
Efficacy of Quantitative Pupillary Light Reflex for Predicting Neurological Outcomes in Patients Treated with Targeted Temperature Management after Cardiac Arrest: A Systematic Review and Meta-Analysis

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Automated Pupillometer
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias in Individual Studies
2.6. Statistical Analysis
2.7. Outcome Measures
3. Results
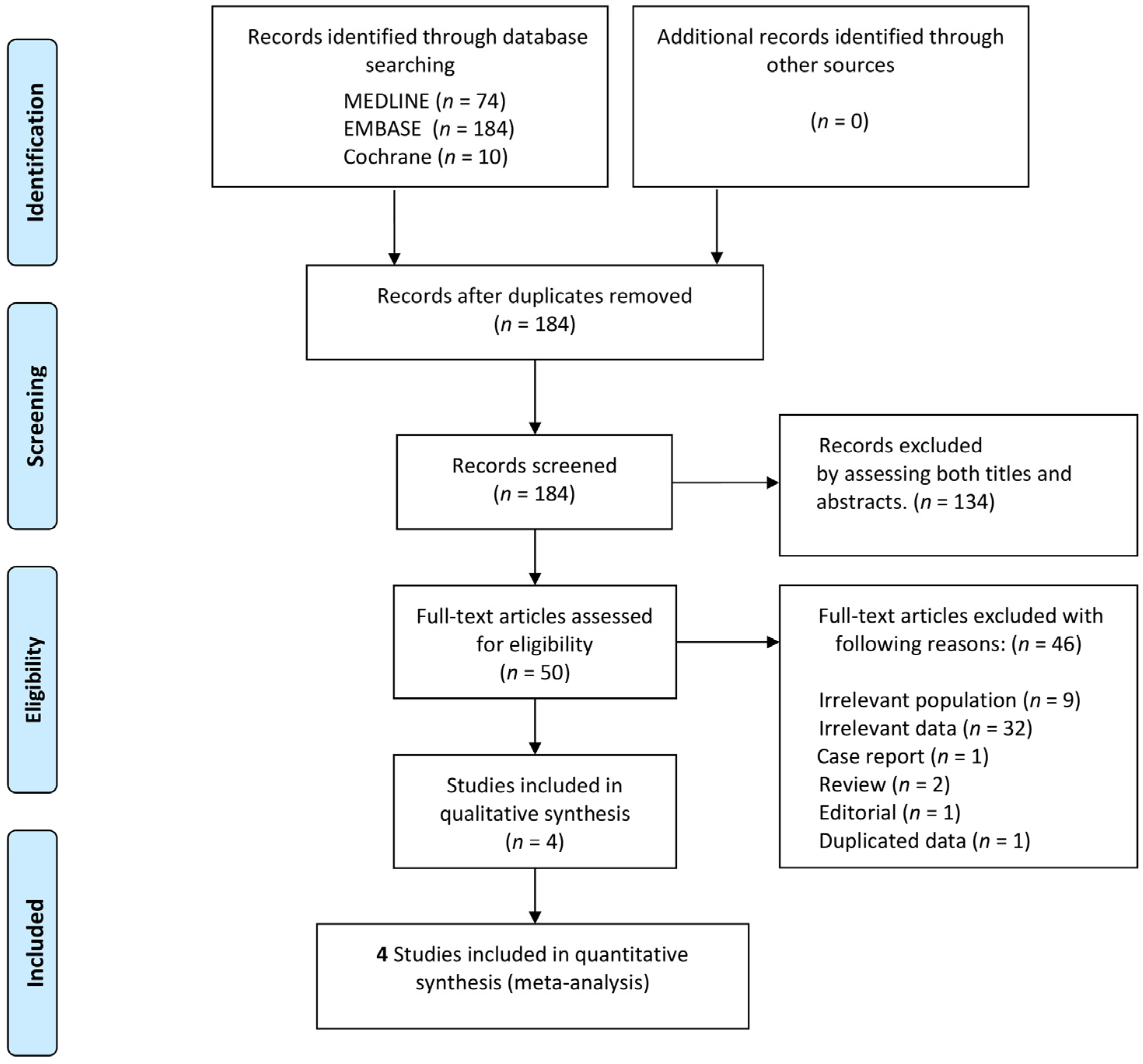
3.1. Study Selection and Characteristics of Included Studies
3.2. Quality of the Included Studies
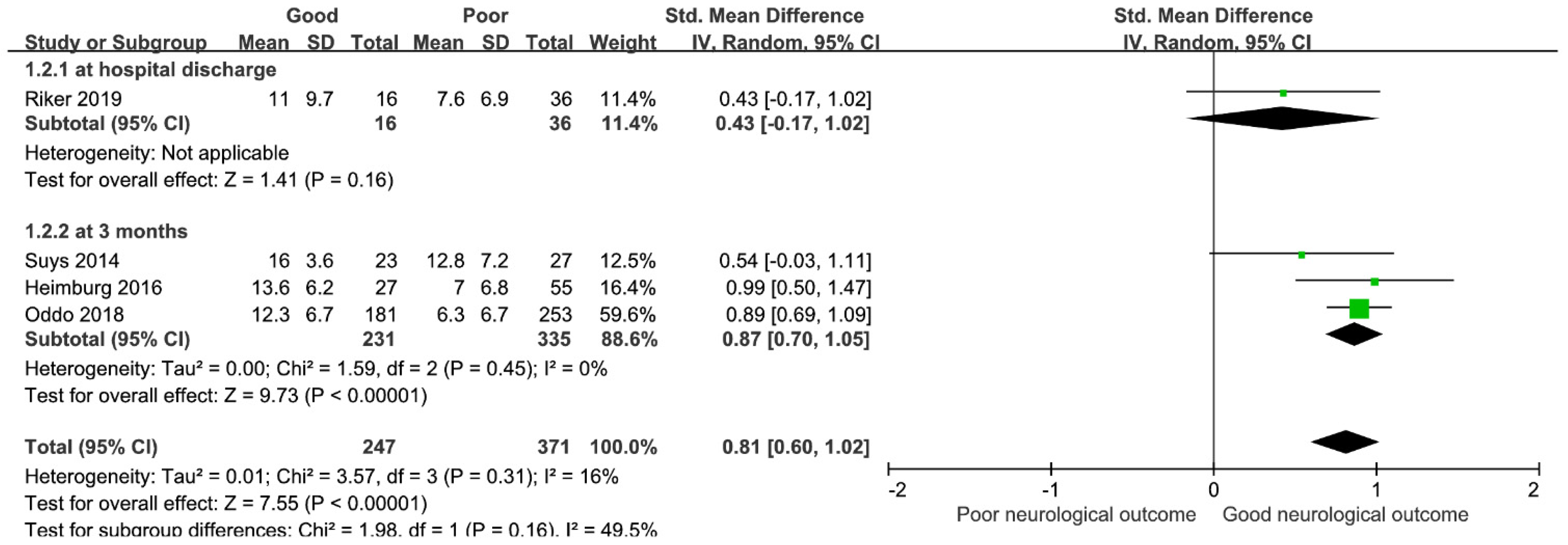
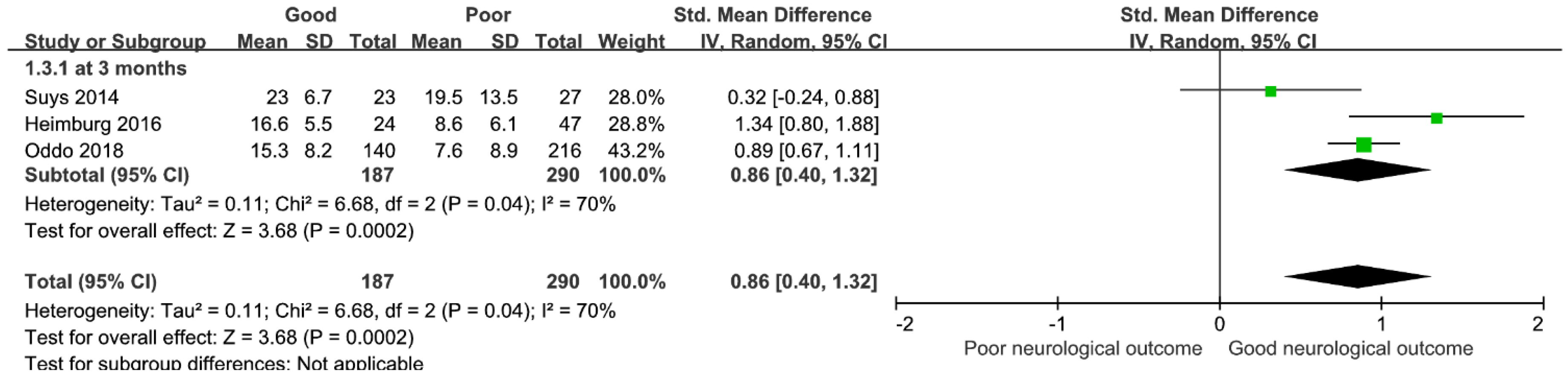
3.3. Main Analysis
3.4. Sensitivity Analysis
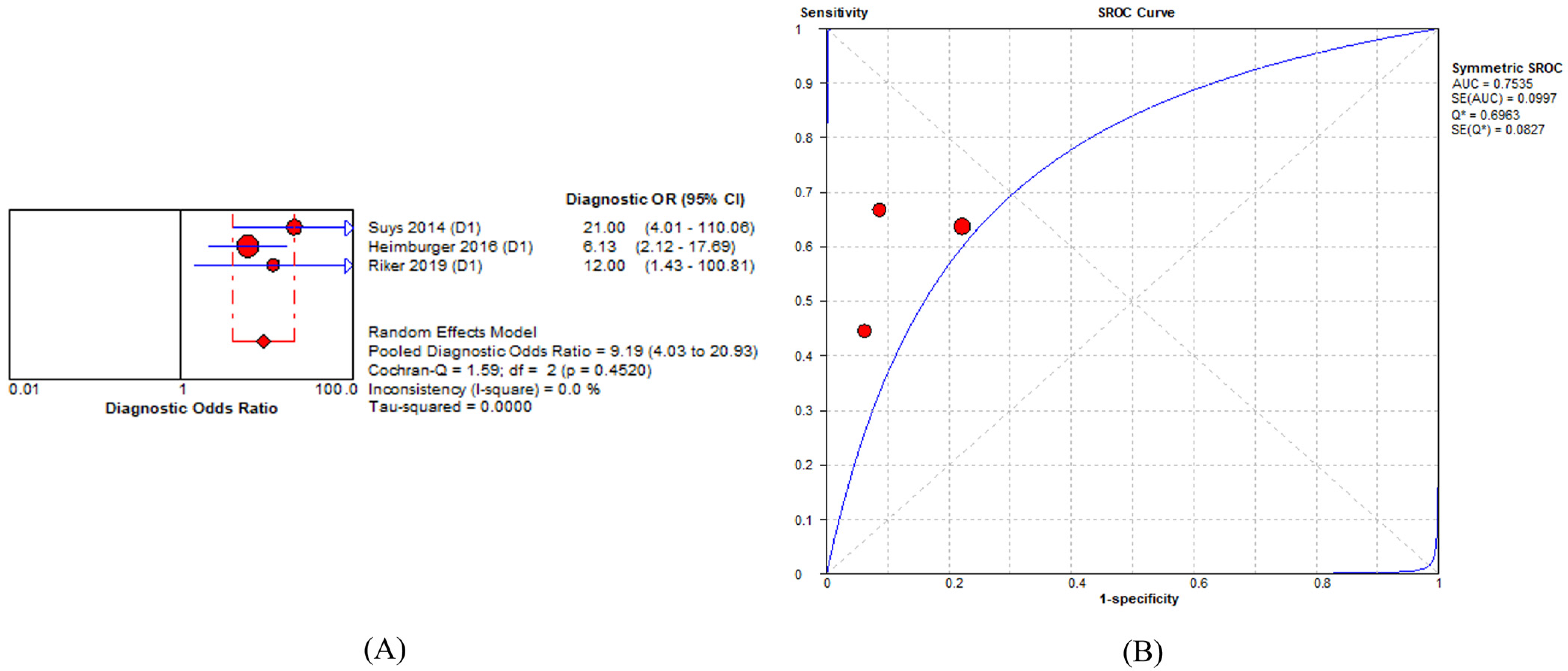
3.5. Prognostic Accuracy of Percent Constriction of Pupillary Light Reflex in Predicting Poor Neurological Outcome
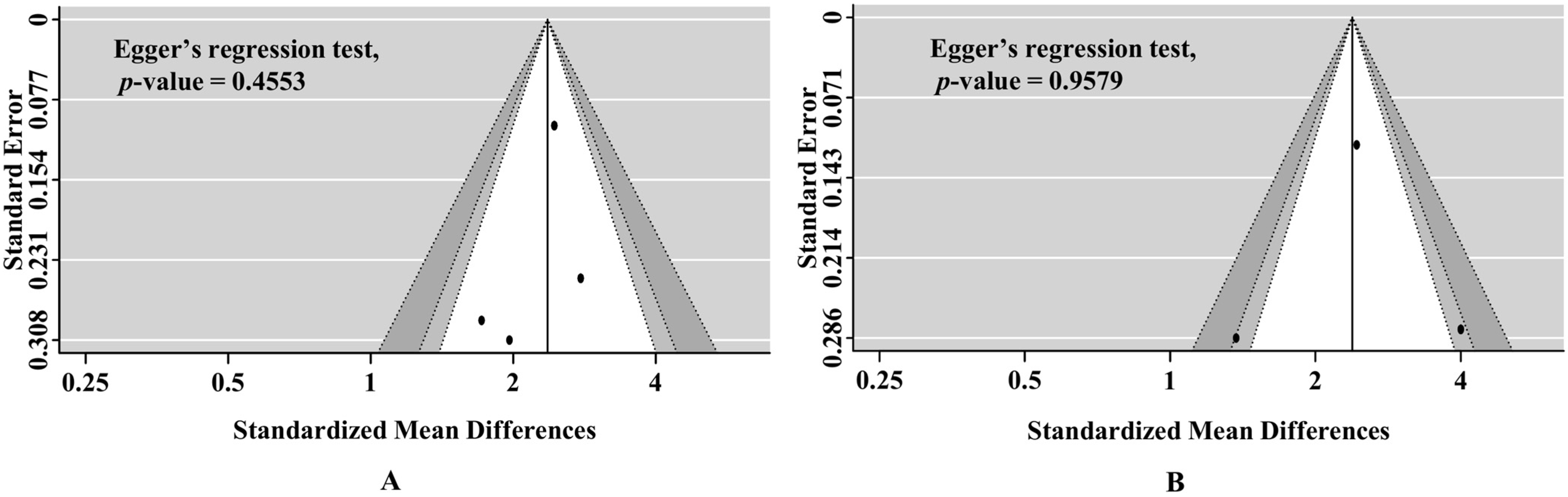
3.6. Publication Bias and Quality of Evidence According to GRADE Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Golan, E.; Barrett, K.; Alali, A.S.; Duggal, A.; Jichici, D.; Pinto, R.; Morrison, L.; Scales, D.C. Predicting neurologic outcome after targeted temperature management for cardiac arrest: Systematic review and meta-analysis. Crit. Care Med. 2014, 42, 1919–1930. [Google Scholar] [CrossRef] [PubMed]
- Greer, D.M.; Yang, J.; Scripko, P.D.; Sims, J.R.; Cash, S.; Wu, O.; Hafler, J.P.; Schoenfeld, D.A.; Furie, K.L. Clinical examination for prognostication in comatose cardiac arrest patients. Resuscitation 2013, 84, 1546–1551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamura, T.; Namiki, J.; Sugawara, Y.; Sekine, K.; Yo, K.; Kanaya, T.; Yokobori, S.; Roberts, R.; Abe, T.; Yokota, H.; et al. Quantitative assessment of pupillary light reflex for early prediction of outcomes after out-of-hospital cardiac arrest: A multicentre prospective observational study. Resuscitation 2018, 131, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Couret, D.; Boumaza, D.; Grisotto, C.; Triglia, T.; Pellegrini, L.; Ocquidant, P.; Bruder, N.J.; Velly, L.J. Reliability of standard pupillometry practice in neurocritical care: An observational, double-blinded study. Crit. Care 2016, 20, 99. [Google Scholar] [CrossRef] [Green Version]
- Du, R.; Meeker, M.; Bacchetti, P.; Larson, M.D.; Holland, M.C.; Manley, G.T. Evaluation of the portable infrared pupillometer. Neurosurgery 2005, 57, 198–203. [Google Scholar] [CrossRef]
- Olson, D.M.; Andrew Kofke, W.; O’Phelan, K.; Gupta, P.K.; Figueroa, S.A.; Smirnakis, S.M.; Leroux, P.D.; Suarez, J.I. Global monitoring in the neurocritical care unit. Neurocrit. Care 2015, 22, 337–347. [Google Scholar] [CrossRef]
- Riker, R.R.; Sawyer, M.E.; Fischman, V.G.; May, T.; Lord, C.; Eldridge, A.; Seder, D.B. Neurological Pupil Index and Pupillary Light Reflex by Pupillometry Predict Outcome Early after Cardiac Arrest. Neurocrit. Care 2019, 32, 152–161. [Google Scholar] [CrossRef]
- Chen, J.W.; Vakil-Gilani, K.; Williamson, K.L.; Cecil, S. Infrared pupillometry, the Neurological Pupil index and unilateral pupillary dilation after traumatic brain injury: Implications for treatment paradigms. SpringerPlus 2014, 3, 548. [Google Scholar] [CrossRef] [Green Version]
- Heimburger, D.; Durand, M.; Gaide-Chevronnay, L.; Dessertaine, G.; Moury, P.H.; Bouzat, P.; Albaladejo, P.; Payen, J.F. Quantitative pupillometry and transcranial Doppler measurements in patients treated with hypothermia after cardiac arrest. Resuscitation 2016, 103, 88–93. [Google Scholar] [CrossRef]
- Oddo, M.; Sandroni, C.; Citerio, G.; Miroz, J.P.; Horn, J.; Rundgren, M.; Cariou, A.; Payen, J.F.; Storm, C.; Stammet, P.; et al. Quantitative versus standard pupillary light reflex for early prognostication in comatose cardiac arrest patients: An international prospective multicenter double-blinded study. Intensive Care Med. 2018, 44, 2102–2111. [Google Scholar] [CrossRef] [Green Version]
- Suys, T.; Bouzat, P.; Marques-Vidal, P.; Sala, N.; Payen, J.F.; Rossetti, A.O.; Oddo, M. Automated quantitative pupillometry for the prognostication of coma after cardiac arrest. Neurocrit. Care 2014, 21, 300–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B.; et al. Meta-analysis of Observational Studies in EpidemiologyA Proposal for Reporting. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Cote, P.; Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Holling, H.; Böhning, W.; Böhning, D. Likelihood-based clustering of meta-analytic SROC curves. Psychometrika 2012, 77, 106–126. [Google Scholar] [CrossRef]
- Zamora, J.; Abraira, V.; Muriel, A.; Khan, K.; Coomarasamy, A. Meta-DiSc: A software for meta-analysis of test accuracy data. BMC Med. Res. Methodol. 2006, 6, 31. [Google Scholar] [CrossRef]
- Jones, C.M.; Athanasiou, T. Summary receiver operating characteristic curve analysis techniques in the evaluation of diagnostic tests. Ann. Thorac. Surg. 2005, 79, 16–20. [Google Scholar] [CrossRef]
- Na, M.K.; Kim, W.; Lim, T.H.; Jang, B.; Cho, Y.; Choi, K.S.; Shin, H.G.; Ahn, C.; Lee, J.; Kim, J.G. Gray matter to white matter ratio for predicting neurological outcomes in patients treated with target temperature management after cardiac arrest: A systematic review and meta-analysis. Resuscitation 2018, 132, 21–28. [Google Scholar] [CrossRef]
- Jorgensen, E.O.; Holm, S. The natural course of neurological recovery following cardiopulmonary resuscitation. Resuscitation 1998, 36, 111–122. [Google Scholar] [CrossRef]
- Larson, M.D.; Behrends, M. Portable infrared pupillometry: A review. Anesth. Analg. 2015, 120, 1242–1253. [Google Scholar] [CrossRef] [PubMed]
- Guldenmund, P.; Soddu, A.; Baquero, K.; Vanhaudenhuyse, A.; Bruno, M.A.; Gosseries, O.; Laureys, S.; Gómez, F. Structural brain injury in patients with disorders of consciousness: A voxel-based morphometry study. Brain Inj. 2016, 30, 343–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obinata, H.; Yokobori, S.; Shibata, Y.; Takiguchi, T.; Nakae, R.; Igarashi, Y.; Shigeta, K.; Matsumoto, H.; Aiyagari, V.; Olson, D.M.; et al. Early automated infrared pupillometry is superior to auditory brainstem response in predicting neurological outcome after cardiac arrest. Resuscitation 2020, 154, 77–84. [Google Scholar] [CrossRef]
- Larson, M.D.; Muhiudeen, I. Pupillometric analysis of the ‘absent light reflex’. Arch. Neurol. 1995, 52, 369–372. [Google Scholar] [CrossRef]
- Zhao, W.; Stutzman, S.; DaiWai, O.; Saju, C.; Wilson, M.; Aiyagari, V. Inter-device reliability of the NPi-100 pupillometer. J. Clin. Neurosci. 2016, 33, 79–82. [Google Scholar] [CrossRef]
- Chen, J.W.; Gombart, Z.J.; Rogers, S.; Gardiner, S.K.; Cecil, S.; Bullock, R.M. Pupillary reactivity as an early indicator of increased intracranial pressure: The introduction of the Neurological Pupil index. Surg. Neurol. Int. 2011, 2, 82. [Google Scholar] [CrossRef] [Green Version]
- Tamura, T.; Namiki, J.; Sugawara, Y.; Sekine, K.; Yo, K.; Kanaya, T.; Yokobori, S.; Abe, T.; Yokota, H.; Sasaki, J. Early outcome prediction with quantitative pupillary response parameters after out-of-hospital cardiac arrest: A multicenter prospective observational study. PLoS ONE 2020, 15, e0228224. [Google Scholar] [CrossRef] [Green Version]
- Solari, D.; Rossetti, A.O.; Carteron, L.; Miroz, J.P.; Novy, J.; Eckert, P.; Oddo, M. Early prediction of coma recovery after cardiac arrest with blinded pupillometry. Ann. Neurol. 2017, 81, 804–810. [Google Scholar] [CrossRef]
- Haddock, J.H.; Mercante, D.E.; Paccione, R.; Breaux, J.L.; Jolley, S.E.; Johnson, J.L.; Connolly, S.E.; deBoisblanc, B.P. Use of Digital Pupillometry to Measure Sedative Response to Propofol. Ochsner J. 2017, 17, 250–253. [Google Scholar]
- Coppler, P.J.; Elmer, J. Novel pupillary assessment in post anoxic coma. Resuscitation 2022, 176, 66–67. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.L.; Niemann, C.U.; Larson, M.D. Mechanism of pupillary reflex dilation in awake volunteers and in organ donors. Anesthesiology 2003, 99, 1281–1286. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors (Year) | Study Design | Country | Sample Size, n | CA Type | GNO, n (%) | Quantitative PLR Assessment Time | Neurological Outcome (Timepoint) |
|---|---|---|---|---|---|---|---|
| Suys (2014) | sPOS | Switzerland | 50 | All OHCA | 23(46) | 0–24 h and 24–48 h | 3 months |
| Heimburger (2016) | sPOS | France | 82 | OHCA + IHCA | 27(32.9) | 0–24 h and 24–48 h | 3 months |
| Oddo (2018) | mPOS | Switzerland | 434 | OHCA + IHCA | 181(41) | 0–24 h, 24–48 h and 48–72 h | 3 months |
| Riker (2019) | sPOS | USA | 55 | OHCA + IHCA | 16(31) | 0–24 h | Hospital discharge |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-G.; Shin, H.; Lim, T.-H.; Kim, W.; Cho, Y.; Jang, B.-H.; Choi, K.-S.; Na, M.-K.; Ahn, C.; Lee, J. Efficacy of Quantitative Pupillary Light Reflex for Predicting Neurological Outcomes in Patients Treated with Targeted Temperature Management after Cardiac Arrest: A Systematic Review and Meta-Analysis. Medicina 2022, 58, 804. https://doi.org/10.3390/medicina58060804
Kim J-G, Shin H, Lim T-H, Kim W, Cho Y, Jang B-H, Choi K-S, Na M-K, Ahn C, Lee J. Efficacy of Quantitative Pupillary Light Reflex for Predicting Neurological Outcomes in Patients Treated with Targeted Temperature Management after Cardiac Arrest: A Systematic Review and Meta-Analysis. Medicina. 2022; 58(6):804. https://doi.org/10.3390/medicina58060804
Chicago/Turabian StyleKim, Jae-Guk, Hyungoo Shin, Tae-Ho Lim, Wonhee Kim, Youngsuk Cho, Bo-Hyoung Jang, Kyu-Sun Choi, Min-Kyun Na, Chiwon Ahn, and Juncheol Lee. 2022. "Efficacy of Quantitative Pupillary Light Reflex for Predicting Neurological Outcomes in Patients Treated with Targeted Temperature Management after Cardiac Arrest: A Systematic Review and Meta-Analysis" Medicina 58, no. 6: 804. https://doi.org/10.3390/medicina58060804