
Quantitative Changes in White Blood Cells: Correlation with the Hallmarks of Polycystic Ovary Syndrome

 ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Design, Setting, and Subjects
2.2. Laboratory Investigations
2.3. Ultrasonography
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Azziz, R.; Woods, K.S.; Reyna, R.; Key, T.J.; Knochenhauer, E.S.; Yildiz, B.O. The prevalence and features of the polycystic ovary syndrome in an unselected population. J. Clin. Endocrinol. Metab. 2004, 89, 2745–2749. [Google Scholar] [CrossRef] [PubMed]
- Rotteredam, E. Rotterdam ESHRE/ASRM-Sponsored PCOS consensus workshop group (2004) Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod. 2004, 19, 41–47. [Google Scholar]
- Dumesic, D.A.; Richards, J.S. Ontogeny of the ovary in polycystic ovary syndrome. Fertil. Steril. 2013, 100, 23–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Escobar-Morreale, H.F.; Luque-Ramírez, M.; González, F. Circulating inflammatory markers in polycystic ovary syndrome: A systematic review and metaanalysis. Fertil. Steril. 2011, 95, 1048–1058.e1042. [Google Scholar] [CrossRef] [Green Version]
- Orio, F., Jr.; Palomba, S.; Cascella, T.; Di Biase, S.; Manguso, F.; Tauchmanovà, L.; Nardo, L.G.; Labella, D.; Savastano, S.; Russo, T.; et al. The increase of leukocytes as a new putative marker of low-grade chronic inflammation and early cardiovascular risk in polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2005, 90, 2–5. [Google Scholar] [CrossRef] [Green Version]
- Phelan, N.; O’Connor, A.; Kyaw Tun, T.; Correia, N.; Boran, G.; Roche, H.M.; Gibney, J. Leucocytosis in women with polycystic ovary syndrome (PCOS) is incompletely explained by obesity and insulin resistance. Clin. Endocrinol. 2013, 78, 107–113. [Google Scholar] [CrossRef]
- Duleba, A.J.; Dokras, A. Is PCOS an inflammatory process? Fertil. Steril. 2012, 97, 7–12. [Google Scholar] [CrossRef] [Green Version]
- Covington, J.D.; Tam, C.S.; Pasarica, M.; Redman, L.M. Higher circulating leukocytes in women with PCOS is reversed by aerobic exercise. Biochimie 2016, 124, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Aboeldalyl, S.; James, C.; Seyam, E.; Ibrahim, E.M.; Shawki, H.E.; Amer, S. The Role of Chronic Inflammation in Polycystic Ovarian Syndrome-A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2021, 22, 734. [Google Scholar] [CrossRef]
- Barvitenko, N.N.; Adragna, N.C.; Weber, R.E. Erythrocyte signal transduction pathways, their oxygenation dependence and functional significance. Cell. Physiol. Biochem. 2005, 15, 1–18. [Google Scholar] [CrossRef]
- Balog, T.; Marotti, T.; Abramić, M.; Beusan-Svoboda, I.; Sobocanec, S.; Hrsak, I. Neutrophil neutral endopeptidase variation and its regulation by opioid peptides. Int. Immunopharmacol. 2001, 1, 569–579. [Google Scholar] [CrossRef]
- Taylor, S.; Dirir, O.; Zamanian, R.T.; Rabinovitch, M.; Thompson, A.A.R. The Role of Neutrophils and Neutrophil Elastase in Pulmonary Arterial Hypertension. Front. Med. 2018, 5, 217. [Google Scholar] [CrossRef]
- Çakıroğlu, Y.; Vural, F.; Vural, B. The inflammatory markers in polycystic ovary syndrome: Association with obesity and IVF outcomes. J. Endocrinol. Investig. 2016, 39, 899–907. [Google Scholar] [CrossRef]
- Yilmaz, M.; Duran, C.; Basaran, M. The mean platelet volume and neutrophil to lymphocyte ratio in obese and lean patients with polycystic ovary syndrome. J. Endocrinol. Investig. 2016, 39, 45–53. [Google Scholar] [CrossRef]
- Mihailidis, J.; Dermesropian, R.; Taxel, P.; Luthra, P.; Grant-Kels, J.M. Endocrine evaluation of hirsutism. Int. J. Women’s Dermatol. 2015, 1, 90–94. [Google Scholar] [CrossRef] [Green Version]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). JAMA 2001, 285, 2486. [Google Scholar] [CrossRef]
- Salama, A.S.-A.; Matta, R.A.-E.; Elhini, S.H.; Hamdi, L.; Adel, L.; Hassan, H. High-normal thyroid stimulating hormone is a predictor of metabolic syndrome among young polycystic ovary syndrome women. Egypt. J. Obes. Diabetes Endocrinol. 2016, 2, 146. [Google Scholar]
- World Health Organization—Regional Office for the Western Pacific. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications: Sydney, Australia, 2000. [Google Scholar]
- Bickerton, A.S.T.; Clark, N.; Meeking, D.; Shaw, K.M.; Crook, M.; Lumb, P.; Turner, C.; Cummings, M.H. Cardiovascular risk in women with polycystic ovarian syndrome (PCOS). J. Clin. Pathol. 2005, 58, 151–154. [Google Scholar] [CrossRef] [Green Version]
- Cibula, D.; Cífková, R.; Fanta, M.; Poledne, R.; Zivny, J.; Skibová, J. Increased risk of non-insulin dependent diabetes mellitus, arterial hypertension and coronary artery disease in perimenopausal women with a history of the polycystic ovary syndrome. Hum. Reprod. 2000, 15, 785–789. [Google Scholar] [CrossRef]
- Christakou, C.D.; Diamanti-Kandarakis, E. Role of Androgen Excess on Metabolic Aberrations and Cardiovascular Risk in Women with Polycystic Ovary Syndrome. Women’s Health 2008, 4, 583–594. [Google Scholar] [CrossRef]
- Kelly, C.C.; Lyall, H.; Petrie, J.R.; Gould, G.W.; Connell, J.M.; Sattar, N. Low grade chronic inflammation in women with polycystic ovarian syndrome. J. Clin. Endocrinol. Metab. 2001, 86, 2453–2455. [Google Scholar] [CrossRef] [PubMed]
- Agacayak, E.; Tunc, S.Y.; Sak, S.; Basaranoglu, S.; Yüksel, H.; Turgut, A.; Gul, T. Levels of neopterin and other inflammatory markers in obese and non-obese patients with polycystic ovary syndrome. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2015, 21, 2446. [Google Scholar]
- Keskin Kurt, R.; Okyay, A.G.; Hakverdi, A.U.; Gungoren, A.; Dolapcioglu, K.S.; Karateke, A.; Dogan, M.O. The effect of obesity on inflammatory markers in patients with PCOS: A BMI-matched case–control study. Arch. Gynecol. Obstet. 2014, 290, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Guasti, L.; Dentali, F.; Castiglioni, L.; Maroni, L.; Marino, F.; Squizzato, A.; Ageno, W.; Gianni, M.; Gaudio, G.; Grandi, A.M.; et al. Neutrophils and clinical outcomes in patients with acute coronary syndromes and/or cardiac revascularisation. A systematic review on more than 34,000 subjects. Thromb. Haemost. 2011, 106, 591–599. [Google Scholar] [CrossRef] [Green Version]
- Sunbul, M.; Gerin, F.; Durmus, E.; Kivrak, T.; Sari, I.; Tigen, K.; Cincin, A. Neutrophil to lymphocyte and platelet to lymphocyte ratio in patients with dipper versus non-dipper hypertension. Clin. Exp. Hypertens. 2014, 36, 217–221. [Google Scholar] [CrossRef]
- Tamhane, U.U.; Aneja, S.; Montgomery, D.; Rogers, E.K.; Eagle, K.A.; Gurm, H.S. Association between admission neutrophil to lymphocyte ratio and outcomes in patients with acute coronary syndrome. Am. J. Cardiol. 2008, 102, 653–657. [Google Scholar] [CrossRef]
- Gomathi, K.; Shaafie, I.; Mummigatti, K.; Shahid, S.; Sreedharan, J. Biochemical parameters in women with polycystic ovary syndrome in Ajman, UAE. Nepal J. Obstet. Gynaecol. 2011, 6, 7–10. [Google Scholar] [CrossRef] [Green Version]
- Naidu, J.N.; Swapna, G.N.; Kumar, A.N.; Krishnamma, M.; Anitha, M. Importance of elevated insulin resistance, dyslipidemia and status of antioxidant vitamins in polycystic ovary disease. Free Radic. Antioxid. 2013, 3, 17–19. [Google Scholar] [CrossRef] [Green Version]
- Rasool, S.O. Anthropometric measurements in PCOS & Non PCO Infertile patients. Int. J. Chem. Environ. Biol. Sci. 2015, 3, 14–16. [Google Scholar]
- Kumar, A.N.; Naidu, J.N.; Uppala Satyanarayana, K.R.; Anitha, M. Metabolic and endocrine characteristics of Indian women with polycystic ovary syndrome. Int. J. Fertil. Steril. 2016, 10, 22. [Google Scholar]
- Shah, A.K.; Sarin, M.; Karunanand, B.; Mohapatra, S.; Bhat, S.A. Association of hormonal status with anthropometric & biochemical parameters in women with polycystic ovarian syndrome. Hypertension 2017, 3, 5. [Google Scholar]
- Bousmpoula, A.; Kouskouni, E.; Benidis, E.; Demeridou, S.; Kapeta-Kourkouli, R.; Chasiakou, A.; Baka, S. Adropin levels in women with polycystic ovaries undergoing ovarian stimulation: Correlation with lipoprotein lipid profiles. Gynecol. Endocrinol. 2018, 34, 153–156. [Google Scholar] [CrossRef]
- Cui, L.; Li, G.; Zhong, W.; Bian, Y.; Su, S.; Sheng, Y.; Shi, Y.; Wei, D.; Zhang, W.; Zhao, H.; et al. Polycystic ovary syndrome susceptibility single nucleotide polymorphisms in women with a single PCOS clinical feature. Hum. Reprod. 2015, 30, 732–736. [Google Scholar] [CrossRef] [Green Version]
- Cui, L.; Zhao, H.; Zhang, B.; Qu, Z.; Liu, J.; Liang, X.; Zhao, X.; Zhao, J.; Sun, Y.; Wang, P.; et al. Genotype–phenotype correlations of PCOS susceptibility SNPs identified by GWAS in a large cohort of Han Chinese women. Hum. Reprod. 2012, 28, 538–544. [Google Scholar] [CrossRef] [Green Version]
- Iuhas, C.I.; Costin, N.; Dan, M. Lipid parameters in patients with polycystic ovary syndrome. Appl. Med. Inform. 2012, 31, 27–32. [Google Scholar]
- Macut, D.; Damjanovic, S.; Panidis, D.; Spanos, N.; Glisic, B.; Petakov, M.; Rousso, D.; Kourtis, A.; Bjekic, J.; Milic, N. Oxidised low-density lipoprotein concentration–early marker of an altered lipid metabolism in young women with PCOS. Eur. J. Endocrinol. 2006, 155, 131–136. [Google Scholar] [CrossRef] [Green Version]
- Tsouma, I.; Kouskouni, E.; Demeridou, S.; Boutsikou, M.; Hassiakos, D.; Chasiakou, A.; Hassiakou, S.; Gennimata, V.; Baka, S. Lipid lipoprotein profile alterations in Greek infertile women with polycystic ovaries: Influence of adipocytokines levels. Vivo 2014, 28, 935–939. [Google Scholar]
- Vital-Reyes, V.; Lopez-Alarcón, M.; Inda-Icaza, P.; Márquez-Maldonado, C. Subtle metabolic alterations in adolescents with obesity and polycystic ovarian syndrome. Gac. Med. De Mex. 2017, 153, S34–S41. [Google Scholar]
- Ferriman, D.; Gallwey, J. Clinical assessment of body hair growth in women. J. Clin. Endocrinol. Metab. 1961, 21, 1440–1447. [Google Scholar] [CrossRef]
- Suzuki, K.; Hayano, Y.; Nakai, A.; Furuta, F.; Noda, M. Adrenergic control of the adaptive immune response by diurnal lymphocyte recirculation through lymph nodes. J. Exp. Med. 2016, 213, 2567–2574. [Google Scholar] [CrossRef] [Green Version]
- Vaduganathan, M.; Ambrosy, A.P.; Greene, S.J.; Mentz, R.J.; Subacius, H.P.; Maggioni, A.P.; Swedberg, K.; Nodari, S.; Zannad, F.; Konstam, M.A.; et al. Predictive value of low relative lymphocyte count in patients hospitalized for heart failure with reduced ejection fraction: Insights from the EVEREST trial. Circ. Heart Fail. 2012, 5, 750–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balta, S.; Celik, T.; Mikhailidis, D.P.; Ozturk, C.; Demirkol, S.; Aparci, M.; Iyisoy, A. The relation between atherosclerosis and the neutrophil–lymphocyte ratio. Clin. Appl. Thromb./Hemost. 2016, 22, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Rasool, S.; Ashraf, S.; Nabi, M.; Rashid, F.; Fazili, K.M.; Amin, S. Elevated fasting insulin is associated with cardiovascular and metabolic risk in women with polycystic ovary syndrome. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2098–2105. [Google Scholar] [CrossRef] [PubMed]
- Nabi, M.; Andrabi, S.M.; Rasool, S.; Ashraf, S.; Majid, I.; Amin, S. Androgen receptor coregulator long noncoding RNA CTBP1-AS is associated with polycystic ovary syndrome in Kashmiri women. Endocrine 2022, 75, 614–622. [Google Scholar] [CrossRef]
- Ashraf, S.; Rasool, S.; Nabi, M.; Ganie, M.A.; Masoodi, S.R.; Amin, S. Impact of rs2414096 polymorphism of CYP19 gene on susceptibility of polycystic ovary syndrome and hyperandrogenism in Kashmiri women. Sci. Rep. 2021, 11, 12942. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Features | PCOS (n = 88) | Controls (n = 118) | p a |
|---|---|---|---|
| Age (years) | 21.10 ± 0.30 | 21.08 ± 0.06 | 0.740 |
| Body mass index (kg/m2) | 26.14 ± 1.02 | 24.43 ± 0.14 | 0.000 |
| Waist circumference (cm) | 94.30 ± 0.29 | 76.04 ± 0.51 | 0.000 |
| Hemoglobin (gm/dL) | 12.24 ± 1.10 | 12.86 ± 0.10 | 0.000 |
| HCT (%) | 38.28 ± 3.27 | 41.81 ± 0.12 | 0.000 |
| Red blood cell count (106/μL) | 4.74 ± 0.60 | 4.13 ± 0.11 | 0.000 |
| MCV (fL) | 81.36 ± 11.65 | 87.48 ± 0.21 | 0.000 |
| MCH (pg) | 24.24 ± 0.68 | 31.09 ± 0.11 | 0.000 |
| MCHC (gm/dL) | 31.92 ± 2.33 | 33.47 ± 0.15 | 0.000 |
| White blood cell count (103/μL) | 7.07 ± 2.49 | 4.87 ± 0.14 | 0.224 |
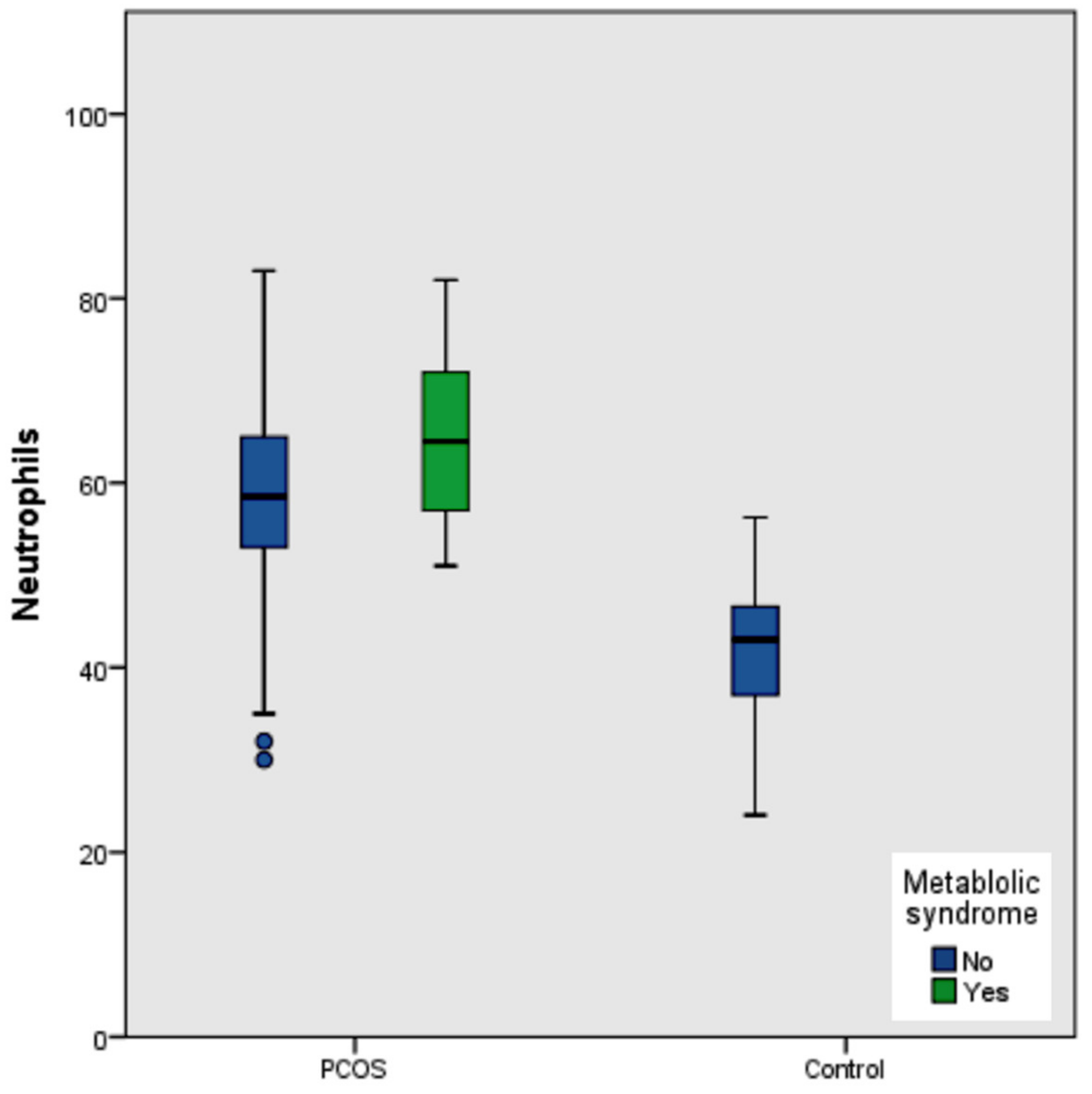
| Neutrophils (%) | 60.81 ± 10.76 | 41.44 ± 0.90 | 0.000 |
| Lymphocytes (%) | 38.77 ± 10.74 | 46.99 ± 1.63 | 0.000 |
| Monocytes (%) | 0.15 ± 0.38 | 0.83 ± 0.13 | 0.000 |
| Eosinophils (%) | 0.27 ± 0.60 | 0.41 ± 0.82 | 0.191 |
| Neutrophil–lymphocyte ratio | 1.80 ± 0.95 | 0.77 ± 0.26 | 0.000 |
| Eosinophil–lymphocyte ratio | 0.007 ± 0.01 | 0.008 ± 0.001 | 0.738 |
| Platelets–lymphocyte ratio | 158.69 ± 109.44 | 127.33 ± 110.47 | 0.000 |
| Platelets (×109/L) | 250.08 ± 87.50 | 243.87 ± 4.14 | 0.544 |
| PCT (%) | 0.26 ± 0.09 | 0.60 ± 0.04 | 0.000 |
| MPV (fL) | 10.49 ± 1.25 | 11.18 ± 0.12 | 0.000 |
| Total cholesterol (mg/dL) | 183.95 ± 42.58 | 116.44 ± 1.37 | 0.000 |
| Triglyceride (mg/dL) | 143.63 ± 41.93 | 109.85 ± 1.26 | 0.000 |
| HDL-C (mg/dL) | 41.84 ± 6.49 | 44.05 ± 0.63 | 0.000 |
| LDL-C (mg/dL) | 113.78 ± 38.43 | 47.24 ± 1.88 | 0.000 |
| Total triiodothyronine (ng/mL) | 1.56 ± 0.55 | 1.45 ± 0.06 | 0.223 |
| Total thyroxine (μg/dL) | 8.28 ± 2.47246 | 7.03 ± 0.12 | 0.005 |
| Thyroid stimulating hormone (μIU/mL) | 4.19 ± 1.51 | 3.99 ± 0.13 | 0.361 |
| Follicle stimulating hormone (IU/L) | 7.38 ± 2.57 | 8.15 ± 0.13 | 0.014 |
| Luteinizing hormone (IU/L) | 14.86 ± 4.75 | 5.36 ± 0.15 | 0.000 |
| Prolactin (ng/dL) | 16.73 ± 6.79 | 11.94 ± 0.48 | 0.000 |
| Total testosterone (ng/mL) | 53.07 ± 28.24 | 19.23 ± 0.45 | 0.000 |
| Right ovary volume (cc) | 17.41 ± 5.99 | 9 ± 0.00 | 0.000 |
| Left ovary volume (cc) | 16.36 ± 4.74 | 9 ± 0.00 | 0.000 |
| Variable | PCOS | |
|---|---|---|
| r | p | |
| Age | 0.062 | 0.565 |
| Body mass index | −0.014 | 0.896 |
| Hemoglobin | 0.058 | 0.591 |
| HCT | 0.125 | 0.248 |
| MCV | −0.135 | 0.210 |
| MCH | −0.079 | 0.465 |
| MCHC | −0.013 | 0.907 |
| White blood cell count | 0.182 | 0.089 |
| Lymphocytes | −0.997 | 0.000 |
| Monocytes | −0.081 | 0.452 |
| Eosinophils | −0.018 | 0.865 |
| Neutrophil–lymphocyte ratio | 0.930 | 0.000 |
| Eosinophil–lymphocyte ratio | 0.023 | 0.829 |
| Monocyte–lymphocyte ratio | 0.009 | 0.936 |
| Platelets–lymphocyte ratio | 0.674 | 0.000 |
| Platelets | 0.139 | 0.198 |
| Serum cholesterol | −0.095 | 0.380 |
| Serum triglyceride | 0.015 | 0.887 |
| HDL-C | −0.080 | 0.458 |
| LDL-C | −0.098 | 0.363 |
| Total triiodothyronine | 0.038 | 0.729 |
| Total thyroxine | 0.050 | 0.646 |
| Thyroid stimulating hormone | −0.049 | 0.651 |
| Follicle stimulating hormone | 0.042 | 0.696 |
| Luteinizing hormone | 0.196 | 0.068 |
| Testosterone | 0.004 | 0.969 |
| Right ovary volume | 0.150 | 0.162 |
| Left ovary volume | 0.007 | 0.947 |
| Wrist circumference | 0.108 | 0.318 |
| Features | β | p Value |
|---|---|---|
| Hemoglobin (gm/dL) | 0.000 | 1.000 |
| HCT (%) | 0.000 | 1.000 |
| Red blood cell count (106/μL) | 0.000 | 1.000 |
| MCV (fL) | 0.000 | 1.000 |
| MCH (pg) | 0.000 | 1.000 |
| MCHC (gm/dL) | 0.000 | 1.000 |
| White blood cell count (103/μL) | 0.000 | 1.000 |
| Lymphocytes (%) | −0.999 | 0.000 |
| Monocytes (%) | −0.036 | 0.000 |
| Eosinophils (%) | −0.056 | 0.000 |
| Neutrophil–lymphocyte ratio | 0.000 | 1.000 |
| Eosinophil–lymphocyte ratio | 0.000 | 1.000 |
| Monocyte–lymphocyte ratio | 0.000 | 1.000 |
| Platelets–lymphocyte ratio | 0.000 | 1.000 |
| MPV (fL) | 0.000 | 1.000 |
| PDWC (%) | 0.000 | 1.000 |
| P-LCC (103/μL) | 0.000 | 1.000 |
| P-LCR (%) | 0.000 | 1.000 |
| Total cholesterol (mg/dL) | 0.000 | 1.000 |
| Triglyceride (mg/dL) | 0.000 | 1.000 |
| HDL-C (mg/dL) | 0.000 | 1.000 |
| LDL-C (mg/dL) | 0.000 | 1.000 |
| Total triiodothyronine (ng/mL) | 0.000 | 1.000 |
| Total thyroxine (μg/dL) | 0.000 | 1.000 |
| Thyroid stimulating hormone (μIU/m) | 0.000 | 1.000 |
| Follicle stimulating hormone (IU/L) | 0.000 | 1.000 |
| Luteinizing hormone (IU/L) | 0.000 | 1.000 |
| Total testosterone (ng/mL) | 0.000 | 1.000 |
| Waist circumference (cm) | 0.000 | 1.000 |
| Right ovary volume (cc) | 0.000 | 1.000 |
| Left ovary volume (cc) | 0.000 | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almaeen, A.H.; Alduraywish, A.A.; Nabi, M.; Shah, N.N.; Shaik, R.; Tantry, B.A. Quantitative Changes in White Blood Cells: Correlation with the Hallmarks of Polycystic Ovary Syndrome. Medicina 2022, 58, 535. https://doi.org/10.3390/medicina58040535
Almaeen AH, Alduraywish AA, Nabi M, Shah NN, Shaik R, Tantry BA. Quantitative Changes in White Blood Cells: Correlation with the Hallmarks of Polycystic Ovary Syndrome. Medicina. 2022; 58(4):535. https://doi.org/10.3390/medicina58040535
Chicago/Turabian StyleAlmaeen, Abdulrahman H., Abdulrahman Abdulwahab Alduraywish, Mudasar Nabi, Naveed Nazir Shah, Rahiman Shaik, and Bilal Ahmad Tantry. 2022. "Quantitative Changes in White Blood Cells: Correlation with the Hallmarks of Polycystic Ovary Syndrome" Medicina 58, no. 4: 535. https://doi.org/10.3390/medicina58040535