
Identification of Risk Factors and Development of Predictive Risk Score Model for Mortality after Open Ruptured Abdominal Aortic Aneurysm Repair

 and
and
Abstract
:1. Introduction
2. Methods
2.1. Patient Population and Study Design
2.2. Data Collection
- -
- Demographics: age and gender
- -
- Baseline comorbidities: smoking status, obesity, presence of hypertension, diabetes mellitus, previous myocardial infarction, previous myocardial revascularization, angina pectoris, heart failure (defined as ejection fraction less than 40%), chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), cerebrovascular disease (previous stroke/transient ischemic attack (TIA)), atrial fibrillation
- -
- Preoperative laboratory: blood count, renal function analysis
- -
- Clinical presentation: systolic, diastolic/mean arterial blood pressure (SAP/DAP/MAP), preoperative shock defined as MAP less than 60 mmHg lasting more than 20 min, state of consciousness, duration of symptoms onset until the surgery, presence of abdominal/lower back pain, presence of collapse, development of ventricular arrhythmia, and cardiac arrest.
- -
- Furthermore, to describe the study group, additional intraoperative and immediate postoperative data were presented as well:
- -
- RAAA parameters: maximal AAA diameter, AAA location (infrarenal, juxtarenal, pararenal, iliac artery aneurysm).
- -
- Intraoperative data: site of the proximal clamp and proximal clamping duration, type of reconstruction, total operative time, intraoperative blood loss, and number of given blood transfusion units.
- -
- Postoperative data/complications: acute kidney injury, pulmonary complications (prolonged ventilation for more than 72 h, pneumonia, atelectasis), surgical reintervention, major bleeding requiring reintervention, lower limb ischemia, stroke, acute coronary syndrome, ischemic colitis, sepsis, wound infection, wound dehiscence, abdominal compartment syndrome.
2.3. Endpoints and Statistical Analysis
3. Results
4. Discussion
5. Limitations and Strengths
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoornweg, L.L.; Storm-Versloot, M.N.; Ubbink, D.T.; Koelemay, M.L.; Legemate, D.A.; Balm, R. Meta analysis on mortality of ruptured abdominal aortic aneurysms. Eur. J. Vasc. Endovasc. Surg. 2008, 35, 558–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapma, M.R.; Dijksman, L.M.; Reimerink, J.J.; de Groof, A.J.; Zeebregts, C.J.; Wisselink, W.; Balm, R.; Dijkgraaf, M.G.; Vahl, A.C. Cost-effectiveness and cost-utility of endovascular versus open repair of ruptured abdominal aortic aneurysm in the Amsterdam Acute Aneurysm Trial. Br. J. Surg. 2014, 101, 208–215. [Google Scholar] [CrossRef]
- IMPROVE Trial Investigators; Powell, J.T.; Sweeting, M.J.; Thompson, M.M.; Ashleigh, R.; Bell, R.; Gomes, M.; Greenhalgh, R.M.; Grieve, R.; Heatley, F.; et al. Endovascular or open repair strategy for ruptured abdominal aortic aneurysm: 30 day outcomes from IMPROVE randomised trial. BMJ 2014, 348, 7661. [Google Scholar] [CrossRef] [Green Version]
- Hoornweg, L.L.; Wisselink, W.; Vahl, A.; Balm, R.; Amsterdam Acute Aneurysm Trial Collaborators. The Amsterdam Acute Aneurysm Trial: Suitability and application rate for endovascular repair of ruptured abdominal aortic aneurysms. Eur. J. Vasc. Endovasc. Surg. 2007, 33, 679–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, B.D.; Azefor, N.; Huang, C.C.; Ricotta, J.J. Trends in treatment of ruptured abdominal aortic aneurysm: Impact of endovascular repair and implications for future care. J. Am. Coll. Surg. 2013, 216, 745–754, discussion 754–755. [Google Scholar] [CrossRef] [PubMed]
- Holt, P.J.; Karthikesalingam, A.; Poloniecki, J.D.; Hinchliffe, R.J.; Loftus, I.M.; Thompson, M.M. Propensity scored analysis of outcomes after ruptured abdominal aortic aneurysm. Br. J. Surg. 2010, 97, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Reimerink, J.J.; van der Laan, M.J.; Koelemay, M.J.; Balm, R.; Legemate, D.A. Systematic review and meta-analysis of population-based mortality from ruptured abdominal aortic aneurysm. Br. J. Surg. 2013, 100, 1405–1413. [Google Scholar] [CrossRef] [PubMed]
- Acosta, S.; Ogren, M.; Bergqvist, D.; Lindblad, B.; Dencker, M.; Zdanowski, Z. The Hardman index in patients operated on for ruptured abdominal aortic aneurysm: A systematic review. J. Vasc. Surg. 2006, 44, 949–954. [Google Scholar] [CrossRef] [Green Version]
- Thompson, P.C.; Dalman, R.L.; Harris, E.J.; Chandra, V.; Lee, J.T.; Mell, M.W. Predictive models for mortality after ruptured aortic aneurysm repair do not predict futility and are not useful for clinical decision making. J. Vasc. Surg. 2016, 64, 1617–1622. [Google Scholar] [CrossRef] [Green Version]
- Wanhainen, A.; Verzini, F.; Van Herzeele, I.; Allaire, E.; Bown, M.; Cohnert, T.; Dick, F.; van Herwaarden, J.; Karkos, C.; Koelemay, M.; et al. ESVS Guidelines Committee. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-iliac Artery Aneurysms. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 8–93. [Google Scholar] [CrossRef] [Green Version]
- Markovic, M.; Tomic, I.; Ilic, N.; Dragas, M.; Koncar, I.; Bukumiric, Z.; Sladojević, M.; Davidović, L. The Rationale for Continuing Open Repair of Ruptured Abdominal Aortic Aneurysm. Ann. Vasc. Surg. 2016, 36, 64–73. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Samy, A.K.; Murray, G.; MacBain, G. Glasgow aneurysm score. Cardiovasc. Surg. 1994, 2, 41–44. [Google Scholar]
- Hardman, D.T.; Fisher, C.M.; Patel, M.I.; Neale, M.; Chambers, J.; Lane, R.; Appleberg, M. Ruptured abdominal aortic aneurysms: Who should be offered surgery? J. Vasc. Surg. 1996, 23, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.C.; Hildebrand, H.D.; Salvian, A.J.; Taylor, D.C.; Strandberg, S.; Myckatyn, T.M.; Hsiang, Y.N. Predictors of death in nonruptured and ruptured abdominal aortic aneurysms. J. Vasc. Surg. 1996, 24, 614–620, discussion 621–623. [Google Scholar] [CrossRef] [Green Version]
- Tambyraja, A.; Murie, J.; Chalmers, R. Predictors of outcome after abdominal aortic aneurysm rupture: Edinburgh Ruptured Aneurysm Score. World J. Surg. 2007, 31, 2243–2247. [Google Scholar] [CrossRef]
- Robinson, W.; Schanzer, A.; Li, Y.; Goodney, P.; Nolan, B.; Eslami, M.; Cronenwett, J.L.; Messina, L.M. Derivation and validation of a practical risk score for prediction of mortality after open repair of ruptured abdominal aortic aneurysms in a U.S. regional cohort and comparison to existing scoring systems. J. Vasc. Surg. 2013, 57, 354–361. [Google Scholar] [CrossRef] [Green Version]
- Wise, E.; Hocking, K.; Brophy, C. Prediction of in-hospital mortality after ruptured abdominal aortic aneurysm repair using an artificial neural network. J. Vasc. Surg. 2015, 62, 8–15. [Google Scholar] [CrossRef] [Green Version]
- Garland, B.T.; Danaher, P.J.; Desikan, S.; Tran, N.T.; Quiroga, E.; Singh, N.; Starnes, B.W. Preoperative risk score for the prediction of mortality afrer repair of ruptured abdominal aortic aneurysms. J. Vasc. Surg. 2018, 68, 991–997. [Google Scholar] [CrossRef]
- Meguid, R.A.; Brooke, B.S.; Perler, B.A.; Freischlag, J.A. Impact of hospital teaching status on survival from ruptured abdominal aneurysm repair. In Proceedings of the Annual Meeting of Eastern Vascular Society, Boston, MA, USA, 12 September 2008. [Google Scholar]
- Oyague, K.S.; Mubarak, O.A.; Nowak, L.R.; Gainer, J.G.; Rehring, T.F.; O’Brien, M.M.; Hollis, H.W., Jr. Endovascular repair of ruptured and symptomatic abdominal aortic aneurysms using a structured protocol in a community teaching hospital. Ann. Vasc. Surg. 2015, 29, 76–83. [Google Scholar] [CrossRef]
- Mayer, D.; Aeschbacher, S.; Pfammatter, T. Complete replacement of open repair for ruptured abdominal aortic aneurysms by endovascular aneurysm repair. A two-center 14-year experience. J. Vasc. Surg. 2013, 57, 1172. [Google Scholar] [CrossRef] [Green Version]
- McPhee, J.; Eslami, M.H.; Arous, E.J.; Messina, L.M.; Schanzer, A. Endovascular treatment of ruptured abdominal aortic aneurysms in the United States (2001–2006): A significant survival benefit over open repair is independently associated with increased institutional volume. J. Vasc. Surg. 2009, 49, 817–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, T.; Lindop, M.; Munday, I.; Quick, C.R.; Gaunt, M.E.; Varty, K. A cost analysis of surgery for ruptured abdominal aortic aneurysm. Eur J. Vasc. Endovasc. Surg. 2003, 26, 299–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| n = 500 | n = 177 | n = 323 | ||
|---|---|---|---|---|
| Demographics | Whole Study Group | Patients Who Died | Patients Who Survived | p Value |
| Age > 74 | 188 (37.6%) | 107 (60.5%) | 81 (25.1%) | <0.001 |
| Female | 81 (16.2%) | 38 (21.5%) | 43 (13.3%) | 0.022 |
| Risk factors | ||||
| Obesity | 176 (35.2%) | 71 (40.1%) | 105 (32.5%) | 0.08 |
| Smoking | 287 (57.4%) | 103 (58.5%) | 184 (57.1%) | 0.76 |
| Hypertension | 461 (92.2%) | 166 (93.8%) | 295 (91.3%) | 0.33 |
| Diabetes mellitus | 84 (16.8%) | 34 (19.2%) | 50 (15.5%) | 0.28 |
| Previous myocardial infarction | 92 (18.4%) | 47 (26.6%) | 45 (13.9%) | <0.001 |
| Previous myocardial revascularisation | 46 (9.2%) | 20 (11.3%) | 26 (8%) | 0.23 |
| Angina pectoris | 60 (12%) | 87 (49.2%) | 79 (24.5%) | <0.001 |
| Heart failure | 88 (17.6%) | 53 (29.9%) | 35 (10.8%) | <0.001 |
| Atrial fibrillation | 60 (12%) | 31 (17.5%) | 29 (9%) | 0.005 |
| Previous stroke | 47 (9.4%) | 24 (13.6%) | 23 (7.1%) | 0.018 |
| COPD | 181 (36.2%) | 85 (48%) | 96 (29.7%) | <0.001 |
| CKD | 71 (14.2%) | 35 (19.8%) | 36 (11.1%) | 0.008 |
| Clinical presentation | ||||
| Abdominal/low back pain | 495 (99%) | 176 (99.4%) | 319 (98.8%) | 0.47 |
| Pulsatile abdominal mass | 438 (87.6%) | 158 (89.3%) | 280 (86.7%) | 0.41 |
| Hypovolemic shock | 369 (73.8%) | 160 (90.4%) | 209 (64.7%) | <0.001 |
| Collapse | 240 (48%) | 119 (67.2%) | 121 (37.5%) | <0.001 |
| Unconsciousness | 95 (19%) | 64 (36.2%) | 31 (9.6%) | <0.001 |
| Ventricular arrhythmia | 37 (7.4%) | 25 (14.1%) | 12 (3.7%) | <0.001 |
| Cardiac arrest | 10 (2%) | 9 (5.1%) | 1 (0.3%) | <0.001 |
| Haemodynamics | ||||
| SAP < 70 (mmHg) | 119 (23.8%) | 75 (42.4%) | 44 (13.6%) | <0.001 |
| DAP < 60 (mmHg) | 293 (58.6%) | 142 (80.2%) | 151 (46.7%) | <0.001 |
| MAP < 60 (mmHg) | 187 (37.4%) | 100 (56.5%) | 87 (26.9%) | <0.001 |
| Laboratory | ||||
| Haemoglobin < 78 (g/L) | 118 (23.6%) | 69 (39%) | 49 (15.2%) | <0.001 |
| Platelets < 145 (109) | 154 (30.8%) | 93 (52.5%) | 87 (26.9%) | <0.001 |
| Creatinine > 145 (mmol/L) | 159 (31.8%) | 83 (46.9%) | 76 (23.5%) | <0.001 |
| Anatomic characteristics | |
| AAA size (mm) | 80 ± 16.8 |
| AAA localization | |
| Infrarenal | 409 (81.8%) |
| Juxtarenal | 76 (15.2%) |
| Iliac | 14 (3%) |
| Procedural characteristics | |
| Position of proximal aortic clamp | |
| Infrarenal | 145 (29%) |
| Suprarenal | 16 (3.2%) |
| Supraceliac | 339 (67.8%) |
| Duration of proximal aortic clamping (min) | 36.6 ± 24.5 |
| Type of reconstruction | |
| None | 18 (3.6%) |
| Tube graft interposition | 262 (52.4%) |
| AII bypass | 140 (28%) |
| AFF bypass | 80 (16%) |
| Total operative time (min) | 166.5 ± 50.6 |
| Blood loss (ml) | 3000 (2000–4500) |
| Acute kidney injury | 70 (14%) |
| Pulmonary complications * | 111 (22.2%) |
| Surgical reintervention | 69 (13.8%) |
| Major bleeding requiring reintervention | 38 (7.6%) |
| Lower limb ischaemia | 17 (3.4%) |
| Stroke | 16 (3.2%) |
| Acute coronary syndrome | 31 (6.2%) |
| Ischaemic colitis | 26 (5.2%) |
| Sepsis | 7 (1.4%) |
| Wound infection | 6 (1.2%) |
| Wound dehiscence | 4 (0.8%) |
| Abdominal compartment syndrome | 13 (2.6%) |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
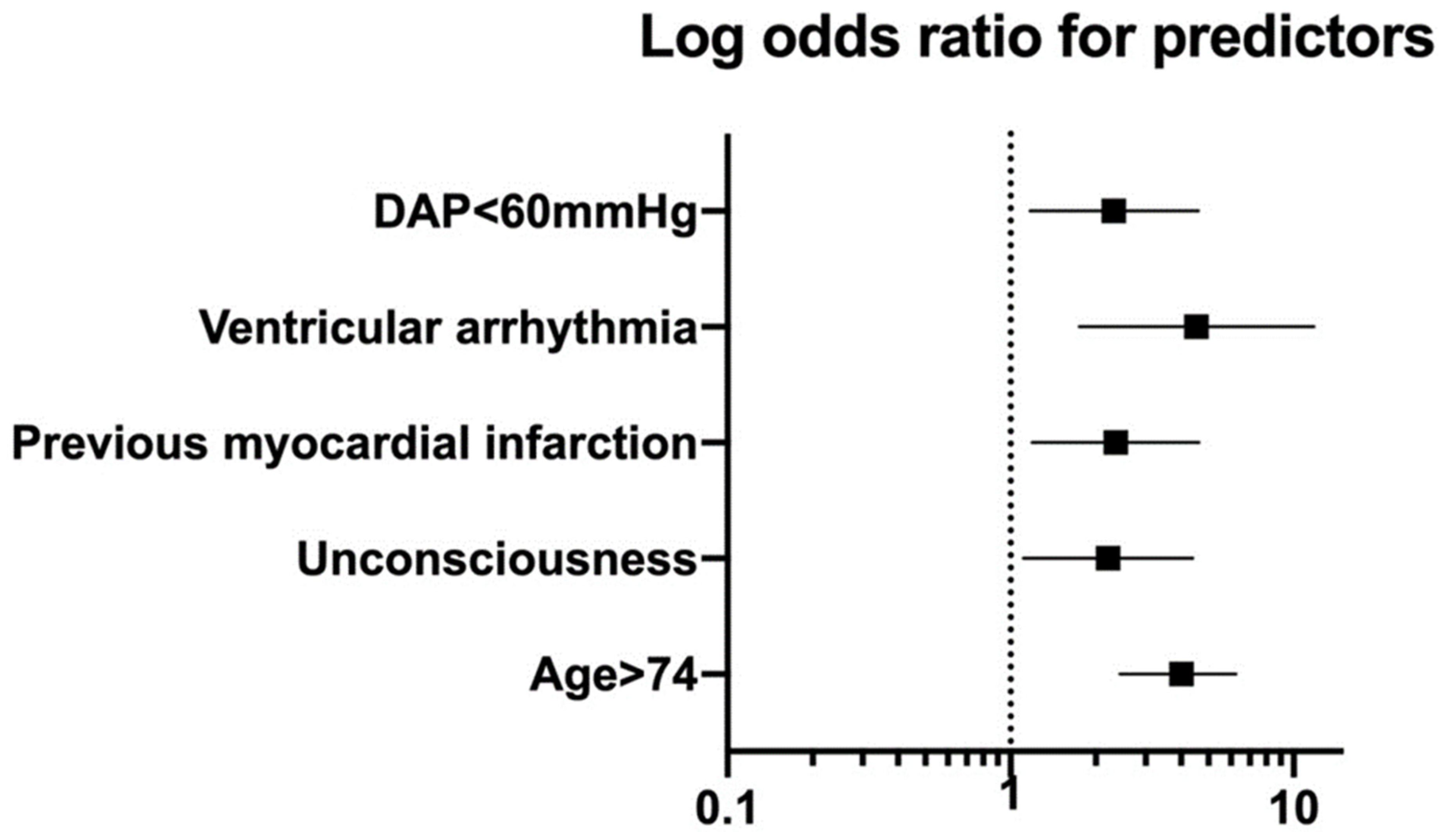
| Variables | OR | 95%CI | p Values | OR | 95%CI | p Values |
| Age > 74 | 4.56 | 3.08–6.76 | <0.001 | 4.01 | 2.43–6.26 | <0.001 |
| Unconsciousness | 5.33 | 3.30–8.63 | <0.001 | 2.21 | 1.11–4.40 | 0.024 |
| Previous myocardial infarction | 2.23 | 1.41–3.53 | <0.001 | 2.35 | 1.19–4.63 | 0.014 |
| Ventricular arrhythmia | 4.26 | 2.08–8.71 | <0.001 | 4.54 | 1.75–11.78 | 0.002 |
| DAP < 60 mmHg | 4.62 | 3.00–7.10 | <0.001 | 2.32 | 1.17–4.62 | 0.016 |
| Predictors | OR | Points |
|---|---|---|
| Age > 74 | 4.01 | 1 |
| Unconsciousness | 2.21 | 1 |
| Previous myocardial infarction | 2.35 | 1 |
| Ventricular arrhythmia | 4.54 | 1 |
| DAP < 60 mmHg | 2.32 | 1 |
| Score | 0 | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|---|
| Deaths, n (%) | 7 (7.4%) | 22 (15.3%) | 44 (34.9%) | 58 (68.2%) | 37 (88.1%) | 9 (100%) |
| Number of patients | 94 | 144 | 126 | 85 | 42 | 9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomic, I.; Zlatanovic, P.; Markovic, M.; Sladojevic, M.; Mutavdzic, P.; Trailovic, R.; Jovanovic, K.; Matejevic, D.; Milicic, B.; Davidovic, L. Identification of Risk Factors and Development of Predictive Risk Score Model for Mortality after Open Ruptured Abdominal Aortic Aneurysm Repair. Medicina 2022, 58, 549. https://doi.org/10.3390/medicina58040549
Tomic I, Zlatanovic P, Markovic M, Sladojevic M, Mutavdzic P, Trailovic R, Jovanovic K, Matejevic D, Milicic B, Davidovic L. Identification of Risk Factors and Development of Predictive Risk Score Model for Mortality after Open Ruptured Abdominal Aortic Aneurysm Repair. Medicina. 2022; 58(4):549. https://doi.org/10.3390/medicina58040549
Chicago/Turabian StyleTomic, Ivan, Petar Zlatanovic, Miroslav Markovic, Milos Sladojevic, Perica Mutavdzic, Ranko Trailovic, Ksenija Jovanovic, David Matejevic, Biljana Milicic, and Lazar Davidovic. 2022. "Identification of Risk Factors and Development of Predictive Risk Score Model for Mortality after Open Ruptured Abdominal Aortic Aneurysm Repair" Medicina 58, no. 4: 549. https://doi.org/10.3390/medicina58040549