
Endothelial Microparticles as Potential Biomarkers in the Assessment of Endothelial Dysfunction in Hypercholesterolemia

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
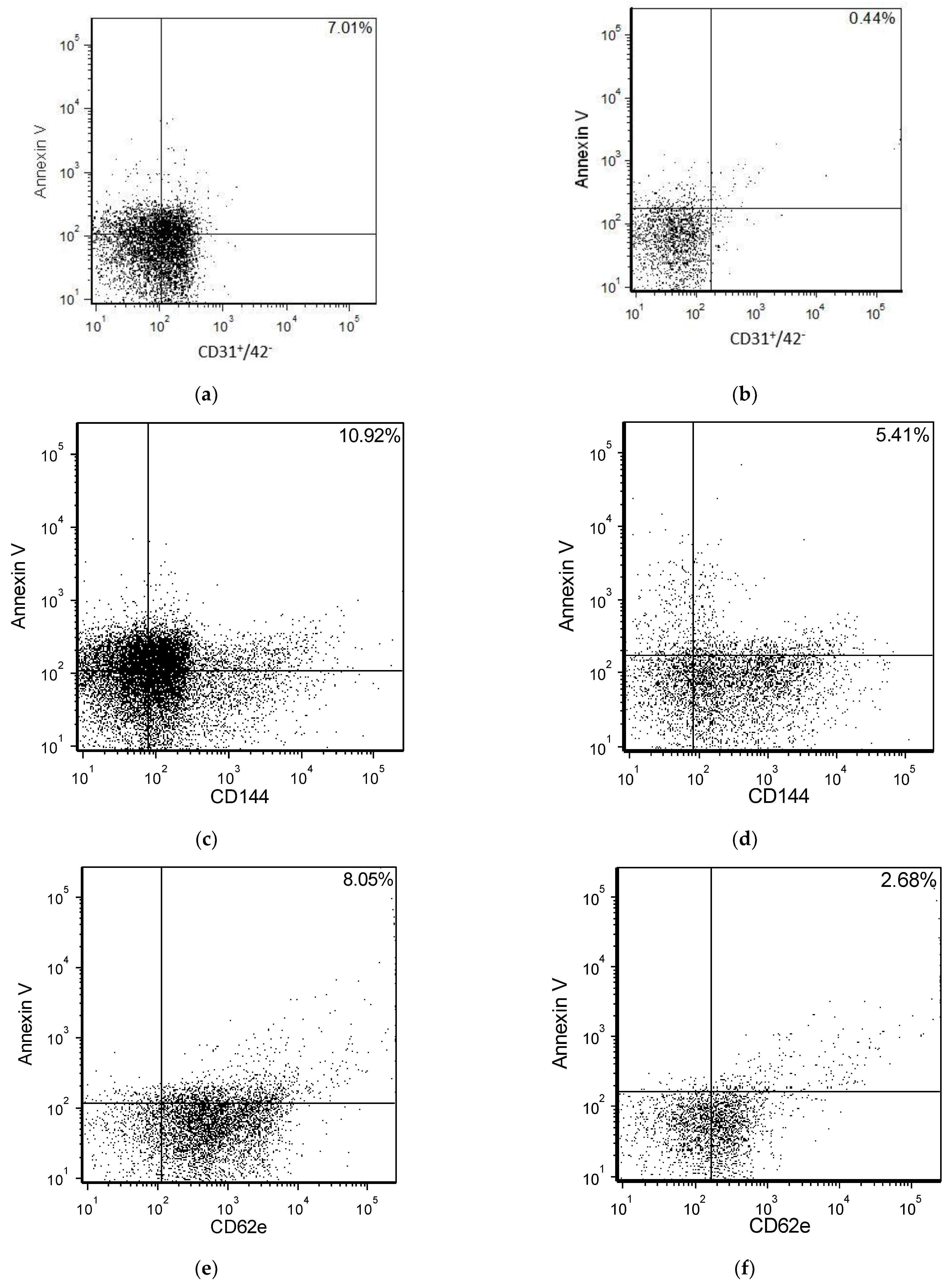
2.2. EMP Quantification
2.3. Endothelial Function Assessment by PWA
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stanek, A.; Fazeli, B.; Bartuś, S.; Sutkowska, E. The Role of Endothelium in Physiological and Pathological States: New Data. Biomed Res. Int. 2018, 2018, 1098039. [Google Scholar] [CrossRef] [Green Version]
- Dubois-deruy, E.; Peugnet, V.; Turkieh, A.; Pinet, F. Oxidative Stress in Cardiovascular Diseases. Antioxidants 2020, 9, 864. [Google Scholar] [CrossRef]
- Jakubiak, G.K.; Cie, G. Nitrotyrosine, Nitrated Lipoproteins, and Cardiovascular Dysfunction in Patients with Type 2 Diabetes: What Do We Know and What Remains to Be Explained ? Antioxidants 2022, 11, 856. [Google Scholar] [CrossRef]
- Senoner, T.; Dichtl, W. Oxidative Stress in Cardiovascular Diseases: Still a Therapeutic Target? Nutrients 2019, 11, 2090. [Google Scholar] [CrossRef] [Green Version]
- Jakubiak, G.K.; Osadnik, K.; Lejawa, M.; Osadnik, T.; Goławski, M.; Lewandowski, P.; Pawlas, N. “Obesity and Insulin Resistance” Is the Component of the Metabolic Syndrome Most Strongly Associated with Oxidative Stress. Antioxidants 2022, 11, 79. [Google Scholar] [CrossRef]
- Celermajer, D.S.; Sorensen, K.E.; Gooch, V.M.; Miller, O.I.; Sullivan, I.D.; Lloyd, J.K.; Deanfield, J.E.; Spiegelhalter, D.J. Non-Invasive Detection of Endothelial Dysfunction in Children and Adults at Risk of Atherosclerosis. Lancet 1992, 340, 1111–1115. [Google Scholar] [CrossRef]
- Xu, S.; Ilyas, I.; Little, P.J.; Li, H.; Kamato, D.; Zheng, X.; Luo, S.; Li, Z.; Liu, P.; Han, J.; et al. Endothelial Dysfunction in Atherosclerotic Cardiovascular Diseases and beyond: From Mechanism to Pharmacotherapies. Pharmacol. Rev. 2021, 73, 924–967. [Google Scholar] [CrossRef]
- Lugo-Gavidia, L.M.; Burger, D.; Matthews, V.B.; Nolde, J.M.; Galindo Kiuchi, M.; Carnagarin, R.; Kannenkeril, D.; Chan, J.; Joyson, A.; Herat, L.Y.; et al. Role of Microparticles in Cardiovascular Disease: Implications for Endothelial Dysfunction, Thrombosis, and Inflammation. Hypertension 2021, 77, 1825–1844. [Google Scholar] [CrossRef]
- Vítková, V.; Živný, J.; Janota, J. Endothelial Cell-Derived Microvesicles: Potential Mediators and Biomarkers of Pathologic Processes. Biomark. Med. 2018, 12, 161–175. [Google Scholar] [CrossRef]
- Storch, A.S.; de Mattos, J.D.; Alves, R.; dos Santos Galdino, I.; Rocha, H.N.M. Methods of Endothelial Function Assessment: Description and Applications. Int. J. Cardiovasc. Sci. 2017, 30, 262–273. [Google Scholar] [CrossRef]
- Silambanan, S.; Hermes, R.S.; Bhaskar, E.; Gayathri, S. Endothelial Microparticle as an Early Marker of Endothelial Dysfunction in Patients with Essential Hypertension: A Pilot Study. Indian J. Clin. Biochem. 2020, 35, 245–250. [Google Scholar] [CrossRef]
- Leite, A.R.; Borges-Canha, M.; Cardoso, R.; Neves, J.S.; Castro-Ferreira, R.; Leite-Moreira, A. Novel Biomarkers for Evaluation of Endothelial Dysfunction. Angiology 2020, 71, 397–410. [Google Scholar] [CrossRef]
- Boulanger, C.M.; Loyer, X.; Rautou, P.E.; Amabile, N. Extracellular Vesicles in Coronary Artery Disease. Nat. Rev. Cardiol. 2017, 14, 259–272. [Google Scholar] [CrossRef]
- Chen, Y.; Li, G.; Liu, M.L. Microvesicles as Emerging Biomarkers and Therapeutic Targets in Cardiometabolic Diseases. Genom. Proteom. Bioinforma 2018, 16, 50–62. [Google Scholar] [CrossRef]
- Latham, S.L.; Tiberti, N.; Gokoolparsadh, N.; Holdaway, K.; Couraud, P.O.; Grau, G.E.R.; Combes, V. Immuno-Analysis of Microparticles: Probing at the Limits of Detection. Sci. Rep. 2015, 5, 16314. [Google Scholar] [CrossRef] [Green Version]
- Paudel, K.R.; Panth, N.; Kim, D.-W. Circulating Endothelial Microparticles: A Key Hallmark of Atherosclerosis Progression. Scientifica 2016, 2016, 8514056. [Google Scholar] [CrossRef] [Green Version]
- Stockelman, K.A.; Hijman, J.G.; Bammet, T.D.; Greiner, J.J.; Stauffer, B.L.; DeSouza, C.A. Circulating Endothelial Cell-Derived Microvesicles Are Elevated with Hypertension and Associated with Endothelial Dysfunction. Can. J. Physiol. Pharmacol. 2021, 98, 557–561. [Google Scholar] [CrossRef]
- Sansone, R.; Baaken, M.; Horn, P.; Schuler, D.; Westenfeld, R.; Amabile, N.; Kelm, M.; Heiss, C. Endothelial Microparticles and Vascular Parameters in Subjects with and without Arterial Hypertension and Coronary Artery Disease. Data Br. 2018, 19, 495–500. [Google Scholar] [CrossRef]
- de Hoog, V.C.; Timmers, L.; Schoneveld, A.H.; Wang, J.W.; Van de Weg, S.M.; Sze, S.K.; Van Keulen, J.K.; Hoes, A.W.; Den Ruijter, H.M.; de Kleijn, D.P.; et al. Serum Extracellular Vesicle Protein Levels Are Associated with Acute Coronary Syndrome. Eur. Heart J. Acute Cardiovasc. Care 2013, 2, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Simak, J.; Gelderman, M.P.; Yu, H.; Wright, V.; Baird, A.E. Circulating Endothelial Microparticles in Acute Ischemic Stroke: A Link to Severity, Lesion Volume and Outcome. J. Thromb. Haemost. 2006, 4, 1296–1302. [Google Scholar] [CrossRef]
- Deng, F.; Wang, S.; Zhang, L. Endothelial Microparticles Act as Novel Diagnostic and Therapeutic Biomarkers of Circulatory Hypoxia-Related Diseases: A Literature Review. J. Cell. Mol. Med. 2017, 21, 1698–1710. [Google Scholar] [CrossRef]
- Tramontano, A.F.; Lyubarova, R.; Tsiakos, J.; Palaia, T.; Deleon, J.R.; Ragolia, L. Circulating Endothelial Microparticles in Diabetes Mellitus. Mediat. Inflamm. 2010, 2010, 250476. [Google Scholar] [CrossRef]
- Esposito, K.; Ciotola, M.; Schisano, B.; Gualdiero, R.; Sardelli, L.; Misso, L.; Giannetti, G.; Giugliano, D. Endothelial Microparticles Correlate with Endothelial Dysfunction in Obese Women. J. Clin. Endocrinol. Metab. 2006, 91, 3676–3679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, F.; Li, Q.; Pfeifer, A.; Werner, N. Endothelial- and Immune Cell-Derived Extracellular Vesicles in the Regulation of Cardiovascular Health and Disease. JACC Basic Transl. Sci. 2017, 2, 790–807. [Google Scholar] [CrossRef]
- Berezin, A.E.; Berezin, A.A. Endothelial Cell-Derived Extracellular Vesicles in Atherosclerosis: The Emerging Value for Diagnosis, Risk Stratification and Prognostication. Vessel Plus 2020, 4, 15. [Google Scholar] [CrossRef]
- Stoner, L.; Young, J.M.; Fryer, S. Assessments of Arterial Stiffness and Endothelial Function Using Pulse Wave Analysis. Int. J. Vasc. Med. 2012, 2012, 903107. [Google Scholar] [CrossRef] [Green Version]
- Amabile, N.; Guérin, A.P.; Leroyer, A.; Mallat, Z.; Nguyen, C.; Boddaert, J.; London, G.M.; Tedgui, A.; Boulanger, C.M. Circulating Endothelial Microparticles Are Associated with Vascular Dysfunction in Patients with End-Stage Renal Failure. J. Am. Soc. Nephrol. 2005, 16, 3381–3388. [Google Scholar] [CrossRef] [Green Version]
- Sansone, R.; Baaken, M.; Horn, P.; Schuler, D.; Westenfeld, R.; Amabile, N.; Kelm, M.; Heiss, C. Release of Endothelial Microparticles in Patients with Arterial Hypertension, Hypertensive Emergencies and Catheter-Related Injury. Atherosclerosis 2018, 273, 67–74. [Google Scholar] [CrossRef]
- Chowienczyk, P.J.; Watts, G.F.; Cockcroft, J.R.; Ritter, J.M. Impaired Endothelium-Dependent Vasodilation of Forearm Resistance Vessels in Hypercholesterolaemia. Lancet 1992, 340, 1430–1432. [Google Scholar] [CrossRef]
- Hermida, N.; Balligand, J.L. Low-Density Lipoprotein-Cholesterol-Induced Endothelial Dysfunction and Oxidative Stress: The Role of Statins. Antioxid. Redox Signal. 2014, 20, 1216–1237. [Google Scholar] [CrossRef]
- Schiffrin, E.L. Vascular Remodeling in Hypertension: Mechanisms and Treatment. Hypertension 2012, 59, 367–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jy, W.; Horstman, L.L.; Jimenez, J.J.; Ahn, Y.S.; Biró, É.; Nieuwland, R.; Sturk, A.; Dignat-George, F.; Sabatier, F.; Camoin-Jau, L.; et al. Measuring Circulating Cell-Derived Microparticles. J. Thromb. Haemost. 2004, 2, 1842–1843. [Google Scholar] [CrossRef] [PubMed]
- Navasiolava, N.M.; Dignat-George, F.; Sabatier, F.; Larina, I.M.; Demiot, C.; Fortrat, J.O.; Gauquelin-Koch, G.; Kozlovskaya, I.B.; Custaud, M.A. Enforced Physical Inactivity Increases Endothelial Microparticle Levels in Healthy Volunteers. Am. J. Physiol. Heart Circ. Physiol. 2010, 299, 248–256. [Google Scholar] [CrossRef]
- Lacroix, R.; Judicone, C.; Mooberry, M.; Boucekine, M.; Key, N.S.; Dignat-George, F.; Ambrozic, A.; Bailly, N.; Buffat, C.; Buzas, E.; et al. Standardization of Pre-Analytical Variables in Plasma Microparticle Determination: Results of the International Society on Thrombosis and Haemostasis SSC Collaborative Workshop. J. Thromb. Haemost. 2013, 11, 1190–1193. [Google Scholar] [CrossRef]
- Dey-Hazra, E.; Hertel, B.; Kirsch, T.; Woywodt, A.; Lovric, S.; Haller, H.; Haubitz, M.; Erdbruegger, U. Detection of Circulating Microparticles by Flow Cytometry: Influence of Centrifugation, Filtration of Buffer, and Freezing. Vasc. Health Risk Manag. 2010, 6, 1125–1133. [Google Scholar] [CrossRef] [Green Version]
- van Ierssel, S.H.; Van Craenenbroeck, E.M.; Conraads, V.M.; Van Tendeloo, V.F.; Vrints, C.J.; Jorens, P.G.; Hoymans, V.Y. Flow Cytometric Detection of Endothelial Microparticles (EMP): Effects of Centrifugation and Storage Alter with the Phenotype Studied. Thromb. Res. 2010, 125, 332–339. [Google Scholar] [CrossRef]
- Bratseth, V.; Margeirsdottir, H.D.; Chiva-Blanch, G.; Heier, M.; Solheim, S.; Arnesen, H.; Dahl-Jørgensen, K.; Seljeflot, I. Annexin V+ Microvesicles in Children and Adolescents with Type 1 Diabetes: A Prospective Cohort Study. J. Diabetes Res. 2020, 2020, 7216863. [Google Scholar] [CrossRef] [Green Version]
- Bratseth, V.; Chiva-Blanch, G.; Byrkjeland, R.; Solheim, S.; Arnesen, H.; Seljeflot, I. Elevated Levels of Circulating Microvesicles in Coronary Artery Disease Patients with Type 2 Diabetes and Albuminuria: Effects of Exercise Training. Diabetes Vasc. Dis. Res. 2019, 16, 431–439. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, I.B.; Hall, I.R.; Maccallum, H.; Mackenzie, I.S.; Mceniery, C.M.; van der Arend, B.J.; Shu, Y.; Mackay, L.S.; Webb, D.J.; Cockcroft, J.R. Pulse-Wave Analysis: Clinical Evaluation of a Noninvasive, Widely Applicable Method for Assessing Endothelial Function. Arterioscler. Thromb. Vasc. Biol. 2002, 22, 147–152. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, N.N.I.N.; Rasool, A.H.G. Assessment of Macrovascular Endothelial Function Using Pulse Wave Analysis and Its Association with Microvascular Reactivity in Healthy Subjects. Ski. Res. Technol. 2017, 23, 321–325. [Google Scholar] [CrossRef]
- Greig, L.D.; Leslie, S.J.; Gibb, F.W.; Tan, S.; Newby, D.E.; Webb, D.J. Comparative Effects of Glyceryl Trinitrate and Amyl Nitrite on Pulse Wave Reflection and Augmentation Index. Br. J. Clin. Pharmacol. 2005, 59, 265–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibrahim, N.N.I.N.; Rasool, A.H.G.; Wong, A.R.; Rahman, A.R.A. Methods Optimization to Assess Endothelial Function in Females- Duration of Glyceryl Trinitrate Effect. Methods Find. Exp. Clin. Pharmacol. 2007, 29, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, H.O.; Bayazeed, B.; Hook, G.; Johnson, A.; Cronin, J.; Baron, A.D. Endothelial Dysfunction Is Associated with Cholesterol Levels in the High Normal Range in Humans. Circulation 1997, 96, 3287–3293. [Google Scholar] [CrossRef]
- Torella, D.; Ellison, G.M.; Torella, M.; Vicinanza, C.; Aquila, I.; Iaconetti, C.; Scalise, M.; Marino, F.; Henning, B.J.; Lewis, F.C.; et al. Carbonic Anhydrase Activation Is Associated with Worsened Pathological Remodeling in Human Ischemic Diabetic Cardiomyopathy. J. Am. Heart Assoc. 2014, 3, e000434. [Google Scholar] [CrossRef] [Green Version]
- Esposito, K.; Ciotola, M.; Sasso, F.C.; Cozzolino, D.; Saccomanno, F.; Assaloni, R.; Ceriello, A.; Giugliano, D. Effect of a Single High-Fat Meal on Endothelial Function in Patients with the Metabolic Syndrome: Role of Tumor Necrosis Factor-α. Nutr. Metab. Cardiovasc. Dis. 2007, 17, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Suades, R.; Padró, T.; Alonso, R.; Mata, P.; Badimon, L. Lipid-Lowering Therapy with Statins Reduces Microparticle Shedding from Endothelium, Platelets and Inflammatory Cells. Thromb. Haemost. 2013, 110, 366–377. [Google Scholar] [CrossRef] [Green Version]
- Lacroix, R.; Robert, S.; Poncelet, P.; Kasthuri, R.S.; Key, N.S.; Dignat-George, F. Standardization of Platelet-Derived Microparticle Enumeration by Flow Cytometry with Calibrated Beads: Results of the International Society on Thrombosis and Haemostasis SSC Collaborative Workshop. J. Thromb. Haemost. 2010, 8, 2571–2574. [Google Scholar] [CrossRef]
- Dignat-George, F.; Boulanger, C.M. The Many Faces of Endothelial Microparticles. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 27–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dignat-George, F. Extracellular Vesicles: Overview and Clinical Implications. Blood 2018, 132, SCI-25. [Google Scholar] [CrossRef]
- Ståhl, A.L.; Johansson, K.; Mossberg, M.; Kahn, R.; Karpman, D. Exosomes and Microvesicles in Normal Physiology, Pathophysiology, and Renal Diseases. Pediatr. Nephrol. 2019, 34, 11–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, R.; Huang, X.; Brekken, R.A.; Schroit, A.J. Detection of Phosphatidylserine-Positive Exosomes for the Diagnosis of Early-Stage Malignancies. Br. J. Cancer 2017, 117, 545–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, D.B.; Thuy Ly, T.B.; Wesseling, M.C.; Hittinger, M.; Torge, A.; Devitt, A.; Perrie, Y.; Bernhardt, I. Characterization of Microvesicles Released from Human Red Blood Cells. Cell. Physiol. Biochem. 2016, 38, 1085–1099. [Google Scholar] [CrossRef]
- Brodsky, S.V.; Zhang, F.; Nasjletti, A.; Goligorsky, M.S. Endothelium-Derived Microparticles Impair Endothelial Function In Vitro. Am. J. Physiol. Heart Circ. Physiol. 2004, 286, 1910–1915. [Google Scholar] [CrossRef] [Green Version]
- Pirro, M.; Schillaci, G.; Paltriccia, R.; Bagaglia, F.; Menecali, C.; Mannarino, M.R.; Capanni, M.; Velardi, A.; Mannarino, E. Increased Ratio of CD31+/CD42− Microparticles to Endothelial Progenitors as a Novel Marker of Atherosclerosis in Hypercholesterolemia. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 2530–2535. [Google Scholar] [CrossRef] [Green Version]
- Northrop, E.F.; Milbauer, L.C.; Rudser, K.D.; Fox, C.K.; Solovey, A.N.; Kaizer, A.M.; Hebbel, R.P.; Kelly, A.S.; Ryder, J.R. Reproducibility of Endothelial Microparticles in Children and Adolescents. Biomark. Med. 2019, 14, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Pfrieger, F.W.; Vitale, N. Cholesterol and the Journey of Extracellular Vesicles. J. Lipid Res. 2018, 59, 2255–2261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, Y.; Luo, N.; Lopes-Virella, M.F. Oxidized LDL Induces the Expression of ALBP/AP2 MRNA and Protein in Human THP-1 Macrophages. J. Lipid Res. 2000, 41, 2017–2023. [Google Scholar] [CrossRef]
- Nomura, S.; Shouzu, A.; Omoto, S.; Nishikawa, M.; Iwasaka, T. Effects of Losartan and Simvastatin on Monocyte-Derived Microparticles in Hypertensive Patients with and Without Type 2 Diabetes Mellitus. Clin. Appl. Thromb. 2004, 10, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Chiva-Blanch, G.; Badimon, L. Cross-Talk between Lipoproteins and Inflammation: The Role of Microvesicles. J. Clin. Med. 2019, 8, 2059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerrero, F.; Carmona, A.; Obrero, T.; Jiménez, M.J.; Soriano, S.; Moreno, J.A.; Martín-Malo, A.; Aljama, P. Role of Endothelial Microvesicles Released by P-Cresol on Endothelial Dysfunction. Sci. Rep. 2020, 10, 10657. [Google Scholar] [CrossRef] [PubMed]
- Marei, I.; Chidiac, O.; Thomas, B.; Pasquier, J.; Dargham, S.; Robay, A.; Vakayil, M.; Jameesh, M.; Triggle, C.; Rafii, A.; et al. Angiogenic Content of Microparticles in Patients with Diabetes and Coronary Artery Disease Predicts Networks of Endothelial Dysfunction. Cardiovasc. Diabetol. 2022, 21, 17. [Google Scholar] [CrossRef] [PubMed]
- Venable, A.S.; Williams, R.R.; Haviland, D.L.; McFarlin, B.K. An Analysis of Endothelial Microparticles as a Function of Cell Surface Antibodies and Centrifugation Techniques. J. Immunol. Methods 2014, 406, 117–123. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Hypercholesterolaemia (n = 44) | Control (n = 44) | p Value |
|---|---|---|---|
| Mean (SD) | Mean (SD) | ||
| Age, y | 43.48 (7.76) | 42.30 (6.63) | 0.45 a |
| Male/female, n(%)/n(%) | 15 (51.7)/29 (49.2) | 14 (48.3)/30 (50.8) | 0.82 b |
| Smoker, n(%) | 4 (9.1%) | 1 (2.3%) | 0.36 c |
| Hypertension, n(%) | 2 (4.5%) | 1 (2.3%) | 0.50 c |
| BMI, kg/m2 | 27.63 (4.16) | 25.99 (4.96) | 0.10 a |
| LDL, mmol/L | 4.66 (0.56) | 2.99 (0.51) | <0.001 a |
| HDL, mmol/L | 1.42 (0.29) | 1.40 (0.33) | 0.73 a |
| Triglyceride, mmol/L | 1.39 (0.50) | 1.15 (0.59) | 0.04 a |
| Total Cholesterol, mmol/L | 6.64 (0.74) | 4.83 (0.82) | <0.001 a |
| SBP, mmHg | 122.90 (13.18) | 119.26 (13.18) | 0.18 a |
| DBP, mmHg | 76.57 (7.94) | 74.91 (10.41) | 0.40 a |
| EIDV, % | 13.43 (3.75) | 14.59 (4.61) | 0.22 a |
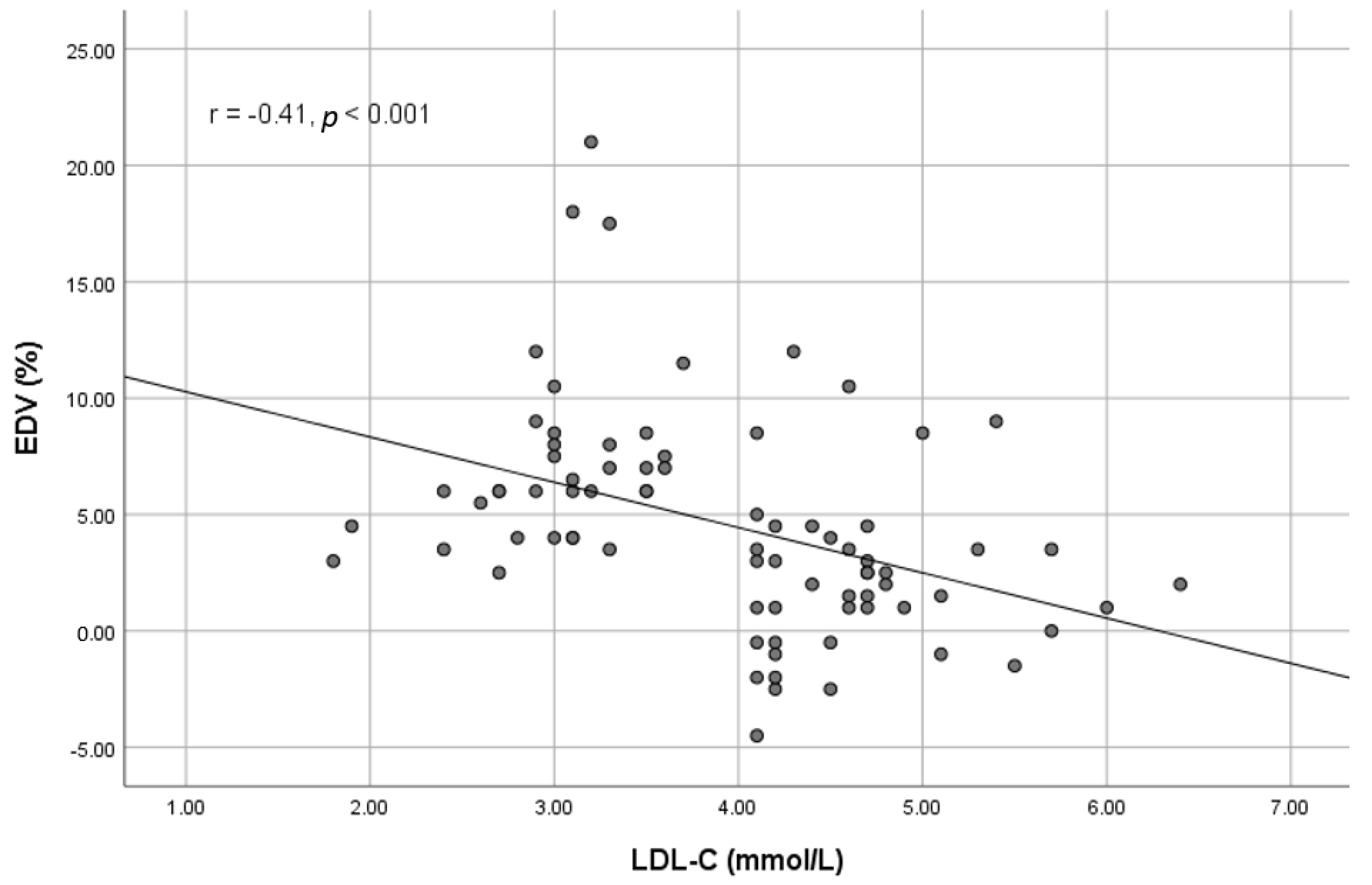
| EDV, % | 2.26 (3.48) | 7.47 (4.21) | <0.001 a |
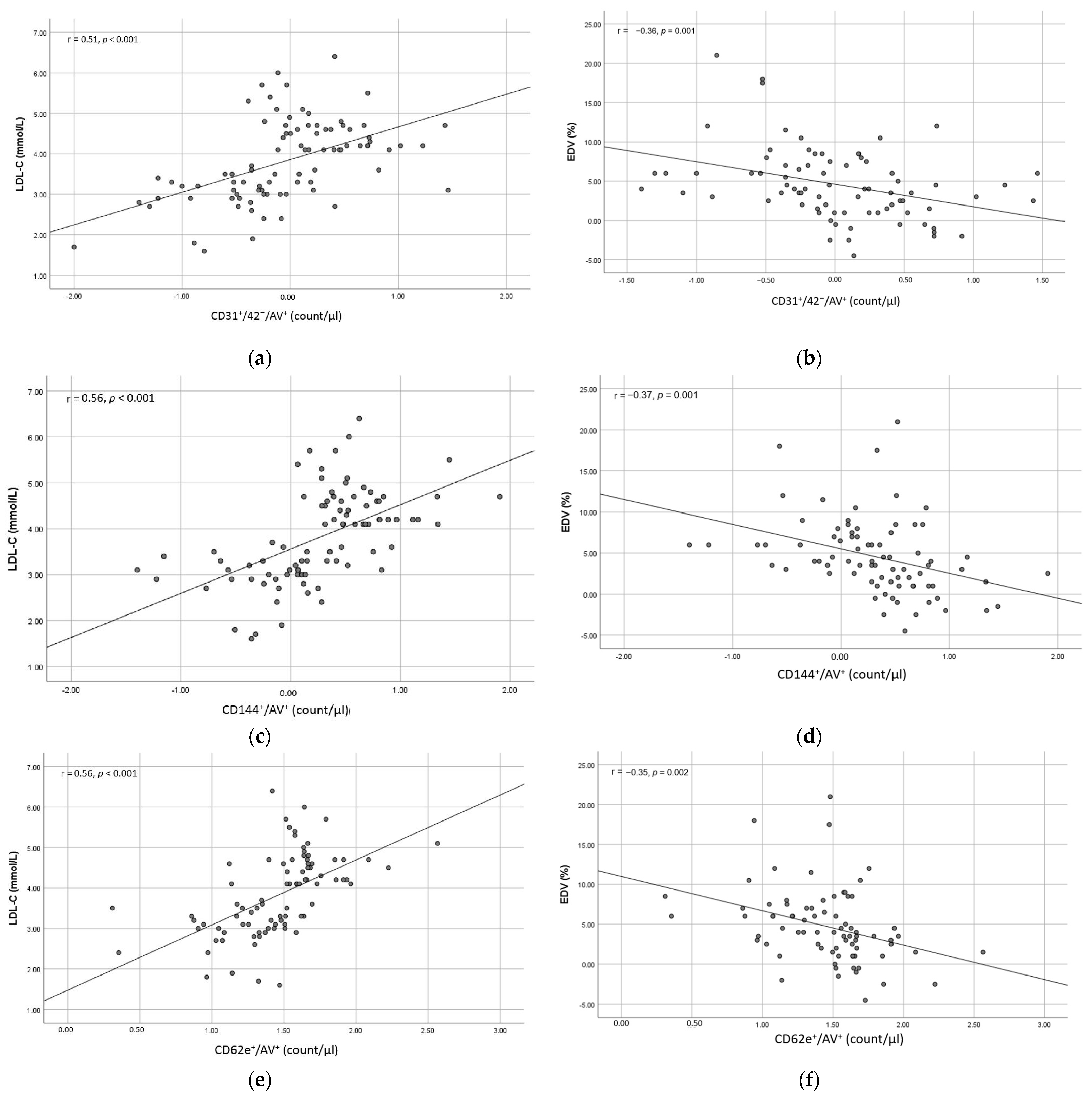
| CD31+/42−/AV+, count/µL | 3.45 (4.74) | 1.33 (4.40) | 0.03 a |
| CD144+/AV+, count/µL | 7.37 (12.66) | 1.42 (1.71) | 0.003 a |
| CD62e+/AV+, count/µL | 57.16 (56.22) | 20.78 (11.04) | <0.001 a |
| Group | Mean (SD) | Mean Difference (95% CI) | p Value | |
|---|---|---|---|---|
| Hypercholesterolaemia (n = 44) | Control (n = 44) | |||
| CD31+/42−/AV+ | 3.45 (4.74) a | 1.33 (4.40) a | −2.12 (−4.06, −0.18) | 0.032 b |
| CD31+/42−/AV+ (adjusted) | 3.41 (2.01, 4.81) | 1.38 (−0.02, 2.78) | 2.03 (0.03, 4.03) c | 0.047 d |
| CD144+/AV+ | 7.37 (12.66) a | 1.42 (1.71) a | −5.96 (−9.79, −2.13) | 0.003 |
| CD144+/AV+ (adjusted) | 7.38 (4.62, 10.14) | 1.41 (−1.35, 4.17) | 5.96 (2.02, 9.91) c | 0.003 d |
| CD62e+/AV+ | 57.16 (56.22) a | 20.78 (11.04) a | 36.38 (−53.56, −19.20) | <0.001 |
| CD62e+/AV+ (adjusted) | 86.62 (69.05, 104.19) | 59.61 (42.24, 76.97) | 27.01 (2.00, 52.03) c | 0.035 d |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nik Ibrahim, N.N.I.; Abdul Rahman, R.; Azlan, M.; Abd Aziz, A.; Ghulam Rasool, A.H. Endothelial Microparticles as Potential Biomarkers in the Assessment of Endothelial Dysfunction in Hypercholesterolemia. Medicina 2022, 58, 824. https://doi.org/10.3390/medicina58060824
Nik Ibrahim NNI, Abdul Rahman R, Azlan M, Abd Aziz A, Ghulam Rasool AH. Endothelial Microparticles as Potential Biomarkers in the Assessment of Endothelial Dysfunction in Hypercholesterolemia. Medicina. 2022; 58(6):824. https://doi.org/10.3390/medicina58060824
Chicago/Turabian StyleNik Ibrahim, Nik Nor Izah, Razlina Abdul Rahman, Maryam Azlan, Aniza Abd Aziz, and Aida Hanum Ghulam Rasool. 2022. "Endothelial Microparticles as Potential Biomarkers in the Assessment of Endothelial Dysfunction in Hypercholesterolemia" Medicina 58, no. 6: 824. https://doi.org/10.3390/medicina58060824