieh Lee, Fang-Ling Chang, Ming-Hsun Li, and Nancy Chen. 2022. "Apocrine Hidrocystoma with IgG4 Plasma Cell Infiltration Presenting as Recurrent Chalazion: A Case Report" Medicina 58, no. 7: 840. https://doi.org/10.3390/medicina58070840