
Neuropsychological Disability in the Case of Natalizumab-Related Progressive Multifocal Leukoencephalopathy

 , ,
, ,
Abstract
:1. Introduction
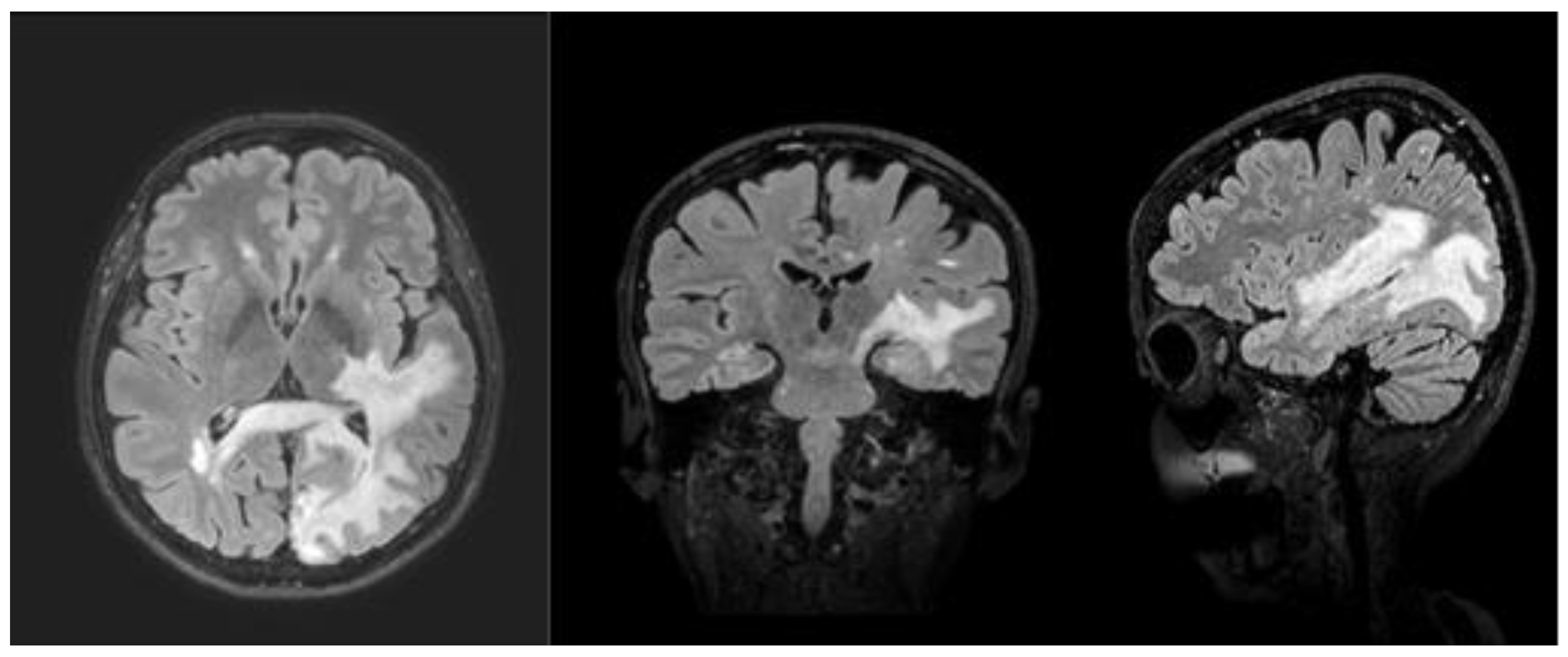
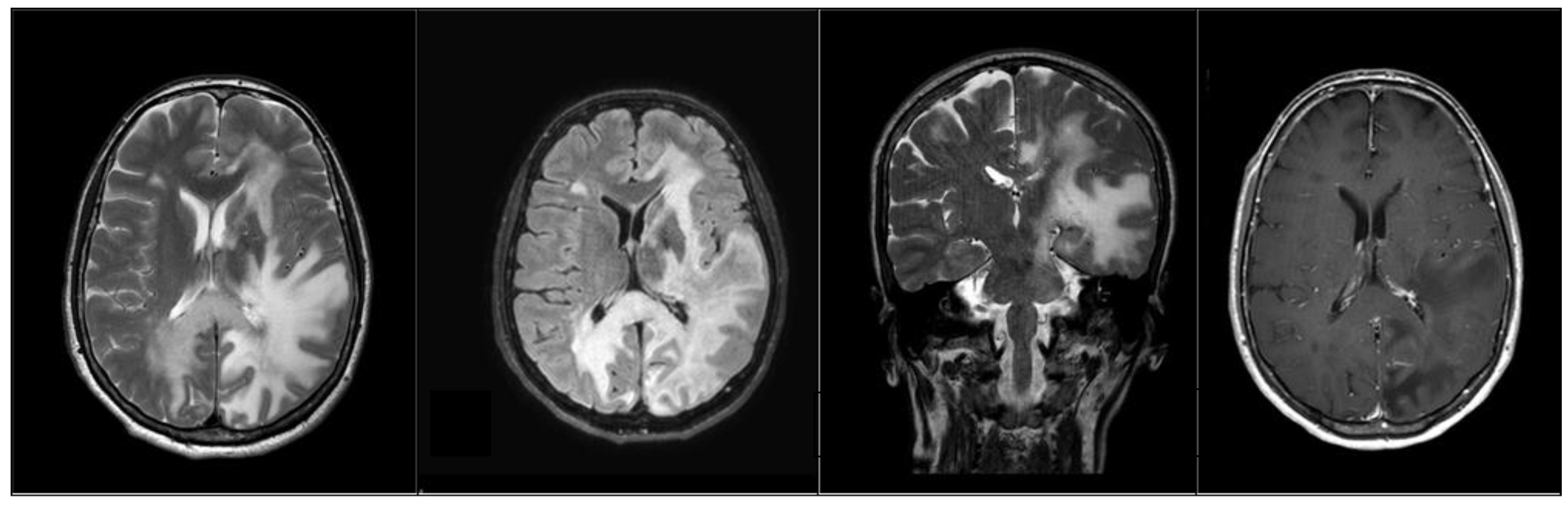
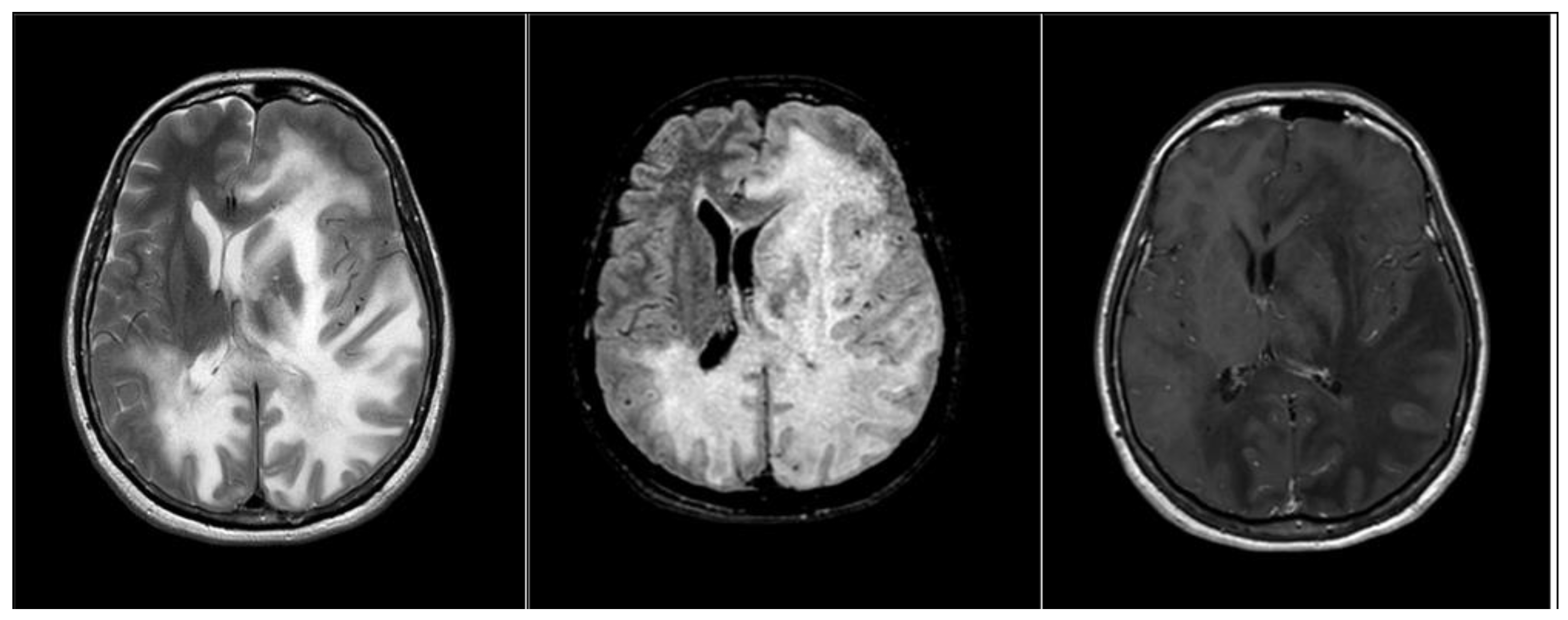
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Williamson, E.M.; Berger, J.R. Diagnosis and Treatment of Progressive Multifocal Leukoencephalopathy Associated with Multiple Sclerosis Therapies. Neurotherapeutics 2017, 14, 961–973. [Google Scholar] [CrossRef] [PubMed]
- Kleinschmidt-DeMasters, B.; Tyler, K.L. Progressive Multifocal Leukoencephalopathy Complicating Treatment with Natalizumab and Interferon Beta-1a for Multiple Sclerosis. N. Engl. J. Med. 2005, 353, 369–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, J.R.; Cree, B.A.; Greenberg, B.; Hemmer, B.; Ward, B.J.; Dong, V.M.; Merschhemke, M. Progressive multifocal leukoencephalopathy after fingolimod treatment. Neurology 2018, 90, e1815–e1821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Major, E.O.; Yousry, T.A.; Clifford, D.B. Pathogenesis of progressive multifocal leukoencephalopathy and risks associated with treatments for multiple sclerosis: A decade of lessons learned. Lancet Neurol. 2018, 17, 467–480. [Google Scholar] [CrossRef] [Green Version]
- Berger, J.R. The clinical features of PML. Clevel. Clin. J. Med. 2011, 78, S8–S12. [Google Scholar] [CrossRef]
- Ikeda, J.; Matsushima, A.; Ishii, W.; Goto, T.; Takahashi, K.; Nakamichi, K.; Saijo, M.; Sekijima, Y.; Ikeda, S.-I. Brain Biopsy Is More Reliable than the DNA test for JC Virus in Cerebrospinal Fluid for the Diagnosis of Progressive Multifocal Leukoencephalopathy. Intern. Med. 2017, 56, 1231–1234. [Google Scholar] [CrossRef] [Green Version]
- Altahan, A.M.; Berger, T.; Alorainy, I.A.; Altahan, H. Progressive Multifocal Leukoencephalopathy in the Absence of Typical Radiological Changes: Can We Make a Diagnosis? Am. J. Case Rep. 2019, 20, 101–105. [Google Scholar] [CrossRef]
- Hoepner, R.; Klotz, P.; Faissner, S.; Schneider, R.; Kinner, M.; Prehn, C.; Gold, R.; Chan, A. Neuropsychological impairment in natalizumab-associated progressive multifocal leukoencephalopathy: Implications for early diagnosis. J. Neurol. Neurosurg. Psychiatry 2015, 87, 224–226. [Google Scholar] [CrossRef]
- Dong-Si, T.; Richman, S.; Wattjes, M.P.; Wenten, M.; Gheuens, S.; Philip, J.; Datta, S.; McIninch, J.; Bozic, C.; Bloomgren, G.; et al. Outcome and survival of asymptomatic PML in natalizumab-treated MS patients. Ann. Clin. Transl. Neurol. 2014, 1, 755–764. [Google Scholar] [CrossRef]
- Scarpazza, C.; De Rossi, N.; Moiola, L.; Gerevini, S.; Cosottini, M.; Capra, R.; Mattioli, F.; Artusi, C.A. The still under-investigated role of cognitive deficits in PML diagnosis. Mult. Scler. Demyelinating Disord. 2017, 2, 255. [Google Scholar] [CrossRef] [Green Version]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, P.-R.; Koendgen, H.; Campbell, N.; Haddock, B.; Richman, S.; Chang, I. Risk of natalizumab-associated progressive multifocal leukoencephalopathy in patients with multiple sclerosis: A retrospective analysis of data from four clinical studies. Lancet Neurol. 2017, 16, 925–933. [Google Scholar] [CrossRef]
- Morales, R.P.; Garcia, M.C.; Gutierrez-Rojas, L.; Hernández, F.J.B. Progressive Multifocal Leukoencephalopathy and Immune Reconstitution Inflammatory Syndrome after Discontinuation of Fingolimod. Case Rep. Neurol. 2022, 14, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Hodel, J.; Outteryck, O.; Dubron, C.; Dutouquet, B.; Benadjaoud, M.A.; Duhin, E.; Verclytte, S.; Zins, M.; Luciani, A.; Rahmouni, A.; et al. Asymptomatic Progressive Multifocal Leukoencephalopathy Associated with Natalizumab: Diagnostic Precision with MR Imaging. Radiology 2016, 278, 863–872. [Google Scholar] [CrossRef]
- Chiaravalloti, N.D.; DeLuca, J. Cognitive impairment in multiple sclerosis. Lancet Neurol. 2008, 7, 1139–1151. [Google Scholar] [CrossRef]
- Sumowski, J.F.; Benedict, R.; Enzinger, C.; Filippi, M.; Geurts, J.J.; Hamalainen, P.; Hulst, H.; Inglese, M.; Leavitt, V.M.; Rocca, M.A.; et al. Cognition in multiple sclerosis: State of the field and priorities for the future. Neurology 2018, 90, 278–288. [Google Scholar] [CrossRef] [Green Version]
- Kinner, M.; Prehn, C.; Schneider, R.; Schroeder, C.; Kolb, E.; Goapprovd, R.; Hoepner, R.; Chan, A. Course of neuropsychological impairment during natalizumab-associated progressive multifocal leukoencephalopathy. Eur. J. Neurol. 2020, 28, 921–927. [Google Scholar] [CrossRef]
- Benedict, R.H.B.; Amato, M.P.; DeLuca, J.; Geurts, J.J.G. Cognitive impairment in multiple sclerosis: Clinical management, MRI, and therapeutic avenues. Lancet Neurol. 2020, 19, 860–871. [Google Scholar] [CrossRef]
- Clifford, D.B.; De Luca, A.; Simpson, D.M.; Arendt, G.; Giovannoni, G.; Nath, A. Natalizumab-associated progressive multifocal leukoencephalopathy in patients with multiple sclerosis: Lessons from 28 cases. Lancet Neurol. 2010, 9, 438–446. [Google Scholar] [CrossRef]
- Dahlhaus, S.; Hoepner, R.; Chan, A.; Kleiter, I.W.; Adams, O.; Lukas, C.; Hellwig, K.; Gold, R. Disease course and outcome of 15 monocentrically treated natalizumab-associated progressive multifocal leukoencephalopathy patients. J. Neurol. Neurosurg. Psychiatry 2013, 84, 1068–1074. [Google Scholar] [CrossRef] [Green Version]
- Borghi, M.; Carletto, S.; Ostacoli, L.; Scavelli, F.; Pia, L.; Pagani, M.; Bertolotto, A.; Malucchi, S.; Signori, A.; Cavallo, M. Decline of Neuropsychological Abilities in a Large Sample of Patients with Multiple Sclerosis: A Two-Year Longitudinal Study. Front. Hum. Neurosci. 2016, 10, 282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, J.R. Classifying PML risk with disease modifying therapies. Mult. Scler. Relat. Disord. 2017, 12, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Mansoor, S.; Mullane, G.; Adenan, M.H.; Kelly, S.; Water, A.; McPartland, G.; Murphy, K. Natalizumab-associated progressive multifocal leukoencephalopathy (PML) in multiple sclerosis (MS):“a case report from Ireland with review of literature, clinical pitfalls and future direction”. Egypt. J. Neurol. Psychiatry Neurosurg. 2021, 57, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Pavlovic, D.; Patera, A.C.; Nyberg, F.; Gerber, M.; Liu, M.; for the Progressive Multifocal Leukeoncephalopathy Consortium. Progressive multifocal leukoencephalopathy: Current treatment options and future perspectives. Ther. Adv. Neurol. Disord. 2015, 8, 255–273. [Google Scholar] [CrossRef] [Green Version]
- Honce, J.M.; Nagae, L.; Nyberg, E. Neuroimaging of Natalizumab Complications in Multiple Sclerosis: PML and Other Associated Entities. Mult. Scler. Int. 2015, 2015, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Patera, A.C.; Butler, S.L.; Cinque, P.; Clifford, D.B.; Elston, R.; Garcea, R.L.; Major, E.O.; Pavlovic, D.; Peterson, I.S.; Ryan, A.M.; et al. 2nd International Conference on Progressive Multifocal Leukoencephalopathy (PML) 2015: JCV virology, progressive multifocal leukoencephalopathy pathogenesis, diagnosis and risk stratification, and new approaches to prevention and treatment. J. NeuroVirology 2015, 21, 702–705. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Subtest | T0 | T1 | T2 | T3 | Cut-Off |
|---|---|---|---|---|---|
| MMSE | 30/30 | 26/30 | 13/30 | ---- | 26 |
| FAB | 18/18 | 13/18 | 6/18 | ---- | 14 |
| SRT-LTS | 64.15 | 14.96 | 1.96 | ---- | 23.3 |
| SRT-CLTR | 63.36 | 4.16 | 3.16 | ---- | 15.5 |
| SPART | 21.94 | 13.52 | 5.52 | ---- | 12.7 |
| SDMT | 83.24 | 40.44 | 11.44 | ---- | 37.9 |
| PASAT 3 | 26.49 | 8.38 | 3.38 | ---- | 28.4 |
| PASAT 2 | 33.75 | 6.56 | 2.56 | ---- | 17.1 |
| SRT-D | 8.87 | 4.28 | 4.28 | ---- | 4.9 |
| SPART-D | 9.28 | 5.18 | 2.18 | ---- | 3.6 |
| WLG | 39.88 | 6.88 | 0.88 | ---- | 17.0 |
| WCST | 20 | 62 | 101 | ---- | 90.50 |
| The Verbal Judgement Task | 56 | 40 | 18 | ---- | 33 |
| Raven’s Standard Progressive Matrices | 36 | 24 | 10 | ---- | 15 |
| HAM-D | 6 | 22 | 44 | ---- | >10 |
| HAM-A | 18 | 24 | 30 | ---- | >8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo Buono, V.; D’Aleo, G.; Cammaroto, S.; De Cola, M.C.; Palmese, F.; Smorto, C.; Marino, S.; Venuti, G.; Sessa, E.; Rifici, C.; et al. Neuropsychological Disability in the Case of Natalizumab-Related Progressive Multifocal Leukoencephalopathy. Medicina 2022, 58, 551. https://doi.org/10.3390/medicina58040551
Lo Buono V, D’Aleo G, Cammaroto S, De Cola MC, Palmese F, Smorto C, Marino S, Venuti G, Sessa E, Rifici C, et al. Neuropsychological Disability in the Case of Natalizumab-Related Progressive Multifocal Leukoencephalopathy. Medicina. 2022; 58(4):551. https://doi.org/10.3390/medicina58040551
Chicago/Turabian StyleLo Buono, Viviana, Giangaetano D’Aleo, Simona Cammaroto, Maria Cristina De Cola, Francesca Palmese, Chiara Smorto, Silvia Marino, Giuseppe Venuti, Edoardo Sessa, Carmela Rifici, and et al. 2022. "Neuropsychological Disability in the Case of Natalizumab-Related Progressive Multifocal Leukoencephalopathy" Medicina 58, no. 4: 551. https://doi.org/10.3390/medicina58040551