
Impact of Mirabegron Administration on the Blood Pressure and Pulse Rate in Patients with Overactive Bladder


Abstract
:1. Introduction
2. Materials and Methods
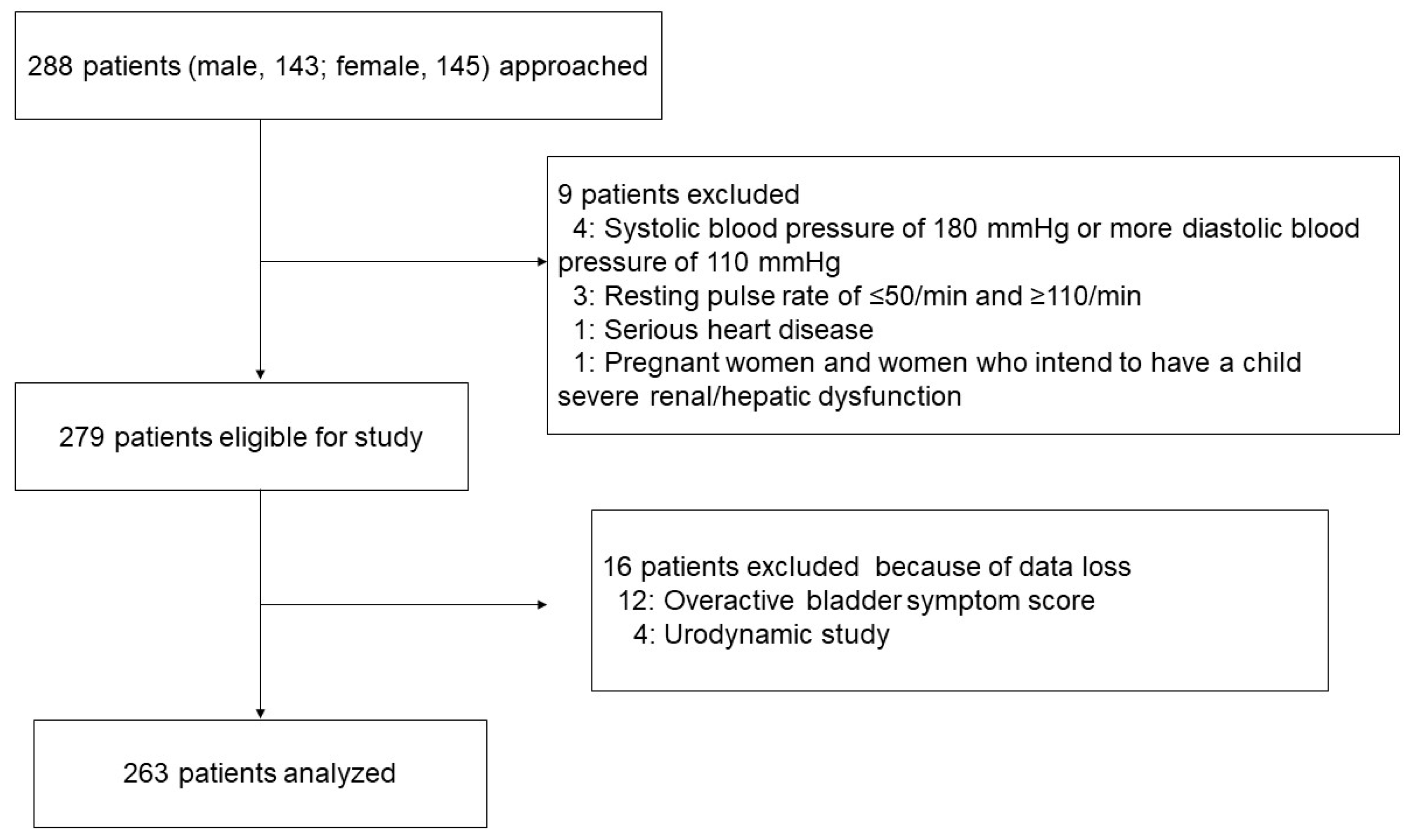
2.1. Patients and Study Design
2.2. Evaluation of BP and PR
2.3. Evaluation of Objective Findings
2.4. Propensity Score Matching
2.5. Statistical Analyses
3. Results
3.1. Patients’ Characteristics
3.2. Efficacy of Mirabegron for OAB Symptoms
3.3. Changes in the Hemodynamics Status during Mirabegron Treatment
3.4. Predictive Marker for the Clinically Significant Elevation of SBP
3.5. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abrams, P.; Cardozo, L.; Fall, M.; Griffiths, D.; Rosier, P.; Ulmsten, U.; van Kerrebroeck, P.; Victor, A.; Wein, A.; Standardisation Sub-committee of the International Continence Society. The standardisation of terminology of lower urinary tract function: Report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn 2002, 21, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.D.; Lin, T.L.; Hu, S.W.; Chen, Y.C.; Lin, L.Y. Prevalence and Correlation of Urinary Incontinence and Overactive Bladder in Taiwanese Women. Neurourol Urodyn 2003, 22, 109–117. [Google Scholar] [CrossRef]
- Stewart, W.F.; Van Rooyen, J.B.; Cundiff, G.W.; Abram, P.; Herzog, A.R.; Corey, R.; Hunt, T.L.; Wein, A.J. Prevalence and burden of overactive bladder in the United States. World J. Urol. 2003, 20, 327–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milsom, I.; Abrams, P.; Cardozo, L.; Roberts, R.G.; Thüroff, J.; Wein, A.J. How widespread are the symptoms of an overactive bladder and how are they managed? A population-based prevalence study. BJU Int. 2001, 87, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Gormley, E.A.; Lightner, D.J.; Burgio, K.L.; Chai, T.C.; Clemens, J.Q.; Culkin, D.J.; Das, A.K.; Foster, H.E.; Scarpero, H.M.; Tessier, C.D.; et al. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline. J. Urol. 2012, 188, 2455–2463. [Google Scholar] [CrossRef] [PubMed]
- Tse, V.; King, J.; Dowling, C.; English, S.; Gray, K.; Millard, R.; O’Connell, H.; Pillay, S.; Thavaseelan, J.; Urological Society of Australia and New Zealand; et al. Conjoint Urological Society of Australia and New Zealand (USANZ) and Urogynaecological Society of Australasia (UGSA) Guidelines on the management of adult non-neurogenic overactive bladder. BJU Int. 2016, 117, 34–47. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Ortega, G.; Walker, D.R.; Johnston, K.; Mickel, A.; Harrigan, S.; Rogula, B.; Kristy, R.M.; Hairston, J.C.; Schermer, C.R. Comparative Safety and Efficacy of Treatments for Overactive Bladder Among Older Adults: A Network Meta-analysis. Drugs Aging 2020, 37, 801–816. [Google Scholar] [CrossRef]
- White, W.B.; Chapple, C.; Gratzke, C.; Herschorn, S.; Robinson, D.; Frankel, J.; Ridder, A.; Stoelzel, M.; Paireddy, A.; van Maanen, R.; et al. Cardiovascular Safety of the β3-Adrenoceptor Agonist Mirabegron and the Antimuscarinic Agent Solifenacin in the SYNERGY Trial. J. Clin. Pharmacol. 2018, 58, 1084–1091. [Google Scholar] [CrossRef] [PubMed]
- Sexton, C.C.; Coyne, K.S.; Thompson, C.; Bavendam, T.; Chen, C.I.; Markland, A. Prevalence and effect on health-related quality of life of overactive bladder in older americans: Results from the epidemiology of lower urinary tract symptoms study. J. Am. Geriatr. Soc. 2011, 59, 1465–1470. [Google Scholar] [CrossRef]
- Hiriscau, E.I.; Buzdugan, E.C.; Hui, L.A.; Bodolea, C. Exploring the Relationship between Frailty, Functional Status, Polypharmacy, and Quality of Life in Elderly and Middle-Aged Patients with Cardiovascular Diseases: A One-Year Follow-Up Study. Int. J. Environ. Res. Public Health. 2022, 19, 2286. [Google Scholar] [CrossRef]
- Slawuta, A.; Jacek, P.; Mazur, G.; Polanska-Jankowska, B. Quality of Life and Frailty Syndrome in Patients with Atrial Fibrillation. Clin. Interv. Aging 2020, 15, 783–795. [Google Scholar] [CrossRef] [PubMed]
- Homma, Y.; Yoshida, M.; Seki, N.; Yokoyama, O.; Kakizaki, H.; Gotoh, M.; Yamanishi, T.; Yamaguchi, O.; Takeda, M.; Nishizawa, O. Symptom assessment tool for overactive bladder syndrome-overactive bladder symptom score. Urology 2006, 68, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Staessen, J.A.; Gasowski, J.; Wang, J.G.; Thijs, L.; Den Hond, E.; Boissel, J.P.; Coope, J.; Ekbom, T.; Gueyffier, F.; Liu, L.; et al. Risks of untreated and treated isolated systolic hypertension in the elderly: Meta-analysis of outcome trials. Lancet 2000, 355, 865–872. [Google Scholar] [CrossRef]
- Weber, M.A.; Chapple, C.R.; Gratzke, C.; Herschorn, S.; Robinson, D.; Frankel, J.M.; Ridder, A.M.; Stoelzel, M.; Paireddy, A.; Van Maanen, R.; et al. A strategy utilizing ambulatory monitoring and home and clinic blood pressure measurements to optimize the safety evaluation of noncardiovascular drugs with potential for hemodynamic effects: A report from the SYNERGY trial. Blood Press. Monit. 2018, 23, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Drake, M.J.; MacDiarmid, S.; Chapple, C.R.; Esen, A.; Athanasiou, S.; Cambronero Santos, J.; Mitcheson, D.; Herschorn, S.; Siddiqui, E.; Huang, M.; et al. Cardiovascular safety in refractory incontinent patients with overactive bladder receiving add-on mirabegron therapy to solifenacin (BESIDE). Int. J. Clin. Pract. 2017, 71, e12944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.L.; Chen, T.C.; Chang, H.M.; Juan, Y.S.; Huang, W.H.; Pan, H.F.; Chang, Y.C.; Wu, C.M.; Wang, Y.L.; Lee, H.Y. Mirabegron is alternative to antimuscarinic agents for overactive bladder without higher risk in hypertension: A systematic review and meta-analysis. World J. Urol. 2018, 36, 1285–1297. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.; Peterson, G.M.; Bereznicki, L.R.; Salahudeen, M.S. Association between anticholinergic drug burden and mortality in older people: A systematic review. Eur. J. Clin. Pharmacol. 2020, 76, 319–335. [Google Scholar] [CrossRef]
- Makhani, A.; Thake, M.; Gibson, W. Mirabegron in the treatment of overactive bladder: Safety and efficacy in the very elderly patient. Clin. Interv. Aging 2020, 15, 575–581. [Google Scholar] [CrossRef] [Green Version]
- Wagg, A.; Staskin, D.; Engel, E.; Herschorn, S.; Kristy, R.M.; Schermer, C.R. Efficacy, safety, and tolerability of mirabegron in patients aged ≥65 yr with overactive bladder wet: A phase IV, double-blind, randomised, placebo-controlled study (PILLAR). Eur. Urol. 2020, 77, 211–220. [Google Scholar] [CrossRef]
- Chapple, C.R.; Kaplan, S.A.; Mitcheson, D.; Klecka, J.; Cummings, J.; Drogendijk, T.; Dorrepaal, C.; Martin, N. Randomized double-blind, active-controlled phase 3 study to assess 12-month safety and efficacy of mirabegron, a β(3)-adrenoceptor agonist, in overactive bladder. Eur. Urol. 2013, 63, 296–305. [Google Scholar] [CrossRef]
- Imran, M.; Najmi, A.K.; Tabrez, S. Mirabegron for Overactive Bladder: A novel, first-in-class β3- agonist therapy. Urol. J. 2013, 10, 935–940. [Google Scholar] [PubMed]
- Katoh, T.; Kakizaki, H.; Lee, K.S.; Ishida, K.; Katou, D.; Yamamoto, O.; Jong, J.J.; Sumarsono, B.; Uno, S.; Yamaguchi, O. Cardiovascular safety of mirabegron add-on therapy to tamsulosin for the treatment of overactive bladder in men with lower urinary tract symptoms: A post hoc analysis from the MATCH study. Low. Urin. Tract Symptoms 2021, 13, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, V.; Hallas, J.; Linder, M.; Margulis, A.V.; Suehs, B.T. Cardiovascular Risk in Users of Mirabegron Compared with Users of Antimuscarinic Treatments for Overactive Bladder: Findings from a Non-Interventional, Multinational, Cohort Study. Drug Saf. 2021, 44, 899–915. [Google Scholar] [CrossRef]
- Van Gelderen, M.; Stölzel, M.; Meijer, J.; Kerbusch, V.; Collins, C.; Korstanje, C. An Exploratory Study in Healthy Male Subjects of the Mechanism of Mirabegron-Induced Cardiovascular Effects. J. Clin. Pharmacol. 2017, 57, 1534–1544. [Google Scholar] [CrossRef]
- Pagan, L.U.; Gomes, M.J.; Gatto, M.; Mota, G.A.F.; Okoshi, K.; Okoshi, M.P. The Role of Oxidative Stress in the Aging Heart. Antioxidants. 2022, 11, 336. [Google Scholar] [CrossRef] [PubMed]
- Bubb, K.J.; Ravindran, D.; Cartland, S.P.; Finemore, M.; Clayton, Z.E.; Tsang, M.; Tang, O.; Kavurma, M.M.; Patel, S.; Figtree, G.A. β3 Adrenergic Receptor Stimulation Promotes Reperfusion in Ischemic Limbs in a Murine Diabetic Model. Front. Pharmacol. 2021, 12, 666334. [Google Scholar] [CrossRef]
- Khullar, V.; Amarenco, G.; Angulo, J.C.; Cambronero, J.; Høye, K.; Milsom, I.; Radziszewski, P.; Rechberger, T.; Boerrigter, P.; Drogendijk, T.; et al. Efficacy and tolerability of mirabegron, a β(3)-adrenoceptor agonist, in patients with overactive bladder: Results from a randomised European-Australian phase 3 trial. Eur. Urol. 2013, 63, 283–295. [Google Scholar] [CrossRef]
- Nitti, V.W.; Auerbach, S.; Martin, N.; Calhoun, A.; Lee, M.; Herschorn, S. Results of a randomized phase III trial of mirabegron in patients with overactive bladder. J. Urol. 2013, 189, 1388–1395. [Google Scholar] [CrossRef]
- Yamaguchi, O.; Kakizaki, H.; Homma, Y.; Igawa, Y.; Takeda, M.; Nishizawa, O.; Gotoh, M.; Yoshida, M.; Yokoyama, O.; Seki, N.; et al. Long-term safety and efficacy of antimuscarinic add-on therapy in patients with overactive bladder who had a suboptimal response to mirabegron monotherapy: A multicenter, randomized study in Japan (MILAI II study). Int. J. Urol. 2019, 26, 342–352. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Question | Frequency | Score |
|---|---|---|
| 1. How many times do you typically urinate from waking in the morning until sleeping at night? | ≤7 | 0 |
| 8–14 | 1 | |
| ≥15 | 2 | |
| 2. How many times do you typically wake up to urinate from sleeping at night until waking in the morning? | 0 | 0 |
| 1 | 1 | |
| 2 | 2 | |
| ≥3 | 3 | |
| 3. How often do you have a sudden desire to urinate, which is difficult to defer? | Not at all | 0 |
| Less than once a week | 1 | |
| Once a week or more | 2 | |
| About once a day | 3 | |
| 2–4 times a day | 4 | |
| 5 times a day or more | 5 | |
| 4. How often do you leak urine because you cannot defer the sudden desire to urinate? | Not at all | 0 |
| Less than once a week | 1 | |
| Once a week or more | 2 | |
| About once a day | 3 | |
| 2–4 times a day | 4 | |
| 5 times a day or more | 5 |
| Total Group | Young Group | Elderly Group | p | |
|---|---|---|---|---|
| Number of patients (Male, %) | 263 (131, 49.8) | 54 (15, 27.8) | 209 (116, 55.5) | <0.001 |
| Age (years) | 73.1 ± 11.6 | 54.9 ± 7.7 | 77.8 ± 6.8 | <0.001 |
| Body mass index (kg/m2) | 22.6 ± 3.9 | 23.2 ± 5.1 | 22.5 ± 3.6 | 0.938 |
| Overactive bladder symptom score | ||||
| Q1 Daytime frequency | 1.0 ± 0.7 | 0.9 ± 0.7 | 1.0 ± 0.7 | 0.689 |
| Q2 Nighttime frequency | 2.3 ± 0.7 | 2.1 ± 0.7 | 2.4 ± 0.7 | 0.007 |
| Q3 Urgency | 3.1 ± 1.3 | 2.9 ± 1.3 | 3.1 ± 1.2 | 0.010 |
| Q4 Urgency incontinence | 1.1 ± 1.3 | 0.9 ± 1.3 | 1.1 ± 1.4 | 0.225 |
| Total score | 7.5 ± 2.7 | 6.9 ± 2.5 | 7.6 ± 2.7 | 0.011 |
| Urodynamic study | ||||
| Voided volume (mL) | 154.2 ± 52.8 | 178.1 ± 61.4 | 148.1 ± 48.6 | <0.001 |
| Qmax (mL/sec) | 14.6 ± 5.0 | 17.4 ± 4.6 | 13.9 ± 4.8 | <0.001 |
| Post-void residual urine (mL) | 24.2 ± 12.3 | 23.0 ± 14.6 | 24.5 ± 11.7 | 0.167 |
| Blood pressure | ||||
| Systolic blood pressure (mmHg) | 127.5 ± 16.2 | 124.2 ± 15.0 | 128.4 ± 16.4 | 0.148 |
| Diastolic blood pressure (mmHg) | 71.2 ± 11.4 | 70.3 ± 14.0 | 71.5 ± 10.6 | 0.390 |
| Pulse rate (/min) | 74.5 ± 12.1 | 75.0 ± 11.0 | 74.3 ± 12.3 | 0.677 |
| Comorbidity | ||||
| Hypertension (%) | 128 (48.7) | 12 (22.2) | 116 (55.5) | <0.001 |
| Diabetes Miletus (%) | 29 (11.0) | 6 (11.1) | 23 (11.0) | 1.000 |
| Hyperlipidemia (%) | 41 (15.6) | 3 (5.6) | 38 (18.2) | 0.023 |
| Chronic renal dysfunction (%) | 78 (29.7) | 6 (16.7) | 69 (33.0) | 0.020 |
| Treatment for Hypertension | 0.912 | |||
| ARBs (% in Hypertension) | 46 (35.9) | 4 (8.7) | 42 (91.3) | |
| CCBs (% in Hypertension) | 33 (25.8) | 4 (12.1) | 29 (87.9) | |
| ARBs + CCBs (% in Hypertension) | 28 (21.9) | 2 (7.1) | 26 (93.9) | |
| ARB + diuretics (% in Hypertension) | 16 (12.5) | 2 (12.5) | 14 (87.5) | |
| Diuretics (% in Hypertension) | 5 (3.9) | 0 (0) | 5 (100) | |
| BPH (% in male) | 94 (71.8) | 9 (60.0) | 85 (73.3) | 0.360 |
| Treatment for BPH (% in BPH) | 93 (98.9) | 8 (88.9) | 85 (100) | 0.096 |
| α1 receptor antagonists (% in BPH) | 87 (93.5) | 7 (87.5) | 80 (94.1) | 0.426 |
| Phosphodiesterase 5 inhibitors (% in BPH) | 6 (6.5) | 1 (12.5) | 5 (5.9) |
| Total Group | Young Group | Elderly Group | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 W | 12 W | p | 0 W | 12 W | p | 0 W | 12 W | p | |
| OABSS | |||||||||
| Q1 Daytime frequency | 1.0 ± 0.7 | 0.8 ± 0.7 | <0.001 | 0.9 ± 0.7 | 0.9 ± 0.6 | 0.833 | 1.0 ± 0.7 | 0.8 ± 0.7 | <0.001 |
| Q2 Nighttime frequency | 2.3 ± 0.7 | 1.8 ± 0.8 | <0.001 | 2.1 ± 0.7 | 1.6 ± 0.8 | <0.001 | 2.4 ± 0.7 | 1.8 ± 0.8 | <0.001 |
| Q3 Urgency | 3.1 ± 1.3 | 1.2 ± 1.1 | <0.001 | 2.9 ± 1.3 | 1.4 ± 1.3 | <0.001 | 3.1 ± 1.2 | 1.2 ± 1.1 | <0.001 |
| Q4 Urgency incontinence | 1.1 ± 1.3 | 0.7 ± 0.9 | <0.001 | 0.9 ± 1.3 | 0.8 ± 1.0 | 0.324 | 1.1 ± 1.4 | 0.7 ± 0.9 | <0.001 |
| Total score | 7.5 ± 2.7 | 4.5 ± 2.5 | <0.001 | 6.9 ± 2.5 | 4.7 ± 2.7 | <0.001 | 7.6 ± 2.7 | 4.4 ± 2.5 | <0.001 |
| Urodynamic study | |||||||||
| VV (mL) | 154.2 ± 52.8 | 179.8 ± 54.2 | <0.001 | 178.1 ± 61.4 | 203.8 ± 67.9 | 0.005 | 148.1 ± 48.6 | 173.6 ± 48.4 | <0.001 |
| Qmax (mL/s) | 14.6 ± 5.0 | 13.6 ± 4.5 | 0.228 | 17.4 ± 4.6 | 16.7 ± 3.9 | 0.119 | 13.9 ± 4.8 | 13.3 ± 4.4 | 0.201 |
| PVR (mL) | 24.2 ± 12.3 | 25.1 ± 12.4 | 0.120 | 23.0 ± 14.6 | 23.6 ± 12.9 | 0.230 | 24.5 ± 11.7 | 25.8 ± 12.2 | 0.315 |
| Total Group | Young Group | Elderly Group | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 W | 12 W | p | 0 W | 12 W | p | 0 W | 12 W | p | |
| SBP(mmHg) | 127.5 ± 16.2 | 126.2 ± 14.9 | 0.148 | 124.2 ± 15.0 | 122.3 ± 16.0 | 0.282 | 128.4 ± 16.4 | 127.2 ± 14.4 | 0.266 |
| DBP(mmHg) | 71.2 ± 11.4 | 69.8 ± 10.7 | 0.041 | 70.3 ± 14.0 | 71.0 ± 12.5 | 0.681 | 71.5 ± 10.6 | 69.5 ± 10.2 | 0.012 |
| Pulse rate (/min) | 74.5 ± 12.1 | 74.0 ± 11.5 | 0.449 | 75.0 ± 11.0 | 74.9 ± 12.2 | 0.871 | 74.3 ± 12.3 | 73.8 ± 11.3 | 0.453 |
| Normotensive n = 135 | Hypertensive n = 128 | |||||
|---|---|---|---|---|---|---|
| 0 W | 12 W | p | 0 W | 12 W | p | |
| SBP(mmHg) | 123.1 ± 16.3 | 122.1 ± 14.5 | 0.916 | 132.3 ± 14.8 | 130.4 ± 14.0 | 0.118 |
| DBP(mmHg) | 70.8 ± 11.9 | 69.2 ± 11.6 | 0.322 | 71.7 ± 10.8 | 70.5 ± 9.7 | 0.199 |
| Pulse rate (/min) | 75.3 ± 12.3 | 74.7 ± 11.6 | 0.492 | 73.6 ± 11.8 | 73.3 ± 11.5 | 0.604 |
| SBP | DBP | PR | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 W | 12 W | p | 0 W | 12 W | p | 0 W | 12 W | p | |
| ARBs | 131.4 ± 15.4 | 130.5 ± 14.7 | 0.216 | 69.9 ± 10.8 | 70.5 ± 9.9 | 0546 | 74.0 ± 12.3 | 74.6 ± 9.4 | 0.931 |
| CCBs | 132.4 ± 12.5 | 131.3 ± 18.2 | 0.203 | 73.5 ± 11.8 | 70.5 ± 10.1 | 0.111 | 73.8 ± 12.6 | 73.1 ± 15.9 | 0.662 |
| ARBs + CCBs | 133.1 ± 16.3 | 130.6 ± 15.7 | 0.571 | 71.6 ± 11.9 | 70.7 ± 9.2 | 0.571 | 72.8 ± 12.4 | 72.0 ± 9.8 | 0.377 |
| ARB + diuretics | 130.4 ± 16.6 | 132.6 ± 14.2 | 0.734 | 71.4 ± 7.1 | 70.3 ± 9.7 | 0.613 | 75.3 ± 10.4 | 73.8 ± 10.6 | 0.270 |
| Diuretics | 140.4 ± 8.8 | 135.0 ± 17.1 | 0.625 | 78.2 ± 7.5 | 69.4 ± 13.4 | 0.250 | 68.2 ± 3.7 | 68.0 ± 5.7 | 0.750 |
| Univariate Analysis | |||
|---|---|---|---|
| OR | 95% CI | p | |
| Age (≥65 years) | 2.77 | 1.13–8.31 | 0.024 |
| Gender: male | 0.96 | 0.53–1.76 | 0.902 |
| Body mass index | 0.97 | 0.90–1.05 | 0.394 |
| Hypertension: presence | 0.77 | 0.41–1.40 | 0.389 |
| Diabetes Miletus: presence | 1.04 | 0.37–2.55 | 0.939 |
| Hyperlipidemia: presence | 1.14 | 0.48–2.47 | 0.757 |
| Chronic renal dysfunction: presence | 1.03 | 0.52–1.96 | 0.925 |
| <65 y. o (Young Group) n = 51 | ≥65 y. o (Elderly Group) n = 51 | p | Standardized Mean Differences | |
|---|---|---|---|---|
| Gender (male/female) | 15/36 | 15/36 | 0.786 | 0.089 |
| Body mass index (kg/m2) | 23.1 ± 5.2 | 22.4 ± 4.2 | 0.481 | 0.028 |
| Hypertension (%) | 12 (23.5) | 13 (25.5) | 1.000 | 0.075 |
| Diabetes Miletus (%) | 6 (11.8) | 5 (9.8) | 1.000 | 0.099 |
| Hyperlipidemia (%) | 3 (5.9) | 1 (2.0) | 0.617 | 0.098 |
| Chronic renal dysfunction (%) | 9 (17.6) | 7 (13.7) | 0.786 | 0.065 |
| SBP at baseline (mmHg) | 123.8 ± 15.2 | 121.6 ± 12.8 | 0.411 | 0.001 |
| <65 Years (Young Group) n = 51 | ≥65 Years (Elderly Group) n = 51 | p | |
|---|---|---|---|
| SBP elevation (%) | 4 (7.8) | 18 (35.3) | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ito, H.; Matsuo, T.; Mitsunari, K.; Ohba, K.; Miyata, Y. Impact of Mirabegron Administration on the Blood Pressure and Pulse Rate in Patients with Overactive Bladder. Medicina 2022, 58, 825. https://doi.org/10.3390/medicina58060825
Ito H, Matsuo T, Mitsunari K, Ohba K, Miyata Y. Impact of Mirabegron Administration on the Blood Pressure and Pulse Rate in Patients with Overactive Bladder. Medicina. 2022; 58(6):825. https://doi.org/10.3390/medicina58060825
Chicago/Turabian StyleIto, Hidenori, Tomohiro Matsuo, Kensuke Mitsunari, Kojiro Ohba, and Yasuyoshi Miyata. 2022. "Impact of Mirabegron Administration on the Blood Pressure and Pulse Rate in Patients with Overactive Bladder" Medicina 58, no. 6: 825. https://doi.org/10.3390/medicina58060825