
Retrospective Comparison of Laparoscopic versus Open Radical Hysterectomy for Early-Stage Cervical Cancer in a Single Tertiary Care Institution from Lithuania between 2009 and 2019



Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Subjects’ Disease and Tumor Characteristics
3.2. Characteristics of MIS and Open Surgery
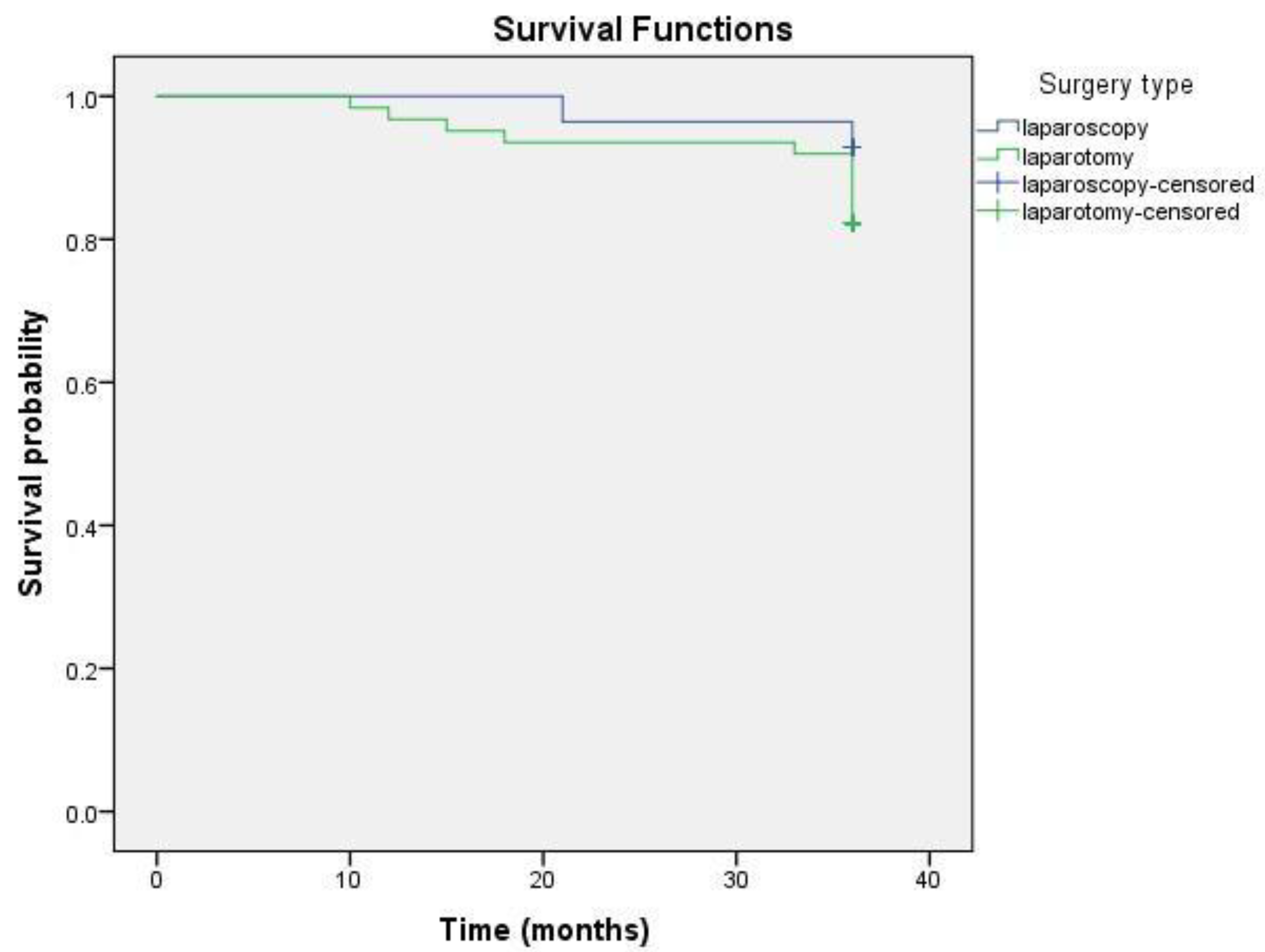
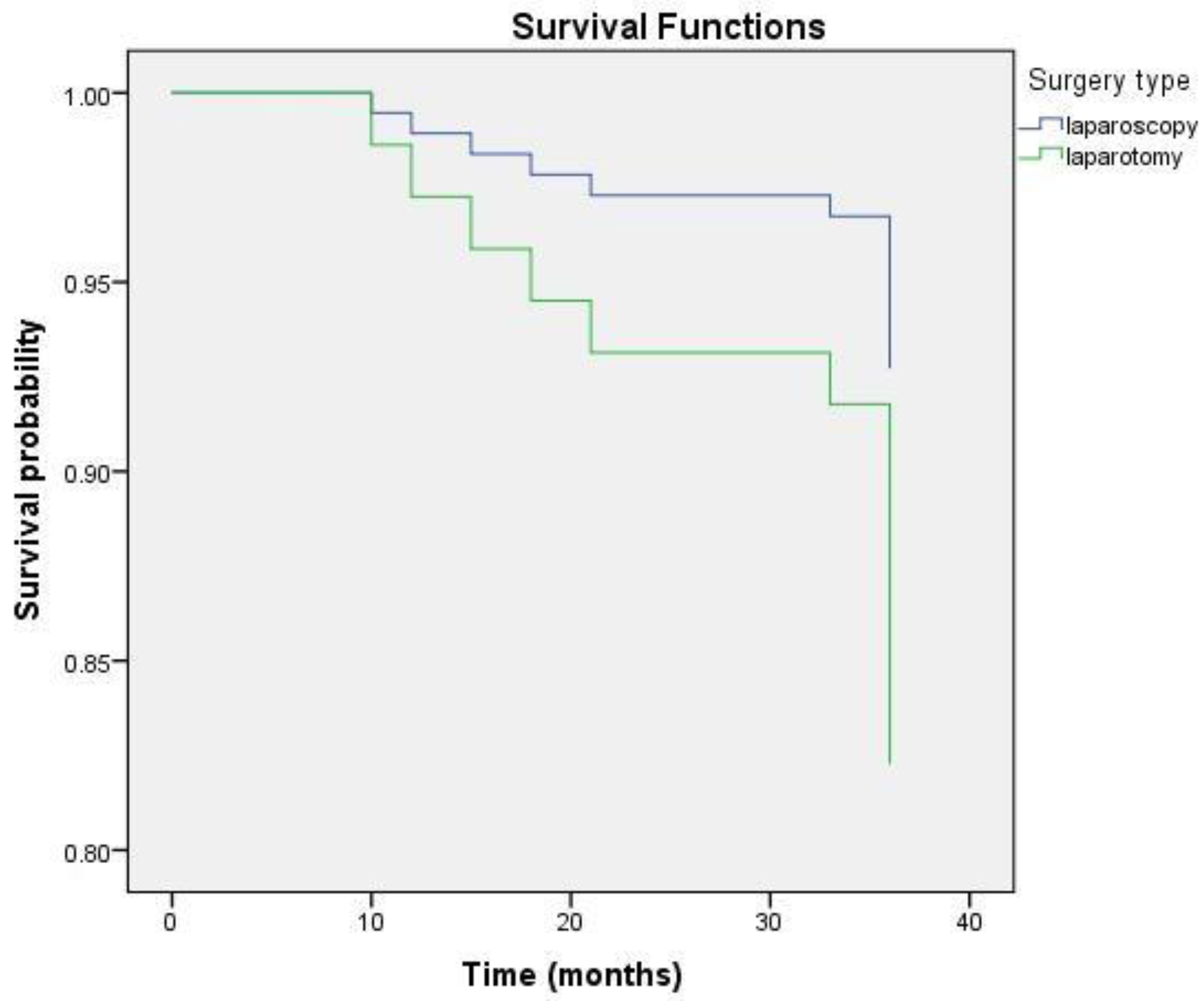
3.3. Patients’ OS Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CC | cervical cancer |
| CI | confidence intervals |
| CT | computed tomography |
| DFS | disease-free survival |
| EC | endometrial cancer |
| ESGO | European Society of Gynaecological Oncology |
| FIGO | The International Federation of Gynecology and Obstetrics |
| ICD | International Classification of Diseases |
| LACC | Laparoscopic Approach of Carcinoma of the Cervix |
| LVSI | lymphovascular space invasion |
| MIS | minimally invasive surgery |
| MRI | magnetic resonance imaging |
| NCI | National Cancer Institute |
| OR | odds ratio |
| ORH | open radical hysterectomy |
| OS | overall survival |
| PET-CT | positron emission tomography-computed tomography |
| RACC | Robot-Assisted Approach to Cervical Cancer |
| RH | radical hysterectomy |
| SEER | Surveillance, Epidemiology, and End Results |
| SGO | Society of Gynecologic Oncology |
| SUCCOR | Surgery in Cervical Cancer Comparing Different Surgical Aproaches in Stage IB1 Cervical Cancer |
References
- Zhang, S.S.; Ding, T.; Cui, Z.H.; Lv, Y.; Jiang, R.A. Efficacy of robotic radical hysterectomy for cervical cancer compared with that of open and laparoscopic surgery: A separate meta-analysis of high-quality studies. Medicine 2019, 98, e14171. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.I.; Cho, J.H.; Seol, A.; Kim, Y.I.; Lee, M.; Kim, H.S.; Chung, H.H.; Kim, J.W.; Park, N.H.; Song, Y.S. Comparison of survival outcomes between minimally invasive surgery and conventional open surgery for radical hysterectomy as primary treatment in patients with stage IB1-IIA2 cervical cancer. Gynecol. Oncol. 2019, 153, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Everatt, R.; Intaitė, B. Trends in cervical cancer mortality rates in Lithuania, 1987–2016. Cancer Epidemiol. 2018, 57, 85–89. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, K.; Park, S.J.; Lee, J.Y.; Kim, K.; Lim, M.C.; Kim, J.W. Comparative Effectiveness of Abdominal versus Laparoscopic Radical Hysterectomy for Cervical Cancer in the Postdissemination Era. Cancer Res. Treat. 2019, 51, 788–796. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, P.T.; Frumovitz, M.; Pareja, R.; Lopez, A.; Vieira, M.; Ribeiro, R.; Buda, A.; Yan, X.; Shuzhong, Y.; Chetty, N.; et al. Minimally Invasive versus Abdominal Radical Hysterectomy for Cervical Cancer. N. Engl. J. Med. 2018, 379, 1895–1904. [Google Scholar] [CrossRef]
- Bhatla, N.; Aoki, D.; Sharma, D.N.; Sankaranarayanan, R. Cancer of the cervix uteri. Int. J. Gynaecol. Obstet. 2018, 143, 22–36. [Google Scholar] [CrossRef]
- Bhatla, N.; Berek, J.S.; Fredes, M.C.; Denny, L.A.; Grenman, S.; Karunaratne, K.; Kehoe, S.T.; Konishi, I.; Olawaiye, A.B.; Prat, J.; et al. Revised FIGO staging for carcinoma of the cervix uteri. Int. J. Gynaecol. Obstet. 2019, 145, 129–135. [Google Scholar] [CrossRef]
- Melamed, A.; Margul, D.J.; Chen, L.; Keating, N.L.; Del Carmen, M.G.; Yang, J.; Seagle, B.L.; Alexander, A.; Barber, E.L.; Rice, L.W.; et al. Survival after Minimally Invasive Radical Hysterectomy for Early Stage Cervical Cancer. N. Engl. J. Med. 2018, 379, 1905–1914. [Google Scholar] [CrossRef]
- Cervical Cancer Pocket Guidelines. Available online: https://www.esgo.org/media/2015/12/ESGO_Cervical-Cancer_A6.pdf (accessed on 23 March 2018).
- Tjalma, W.A.A. The survival after a radical hysterectomy for cervical cancer by open surgery is significantly better then after minimal invasive surgery: Evidence beats gut feeling! Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 229, 195–197. [Google Scholar] [CrossRef]
- Pyeon, S.Y.; Hur, Y.J.; Lee, J.M. Rethinking the next step after unexpected results associated with minimally invasive radical hysterectomy for early cervical cancer. J. Gynecol. Oncol. 2019, 30, e43. [Google Scholar] [CrossRef]
- Kanao, H.; Aoki, Y.; Takeshima, N. Unexpected result of minimally invasive surgery for cervical cancer. J. Gynecol. Oncol. 2018, 29, e73. [Google Scholar] [CrossRef] [PubMed]
- Chiva, L.; Cibula, D.; Querleu, D. Minimally Invasive or Abdominal Radical Hysterectomy for Cervical Cancer. N. Engl. J. Med. 2019, 380, 793–794. [Google Scholar] [PubMed]
- Lee, C.L.; Huang, K.G.; Board of Directors of TAMIG. Clinical trial should be more rigorous. Taiwan J. Obstet. Gynecol. 2019, 58, 306–307. [Google Scholar] [CrossRef] [PubMed]
- Leitao, M.M. The change in landscape after a new landmark is constructed: Radical hysterectomy for early cervical cancer and minimally invasive surgery. Gynecol. Oncol. 2019, 153, 1–2. [Google Scholar] [CrossRef]
- Park, J.Y.; Nam, J.H. How should gynecologic oncologists react to the unexpected results of LACC trial? J. Gynecol. Oncol. 2018, 29, e74. [Google Scholar] [CrossRef]
- Tjalma, W.A.A. Surgical management of cervical cancer by laparoscopy or laparotomy? Gynecol. Oncol. Rep. 2018, 27, 5. [Google Scholar] [CrossRef]
- Corrado, G.; Vizza, E.; Legge, F.; Anchora, L.P.; Sperduti, I.; Fagotti, A.; Mancini, E.; Gallotta, V.; Zampa, A.; Chiofalo, B.; et al. Comparison of Different Surgical Approaches for Stage IB1 Cervical Cancer Patients: A Multi-institution Study and a Review of the Literature. Int. J. Gynecol. Cancer 2018, 28, 1020–1028. [Google Scholar] [CrossRef]
- Nam, J.H.; Park, J.Y.; Kim, D.Y.; Kim, J.H.; Kim, Y.M.; Kim, Y.T. Laparoscopic versus open radical hysterectomy in early stage cervical cancer: Long-term survival outcomes in a matched cohort study. Ann. Oncol. 2012, 23, 903–911. [Google Scholar] [CrossRef]
- Yang, L.; Cai, J.; Dong, W.; Shen, Y.; Xiong, Z.; Wang, H.; Min, J.; Li, G.; Wang, Z. Laparoscopic radical hysterectomy and pelvic lymphadenectomy can be routinely used for treatment of early stage cervical cancer: A single-institute experience with 404 patients. J. Minim. Invasive Gynecol. 2015, 22, 199–204. [Google Scholar] [CrossRef]
- Wang, W.; Chu, H.J.; Shang, C.L.; Gong, X.; Liu, T.Y.; Zhao, Y.H.; Huang, J.M.; Yao, S.Z. Long-Term Oncological Outcomes After Laparoscopic Versus Abdominal Radical Hysterectomy in Stage IA2 to IIA2 Cervical Cancer: A Matched Cohort Study. Int. J. Gynecol. Cancer 2016, 26, 1264–1273. [Google Scholar] [CrossRef]
- Wang, Y.Z.; Deng, L.; Xu, H.C.; Zhang, Y.; Liang, Z.Q. Laparoscopy versus laparotomy for the management of early stage cervical cancer. BMC Cancer 2015, 15, 928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaccarini, F.; Santy, A.; Dabi, Y.; Lavoue, V.; Carcopino, X.; Bendifallah, S.; Benbara, A.; Collinet, P.; Canlorbe, G.; Raimond, E.; et al. Comparison of survival outcomes between laparoscopic and abdominal radical hysterectomy for early stage cervical cancer: A French multicentric study. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 102046. [Google Scholar] [CrossRef] [PubMed]
- Basaran, D.; Leitao, M.M. The Landmark Series: Minimally invasive surgery for cervical cancer. Ann. Surg. Oncol. 2021, 28, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, J.; Rauh-Hain, J.A.; Saenz, J.; Isla, D.O.; Pereira, G.J.R.; Odetto, D.; Martinelli, F.; Villoslada, V.; Zapardiel, I.; Trujillo, L.M.; et al. Oncological outcomes of laparoscopic radical hysterectomy versus radical abdominal hysterectomy in patients with early stage cervical cancer: A multicenter analysis. Int. J. Gynecol. Cancer 2021, 31, 504–511. [Google Scholar] [CrossRef]
- Ceccaroni, M.; Roviglione, G.; Malzoni, M.; Cosentino, F.; Spagnolo, E.; Clarizia, R.; Casadio, P.; Seracchioli, R.; Ghezzi, F.; Mautone, D.; et al. Total laparoscopic vs. conventional open abdominal nerve-sparing radical hysterectomy: Clinical, surgical, oncological and functional outcomes in 301 patients with cervical cancer. J. Gynecol. Oncol. 2021, 32, e10. [Google Scholar] [CrossRef]
- Smith, A.J.B.; Jones, T.N.; Miao, D.; Fader, A.N. Minimally invasive radical hysterectomy for cervical cancer: A systematic review and meta-analysis. J. Minim. Invasive Gynecol. 2021, 28, 544–555.e7. [Google Scholar] [CrossRef]
- Chen, C.; Fang, Z.; Wang, Q.; Li, W.; Li, P.; Wang, L.; Kang, S.; Zhu, B.; Lin, Z.; Wang, X.; et al. Comparative study on the oncological prognosis of laparoscopy and laparotomy for stage IIA1 cervical squamous cell carcinoma. Eur. J. Surg. Oncol. 2021, 47, 346–352. [Google Scholar] [CrossRef]
- Li, P.; Chen, L.; Ni, Y.; Liu, J.; Li, D.; Guo, J.; Liu, Z.; Jin, S.; Xu, Y.; Li, Z.; et al. Comparison between laparoscopic and abdominal radical hysterectomy for stage IB1 and tumor size <2 cm cervical cancer with visible or invisible tumors: A multicentre retrospective study. J. Gynecol. Oncol. 2021, 32, e17. [Google Scholar] [CrossRef]
- Naumann, R.W. Minimally invasive radical hysterectomy has many benefits compared with open radical hysterectomy: Will the LACC trial cause the premature demise of this procedure? J. Minim. Invasive Gynecol. 2019, 26, 379–380. [Google Scholar] [CrossRef]
- Martin-Hirsch, P.; Wood, N.; Whitham, N.L.; Macdonald, R.; Kirwan, J.; Anagnostopoulos, A.; Hutson, R.; Theophilou, G.; Otify, M.; Smith, M.; et al. Survival of women with early stage cervical cancer in the UK treated with minimal access and open surgery. BJOG 2019, 126, 956–959. [Google Scholar] [CrossRef] [Green Version]
- Park, J.Y.; Kim, D.; Suh, D.S.; Kim, J.H.; Kim, Y.M.; Kim, Y.T.; Nam, J.H. The Role of Laparoscopic Radical Hysterectomy in Early Stage Adenocarcinoma of the Uterine Cervix. Ann. Surg. Oncol. 2016, 23, 825–833. [Google Scholar] [CrossRef] [PubMed]
- Tinelli, A.; Perrone, A.; Gustapane, S.; Pavone, G.; Giacci, F.; Malvasi, A.; Perrone, E.; Eliseeva, M.; Medvedev, M.; Mynbaev, O. Endoscopic surgical procedures for cervical cancer treatment: A literature review. In Cervical, Breast and Prostate Cancer; iConcept Press Ltd.: Phoenix, AZ, USA, 2013. [Google Scholar]
- Gil-Moreno, A.; Carbonell-Socias, M.; Salicrú, S.; Centeno-Mediavilla, C.; Franco-Camp, S.; Colas, E.; Oaknin, A.; Pérez-Benavente, A.; Díaz-Feijoo, B. Radical Hysterectomy: Efficacy and Safety in the Dawn of Minimally Invasive Techniques. J. Minim. Invasive Gynecol. 2019, 26, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Lago, V.; Tiermes, M.; Padilla-Iserte, P.; Matute, L.; Gurrea, M.; Domingo, S. Protective maneuver to avoid tumor spillage during laparoscopic radical hysterectomy: Vaginal cuff closure. J. Minim. Invasive Gynecol. 2021, 28, 174–175. [Google Scholar] [CrossRef] [PubMed]
- Marcos-Sanmartín, J.; López Fernández, J.A.; Sánchez-Payá, J.; Piñero-Sánchez, Ó.C.; Román-Sánchez, M.J.; Quijada-Cazorla, M.A.; Candela-Hidalgo, M.A.; Martínez-Escoriza, J.C. Does the Type of Surgical Approach and the Use of Uterine Manipulators Influence the Disease-Free Survival and Recurrence Rates in Early Stage Endometrial Cancer? Int. J. Gynecol. Cancer 2016, 26, 1722–1726. [Google Scholar] [CrossRef]
- Uccella, S.; Bonzini, M.; Malzoni, M.; Fanfani, F.; Palomba, S.; Aletti, G.; Corrado, G.; Ceccaroni, M.; Seracchioli, R.; Shakir, F.; et al. The effect of a uterine manipulator on the recurrence and mortality of endometrial cancer: A multi-centric study by the Italian Society of Gynecological Endoscopy. Am. J. Obstet. Gynecol. 2017, 216, 592.e1–592.e11. [Google Scholar] [CrossRef]
- Rakowski, J.A.; Tran, T.A.; Ahmad, S.; James, J.A.; Brudie, L.A.; Pernicone, P.J.; Radi, M.J.; Holloway, R.W. Does a uterine manipulator affect cervical cancer pathology or identification of lymphovascular space involvement? Gynecol. Oncol. 2012, 127, 98–101. [Google Scholar] [CrossRef]
- Kavallaris, A.; Chalvatzas, N.; Gkoutzioulis, A.; Zygouris, D. Laparoscopic nerve-sparing radical hysterectomy without uterine manipulator for cervical cancer stage IB: Description of the technique, our experience and results after the era of LACC trial. Arch. Gynecol. Obstet. 2021, 303, 1039–1047. [Google Scholar] [CrossRef]
- Kim, S.; Min, K.J.; Lee, S.; Hong, J.H.; Song, J.Y.; Lee, J.K.; Lee, N.W. Learning curve could affect oncologic outcome of minimally invasive radical hysterectomy for cervical cancer. Asian J. Surg. 2021, 44, 174–180. [Google Scholar] [CrossRef]
- Falconer, H. The impact of surgical learning curve on survival—Reopening the door for minimally invasive surgery in the management of cervical cancer? BJOG 2021, 128, 572. [Google Scholar] [CrossRef]
- Chong, G.O.; Park, N.; Hong, D.G.; Cho, Y.L.; Park, I.S.; Lee, Y.S. Learning curve of laparoscopic radical hysterectomy with pelvic and/or para-aortic lymphadenectomy in the early and locally advanced cervical cancer: Comparison of the first 50 and second 50 cases. Int. J. Gynecol. Cancer 2009, 19, 1459–1464. [Google Scholar] [CrossRef]
- Reade, C.; Hauspy, J.; Schmuck, M.L.; Moens, F. Characterizing the learning curve for laparoscopic radical hysterectomy: Buddy operating as a technique for accelerating skill acquisition. Int. J. Gynecol. Cancer 2011, 21, 930–935. [Google Scholar] [CrossRef] [PubMed]
- Kimmig, R.; Ind, T. Minimally invasive surgery for cervical cancer: Consequences for treatment after LACC study. J. Gynecol. Oncol. 2018, 29, e75. [Google Scholar] [CrossRef] [PubMed]
- Cusimano, M.C.; Baxter, N.N.; Gien, L.T.; Moineddin, R.; Liu, N.; Dossa, F.; Willows, K.; Ferguson, S.E. Impact of surgical approach on oncologic outcomes in women undergoing radical hysterectomy for cervical cancer. Am. J. Obstet. Gynecol. 2019, 221, 619.e1–619.e24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, F.; Pan, L.; Li, L.; Li, D.; Mo, L. Effects of a simulated CO2 pneumoperitoneum environment on the proliferation, apoptosis, and metastasis of cervical cancer cells in vitro. Med. Sci. Monit. 2014, 20, 2497–2503. [Google Scholar]
- Kong, T.W.; Chang, S.J.; Piao, X.; Paek, J.; Lee, Y.; Lee, E.J.; Chun, M.; Ryu, H.S. Patterns of recurrence and survival after abdominal versus laparoscopic/robotic radical hysterectomy in patients with early cervical cancer. J. Obstet. Gynaecol. Res. 2016, 42, 77–86. [Google Scholar] [CrossRef]
- Son, T.; Kwon, I.G.; Hyung, W.J. Minimally invasive surgery for gastric cancer treatment: Current status and future perspectives. Gut Liver. 2014, 8, 229–236. [Google Scholar] [CrossRef]
- Keller, D.S.; Flores-Gonzalez, J.R.; Ibarra, S.; Madhoun, N.; Tahilramani, R.; Mahmood, A.; Haas, E.M. Evaluating quality across minimally invasive platforms in colorectal surgery. Surg. Endosc. 2016, 30, 2207–2216. [Google Scholar] [CrossRef]
- Leow, J.; Chung, B.; Chang, S. Mp54-09 trends in surgical approach and outcomes for radical cystectomy: A contemporary population-based analysis. J. Urol. 2017, 197, e725. [Google Scholar] [CrossRef]
- Ohlmann, C.H.; Hadaschik, B. Re: Minimally invasive versus abdominal radical hysterectomy for cervical cancer. Eur. Urol. 2019, 75, 875. [Google Scholar] [CrossRef]
- Casarin, J.; Bogani, G.; Papadia, A.; Ditto, A.; Pinelli, C.; Garzon, S.; Donadello, N.; Laganà, A.S.; Cromi, A.; Mueller, M.; et al. Preoperative conization and risk of recurrence in patients undergoing laparoscopic radical hysterectomy for early stage cervical cancer: A multicenter study. J. Minim. Invasive Gynecol. 2021, 28, 117–123. [Google Scholar] [CrossRef]
- Chiva, L.; Zanagnolo, V.; Querleu, D.; Martin-Calvo, N.; Arévalo-Serrano, J.; Căpîlna, M.E.; Fagotti, A.; Kucukmetin, A.; Mom, C.; Chakalova, G.; et al. SUCCOR study: An international European cohort observational study comparing minimally invasive surgery versus open abdominal radical hysterectomy in patients with stage IB1 cervical cancer. Int. J. Gynecol. Cancer 2020, 30, 1269–1277. [Google Scholar] [CrossRef] [PubMed]
- Monk, B.J.; Wang, J.; Im, S.; Stock, R.J.; Peters, W.A., 3rd; Liu, P.Y.; Barrett, R.J., 2nd; Berek, J.S.; Souhami, L.; Grigsby, P.W.; et al. Rethinking the use of radiation and chemotherapy after radical hysterectomy: A clinical-pathologic analysis of a Gynecologic Oncology Group/Southwest Oncology Group/Radiation Therapy Oncology Group trial. Gynecol. Oncol. 2005, 96, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Peters, W.A., 3rd; Liu, P.Y.; Barrett, R.J., 2nd; Stock, R.J.; Monk, B.J.; Berek, J.S.; Souhami, L.; Grigsby, P.; Gordon, W., Jr.; Alberts, D.S. Concurrent chemotherapy and pelvic radiation therapy compared with pelvic radiation therapy alone as adjuvant therapy after radical surgery in high-risk early stage cancer of the cervix. J. Clin. Oncol. 2000, 18, 1606–1613. [Google Scholar] [CrossRef] [PubMed]
- Sedlis, A.; Bundy, B.N.; Rotman, M.Z.; Lentz, S.S.; Muderspach, L.I.; Zaino, R.J. A randomized trial of pelvic radiation therapy versus no further therapy in selected patients with stage IB carcinoma of the cervix after radical hysterectomy and pelvic lymphadenectomy: A Gynecologic Oncology Group Study. Gynecol. Oncol. 1999, 73, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.D.; Herzog, T.J.; Neugut, A.I.; Burke, W.M.; Lu, Y.S.; Lewin, S.N.; Hershman, D.L. Comparative effectiveness of minimally invasive and abdominal radical hysterectomy for cervical cancer. Gynecol. Oncol. 2012, 127, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Odetto, D.; Puga, M.C.; Saadi, J.; Noll, F.; Perrotta, M. Minimally invasive radical hysterectomy: An analysis of oncologic outcomes from Hospital Italiano (Argentina). Int. J.Gynecol. Cancer 2019, 29, 863–868. [Google Scholar] [CrossRef]
- Friedlander, M.; Grogan, M. Guidelines for the treatment of recurrent and metastatic cervical cancer. Oncologist 2002, 7, 342–347. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Group by Operation Type | p Value | |
|---|---|---|---|
| MIS (n = 28) | Open-Surgery (n = 62) | ||
| Age (in years) | |||
| 40.07 ± 8.08 | 43.98 ± 13.07 | 0.087 |
| 39 | 41 | 0.366 | |
| Conization prior to surgery | 13 (46.4%) | 35 (56.4%) | 0.378 |
| Histopathological type of CC | 0.113 | ||
| 20 (71.4%) | 47 (75.8%) | |
| 7 (25.0%) | 7 (11.3%) | ||
| 1 (3.6%) | 3 (4.8%) | ||
| 0 (0%) | 5 (8.1%) | ||
| Radiological examination | 0.019 | ||
| 28 (100%) | 62 (100%) | |
| 1 (3.6%) | 2 (3.2%) | ||
| 0 (0%) | 3 (4.8%) | ||
| FIGO stage | 0.599 | ||
| 3 (10.7%) | 1 (1.6%) | |
| 0 (0%) | 14 (22.54%) | ||
| 25 (89.3%) | 43 (69.4%) | ||
| 0 (0%) | 4 (6.5%) | ||
| Hysterectomy type | 0.264 | ||
| 28 (100%) | 62 (100%) | |
| Tumor differentiation grade | 0.065 | ||
| 3 (10.7%) | 0 (0%) | |
| 5 (17.9%) | 18 (29.0%) | ||
| 20 (71.4%) | 44 (71%) | ||
| Tumor size | 0.086 | ||
| 4 (14.3%) | 16 (25.8%) | |
| 12 (42.9%) | 25 (40.3%) | ||
| 12 (42.9%) | 21 (33.9%) | ||
| Stromal invasion | 0.193 | ||
| 0 (0%) | 8 (12.9%) | |
| 6 (21.4%) | 14 (22.6%) | ||
| 22 (78.6%) | 40 (64.5%) | ||
| Lymphovascular space invasion | 0.453 | ||
| 9 (32.1%) | 14 (22.6%) | |
| 19 (67.9%) | 48 (77.4%) | ||
| Positive margins | 0 (0%) | 0 (0%) | 0.054 |
| Pelvis lymph nodes resected | 28 (100%) | 62 (100%) | 0.169 |
| Para-aortic lymph nodes resected | 0 (0%) | 8 (12.1%) | 0.054 |
| Median of resected lymph nodes (range) | 11 (8–25) | 19 (2–54) | <0.001 |
| Subjects with positive lymph nodes | 1 (3.6%) | 11 (17.7%) | 0.095 |
| Adjuvant therapy | 7 (25%) | 27 (43.5%) | 0.093 |
| Type of adjuvant therapy | 0.19 | ||
| 5 patients | 18 patients | |
| 1 patient | 0 patients | ||
| 1 patient | 9 patients | ||
| Characteristic | Group by Surgery Type | p Value | |
|---|---|---|---|
| MIS (n = 28) | Open Surgery (n = 62) | ||
| Operation length * | 218 min ± 39 min | 205 min ± 42 min | 0.195 |
| Length of hospitalization stay ** | 6 days (3, 16) | 10 days (6, 36) | <0.001 |
| Short-term postoperative complication | 5 (17.9%) | 16 (25.8%) | 0.205 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vasilevska, D.; Vasilevska, D.; Semczuk, A.; Rudaitis, V. Retrospective Comparison of Laparoscopic versus Open Radical Hysterectomy for Early-Stage Cervical Cancer in a Single Tertiary Care Institution from Lithuania between 2009 and 2019. Medicina 2022, 58, 553. https://doi.org/10.3390/medicina58040553
Vasilevska D, Vasilevska D, Semczuk A, Rudaitis V. Retrospective Comparison of Laparoscopic versus Open Radical Hysterectomy for Early-Stage Cervical Cancer in a Single Tertiary Care Institution from Lithuania between 2009 and 2019. Medicina. 2022; 58(4):553. https://doi.org/10.3390/medicina58040553
Chicago/Turabian StyleVasilevska, Danuta, Dominika Vasilevska, Andrzej Semczuk, and Vilius Rudaitis. 2022. "Retrospective Comparison of Laparoscopic versus Open Radical Hysterectomy for Early-Stage Cervical Cancer in a Single Tertiary Care Institution from Lithuania between 2009 and 2019" Medicina 58, no. 4: 553. https://doi.org/10.3390/medicina58040553