
Long-Term Survival Impact of High-Grade Complications after Liver Resection for Hepatocellular Carcinoma: A Retrospective Single-Centre Cohort Study

 and
and
Abstract
:1. Introduction
2. Materials and Methods
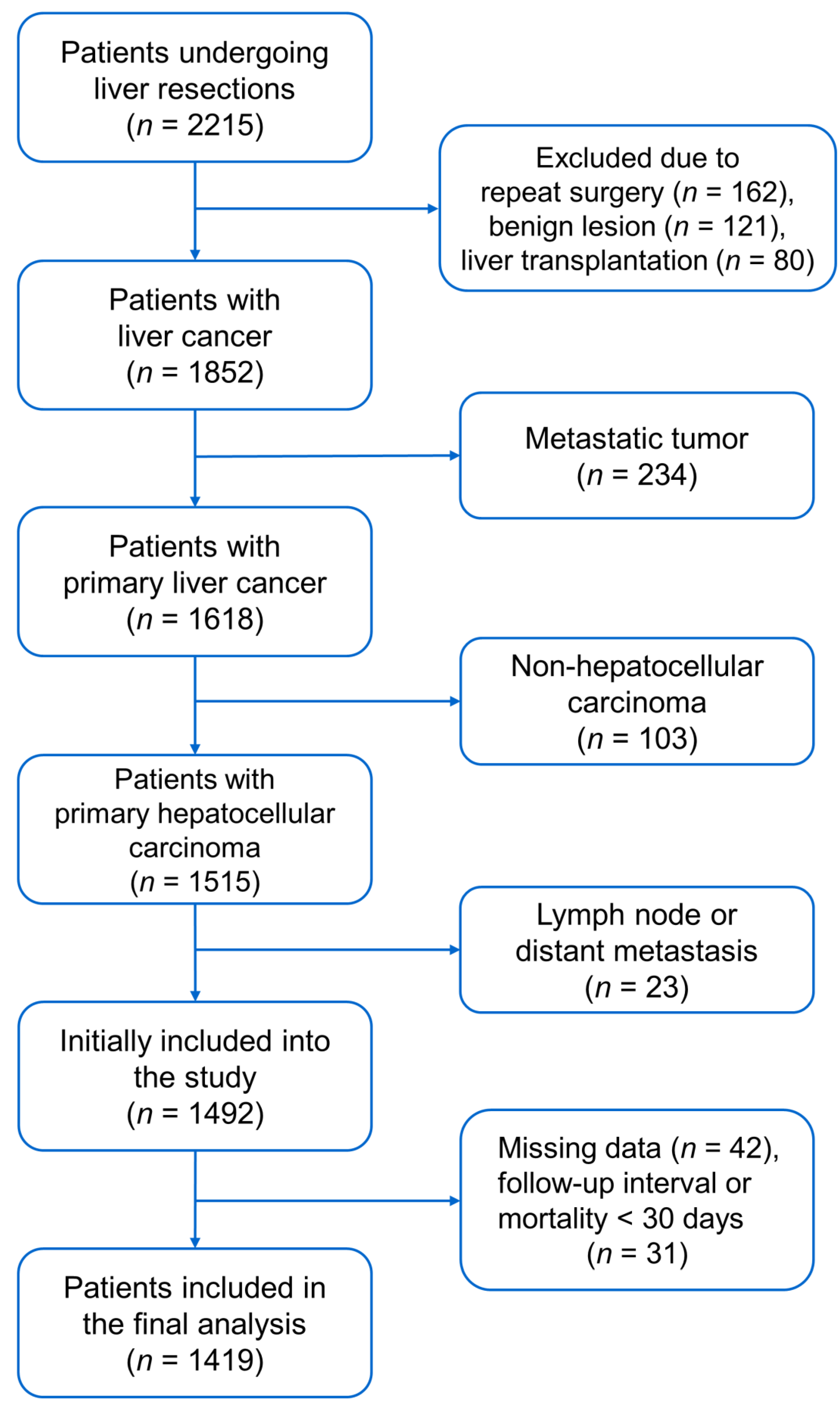
2.1. Criteria of Patient Selection
2.2. Postoperative Complications
2.3. Primary and Secondary Endpoints
2.4. Covariates for Adjustment
2.5. Surgical Techniques and Cancer Surveillance
2.6. Sample Size Estimation
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
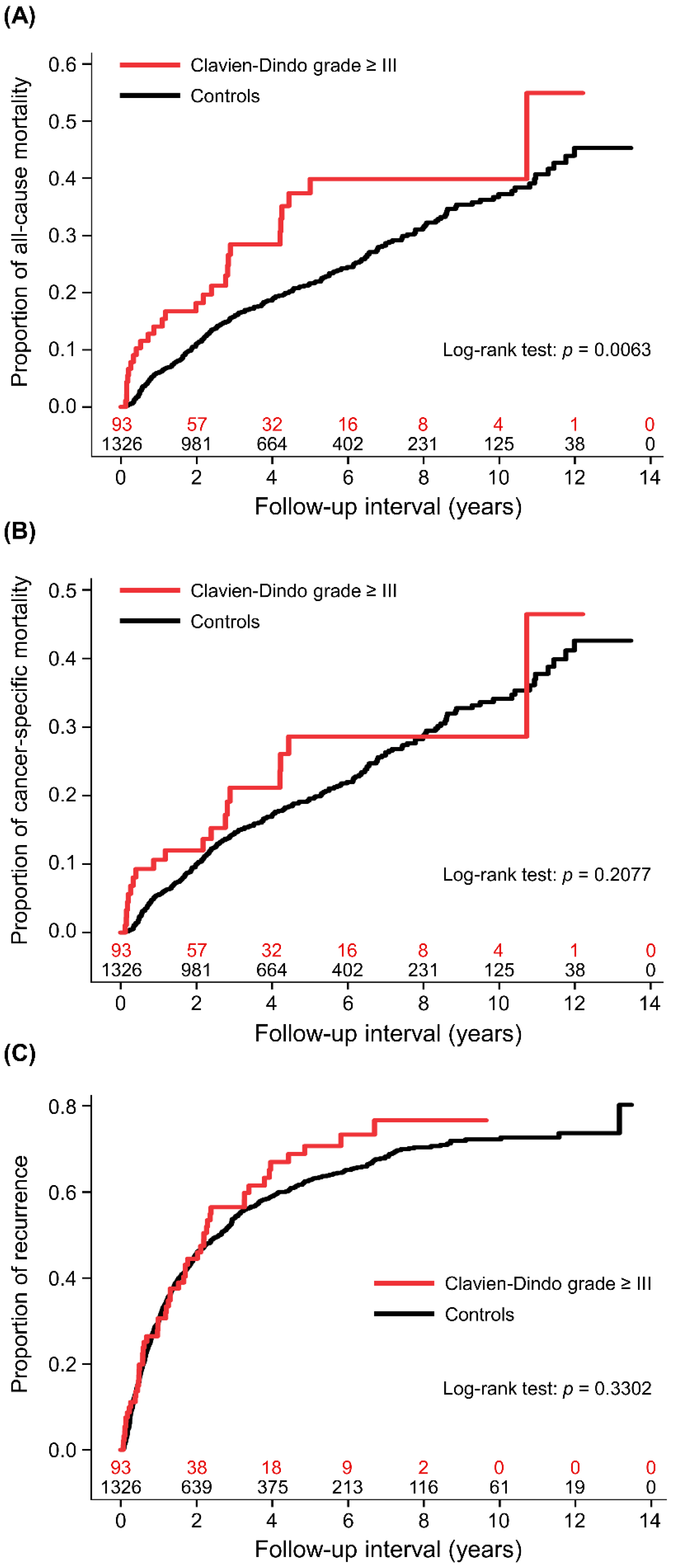
3.2. All-Cause Mortality
3.3. Cancer-Specific Mortality
3.4. Cancer Recurrence
3.5. Influential Factors for High-Grade Complications
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization; International Agency for Research on Cancer. GLOBOCAN: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2020. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/11-Liver-fact-sheet.pdf. (accessed on 5 April 2022).
- Ma, K.W.; Cheung, T.T. Surgical resection of localized hepatocellular carcinoma: Patient selection and special consideration. J. Hepatocell. Carcinoma 2016, 4, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Y.-J.; Lin, C.-N.; Sedghi, T.; Hsu, S.H.; Gross, C.P.; Wang, J.-D.; Wang, S.-Y. Treatment patterns and survival in hepatocellular carcinoma in the United States and Taiwan. PLoS ONE 2020, 15, e0240542. [Google Scholar] [CrossRef] [PubMed]
- Ishii, M.; Mizuguchi, T.; Harada, K.; Ota, S.; Meguro, M.; Ueki, T.; Nishidate, T.; Okita, K.; Hirata, K. Comprehensive review of post-liver resection surgical complications and a new universal classification and grading system. World J. Hepatol. 2014, 6, 745–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galun, D.; Bogdanovic, A.; Zivanovic, M.; Zuvela, M. Short- and long-term outcomes after hepatectomy in elderly patients with hepatocellular carcinoma: An analysis of 229 cases from a developing country. J. Hepatocell. Carcinoma 2021, 8, 155–165. [Google Scholar] [CrossRef]
- Harimoto, N.; Shirabe, K.; Ikegami, T.; Yoshizumi, T.; Maeda, T.; Kajiyama, K.; Yamanaka, T.; Maehara, Y. Postoperative complications are predictive of poor prognosis in hepatocellular carcinoma. J. Surg. Res. 2015, 199, 470–477. [Google Scholar] [CrossRef]
- Virani, S.; Michaelson, J.S.; Hutter, M.M.; Lancaster, R.T.; Warshaw, A.L.; Henderson, W.G.; Khuri, S.F.; Tanabe, K.K. Morbidity and mortality after liver resection: Results of the patient safety in surgery study. J. Am. Coll. Surg. 2007, 204, 1284–1292. [Google Scholar] [CrossRef]
- Spolverato, G.; Ejaz, A.; Kim, Y.; Weiss, M.; Wolfgang, C.L.; Hirose, K.; Pawlik, T.M. Readmission incidence and associated factors after a hepatic resection at a major hepato-pancreatico-biliary academic centre. HPB 2014, 16, 972–978. [Google Scholar] [CrossRef] [Green Version]
- Jin, S.; Fu, Q.; Wuyun, G.; Wuyun, T. Management of post-hepatectomy complications. World J. Gastroenterol. 2013, 19, 7983–7991. [Google Scholar] [CrossRef]
- Lorenzo, C.S.; Limm, W.M.; Lurie, F.; Wong, L.L. Factors affecting outcome in liver resection. HPB 2005, 7, 226–230. [Google Scholar] [CrossRef] [Green Version]
- Idrees, J.J.; Johnston, F.M.; Canner, J.K.; Dillhoff, M.; Schmidt, C.; Haut, E.R.; Pawlik, T.M. Cost of major complications after liver resection in the United States: Are high-volume centers cost-effective? Ann. Surg. 2019, 269, 503–510. [Google Scholar] [CrossRef]
- Khuri, S.F.; Henderson, W.G.; De Palma, R.G.; Mosca, C.; Healey, N.A.; Kumbhani, D.J. Determinants of long-term survival after major surgery and the adverse effect of postoperative complications. Ann. Surg. 2005, 242, 326–341, discussion 341–323. [Google Scholar] [CrossRef]
- Straatman, J.; Cuesta, M.A.; de Lange-de Klerk, E.S.; van der Peet, D.L. Long-term survival after complications following major abdominal surgery. J. Gastrointest. Surg. 2016, 20, 1034–1041. [Google Scholar] [CrossRef] [Green Version]
- Gowing, S.; Baker, L.; Tran, A.; Zhang, Z.; Ahn, H.; Ivanovic, J.; Anstee, C.; Grigor, E.; Gilbert, S.; Maziak, D.E.; et al. Postoperative adverse events are associated with oncologic recurrence following curative-intent resection for lung cancer. Lung 2020, 198, 973–981. [Google Scholar] [CrossRef]
- Suzuki, S.; Kanaji, S.; Matsuda, Y.; Yamamoto, M.; Hasegawa, H.; Yamashita, K.; Oshikiri, T.; Matsuda, T.; Sumi, Y.; Nakamura, T.; et al. Long-term impact of postoperative pneumonia after curative gastrectomy for elderly gastric cancer patients. Ann. Gastroenterol. Surg. 2017, 2, 72–78. [Google Scholar] [CrossRef]
- Sandini, M.; Ruscic, K.J.; Ferrone, C.R.; Qadan, M.; Eikermann, M.; Warshaw, A.L.; Lillemoe, K.D.; Castillo, C.F.-D. Major complications independently increase long-term mortality after pancreatoduodenectomy for cancer. J. Gastrointest. Surg. 2019, 23, 1984–1990. [Google Scholar] [CrossRef]
- Noba, L.; Rodgers, S.; Chandler, C.; Balfour, A.; Hariharan, D.; Yip, V.S. Enhanced Recovery After Surgery (ERAS) reduces hospital costs and improve clinical outcomes in liver surgery: A systematic review and meta-analysis. J. Gastrointest. Surg. 2020, 24, 918–932. [Google Scholar] [CrossRef] [Green Version]
- Chok, K.S.; Ng, K.K.; Poon, R.T.; Lo, C.M.; Fan, S.T. Impact of postoperative complications on long-term outcome of curative resection for hepatocellular carcinoma. Br. J. Surg. 2009, 96, 81–87. [Google Scholar] [CrossRef]
- Kusano, T.; Sasaki, A.; Kai, S.; Endo, Y.; Iwaki, K.; Shibata, K.; Ohta, M.; Kitano, S. Predictors and prognostic significance of operative complications in patients with hepatocellular carcinoma who underwent hepatic resection. Eur. J. Surg. Oncol. 2009, 35, 1179–1185. [Google Scholar] [CrossRef]
- Okamura, Y.; Takeda, S.; Fujii, T.; Sugimoto, H.; Nomoto, S.; Nakao, A. Prognostic significance of postoperative complications after hepatectomy for hepatocellular carcinoma. J. Surg. Oncol. 2011, 104, 814–821. [Google Scholar] [CrossRef]
- Zhou, Y.M.; Zhang, X.F.; Li, B.; Sui, C.J.; Yang, J.M. Postoperative complications affect early recurrence of hepatocellular carcinoma after curative resection. BMC Cancer 2015, 15, 689. [Google Scholar] [CrossRef] [Green Version]
- Doussot, A.; Lim, C.; Lahat, E.; Salloum, C.; Osseis, M.; Gavara, C.G.; Levesque, E.; Feray, C.; Compagnon, P.; Azoulay, D. Complications after hepatectomy for hepatocellular carcinoma independently shorten survival: A western, single-center audit. Ann. Surg. Oncol. 2017, 24, 1569–1578. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Liu, K.; Liu, C.; Zhong, Q.; Zhang, J.; Yu, J.; Liang, L.; Li, C.; Wang, M.; Li, Z.; et al. Impact of postoperative infective complications on long-term survival after liver resection for hepatocellular carcinoma. Br. J. Surg. 2019, 106, 1228–1236. [Google Scholar] [CrossRef] [PubMed]
- Wei, T.; Zhang, X.F.; Bagante, F.; Ratti, F.; Marques, H.P.; Silva, S.; Soubrane, O.; Lam, V.; Poultsides, G.A.; Popescu, I.; et al. Postoperative infectious complications worsen long-term survival after curative-intent resection for hepatocellular carcinoma. Ann. Surg. Oncol. 2022, 29, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.-C.; Wu, R.-L.; Liu, F.-B.; Zhao, Y.-J.; Wang, G.-B.; Zhang, Z.-G.; Huang, F.; Xie, K.; Geng, X.-P. A retrospective analysis of long-term outcomes in patients undergoing hepatic resection for large (>5 cm) hepatocellular carcinoma. HPB 2016, 18, 943–949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khandoga, A.; Drefs, M.; Schoenberg, M.; Schiergens, T.; Frenes, K.; Trumm, C.; Angele, M.K.; Guba, M.; Werner, J.; Rentsch, M. Differential significance of early surgical complications for acute and long-term recurrence-free survival following surgical resection of hepatocellular carcinoma: Do comorbidities play a role? Eur. J. Gastroenterol. Hepatol. 2017, 29, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Kong, J.; Li, G.; Chai, J.; Yu, G.; Liu, Y.; Liu, J. Impact of postoperative complications on long-term survival after resection of hepatocellular carcinoma: A systematic review and meta-analysis. Ann. Surg. Oncol. 2021, 28, 8221–8233. [Google Scholar] [CrossRef] [PubMed]
- Arzumanyan, A.; Reis, H.M.; Feitelson, M.A. Pathogenic mechanisms in HBV- and HCV-associated hepatocellular carcinoma. Nat. Rev. Cancer 2013, 13, 123–135. [Google Scholar] [CrossRef]
- Wang, Y.-Y.; Zhong, J.-H.; Su, Z.-Y.; Huang, J.-F.; Lu, S.-D.; Xiang, B.-D.; Ma, L.; Qi, L.-N.; Ou, B.-N.; Li, L.-Q. Albumin-bilirubin versus Child-Pugh score as a predictor of outcome after liver resection for hepatocellular carcinoma. Br. J. Surg. 2016, 103, 725–734. [Google Scholar] [CrossRef]
- Wu, H.-L.; Kuo, H.-C.; Li, C.-C.; Wu, Y.-M.; Lin, S.-P.; Chang, K.-Y.; Hou, M.-C.; Tsou, M.-Y.; Cherng, Y.-G.; Chen, J.-T.; et al. A comparison of prognostic performance of perioperative inflammation markers in surgical resection for hepatocellular carcinoma. J. Chin. Med. Assoc. 2021, 84, 614–622. [Google Scholar] [CrossRef]
- Chang, W.K.; Lee, M.Y.; Tai, Y.H.; Kuo, Y.M.; Tsou, M.Y.; Chang, K.Y. Does epidural analgesia improve the cancer outcome in hepatocellular carcinoma after resection surgery? A retrospective analysis. J. Chin. Med. Assoc. 2019, 82, 295–299. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.L.; Tai, Y.H.; Lin, S.P.; Yang, S.H.; Tsou, M.Y.; Chang, K.Y. Epidural analgesia does not impact recurrence or mortality in patients after rectal cancer resection. Sci. Rep. 2021, 11, 913. [Google Scholar] [CrossRef]
- Tai, Y.H.; Wu, H.L.; Mandell, M.S.; Tsou, M.Y.; Chang, K.Y. The association of allogeneic blood transfusion and the recurrence of hepatic cancer after surgical resection. Anaesthesia 2020, 75, 464–471. [Google Scholar] [CrossRef]
- Tai, Y.H.; Wu, H.L.; Mandell, M.S.; Lin, S.P.; Tsou, M.Y.; Chang, K.Y. The association of non-small cell lung cancer recurrence with allogenic blood transfusion after surgical resection: A propensity score analysis of 1803 patients. Eur. J. Cancer 2020, 140, 45–54. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Pawlik Shindoh, J.; Vauthey, J.N. Liver. In AJCC Cancer Staging Manual., 8th ed.; Amin, M.B., Ed.; AJCC: Chicago, IL, USA, 2017; pp. 287–293. [Google Scholar]
- Iguchi, T.; Aishima, S.; Taketomi, A.; Nishihara, Y.; Fujita, N.; Sanefuji, K.; Maehara, Y.; Tsuneyoshi, M. Extracapsular penetration is a new prognostic factor in human hepatocellular carcinoma. Am. J. Surg. Pathol. 2008, 32, 1675–1682. [Google Scholar] [CrossRef]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [Green Version]
- Sample-Size Determination. In Statistical Methods in Medical Research; Armitage, P.; Berry, G.; Matthews, J.N.S. (Eds.) Blackwell Science: Malden, MA, USA, 2002; pp. 137–146. [Google Scholar]
- Thoemmes, F.; Ong, A.D. A primer on inverse probability of treatment weighting and marginal structural models. Emerg. Adulthood. 2016, 4, 40–59. [Google Scholar] [CrossRef] [Green Version]
- Cata, J.P.; Wang, H.; Gottumukkala, V.; Reuben, J.; Sessler, D.I. Inflammatory response, immunosuppression, and cancer recurrence after perioperative blood transfusions. Br. J. Anaesth. 2013, 110, 690–701. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.G.; Wang, P.; Wang, B.; Fu, Z.J.; Zhao, W.J.; Yan, S.L. Diabetes mellitus and poorer prognosis in hepatocellular carcinoma: A systematic review and meta-analysis. PLoS ONE 2014, 9, e95485. [Google Scholar] [CrossRef] [Green Version]
- Hosokawa, T.; Kurosaki, M.; Tsuchiya, K.; Matsuda, S.; Muraoka, M.; Suzuki, Y.; Tamaki, N.; Yasui, Y.; Nakata, T.; Nishimura, T.; et al. Hyperglycemia is a significant prognostic factor of hepatocellular carcinoma after curative therapy. World J. Gastroenterol. 2013, 19, 249–257. [Google Scholar] [CrossRef]
- Ripollés-Melchor, J.; Ramírez-Rodríguez, J.M.; Casans-Francés, R.; Aldecoa, C.; Abad-Motos, A.; Logroño-Egea, M.; García-Erce, J.A.; Camps-Cervantes, Á.; Ferrando-Ortolá, C.; de la Rica, A.S.; et al. Association between use of enhanced recovery after surgery protocol and postoperative complications in colorectal surgery: The Postoperative Outcomes Within Enhanced Recovery After Surgery Protocol (POWER) study. JAMA Surg. 2019, 154, 725–736. [Google Scholar] [CrossRef] [PubMed]
- Pisarska, M.; Torbicz, G.; Gajewska, N.; Rubinkiewicz, M.; Wierdak, M.; Major, P.; Budzyński, A.; Ljungqvist, O.; Pędziwiatr, M. Compliance with the ERAS protocol and 3-year survival after laparoscopic surgery for non-metastatic colorectal cancer. World J. Surg. 2019, 43, 2552–2560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pang, Q.; Duan, L.; Jiang, Y.; Liu, H. Oncologic and long-term outcomes of enhanced recovery after surgery in cancer surgeries—A systematic review. World J. Surg. Oncol. 2021, 19, 191. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Clymer, J.W.; Chen, B.P.-H.; Sadeghirad, B.; Ferko, N.C.; Cameron, C.G.; Hinoul, P. Prolonged operative duration is associated with complications: A systematic review and meta-analysis. J. Surg. Res. 2018, 229, 134–144. [Google Scholar] [CrossRef] [Green Version]
- Villanueva, A. Hepatocellular carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| CD Grade ≥ III (n = 93) | CD Grade (0–II) (n = 1326) | p | |
|---|---|---|---|
| Age, year | 63.7 ± 12.2 | 61.0 ± 12.9 | 0.0488 |
| Sex, male | 66 (71.0%) | 1018 (76.8%) | 0.2026 |
| ASA class ≥ 3 | 42 (45.2%) | 378 (28.5%) | 0.0007 |
| Aetiology of HCC | |||
| HBsAg-positive | 58 (62.4%) | 894 (67.4%) | 0.3159 |
| Anti-HCV Ab-positive | 20 (21.5%) | 289 (21.8%) | 0.9479 |
| Alcoholism | 8 (8.6%) | 94 (7.1%) | 0.5850 |
| Liver cirrhosis | 45 (48.4%) | 573 (43.2%) | 0.3306 |
| Child–Pugh classification | 0.5851 | ||
| Class A | 41 (44.1%) | 530 (40.0%) | |
| Class B | 4 (4.3%) | 43 (3.2%) | |
| Clinically significant portal hypertension | 9 (9.7%) | 129 (9.7%) | 0.9872 |
| Oesophageal varices | 9 (9.7%) | 74 (5.6%) | 0.1036 |
| Diabetes mellitus | 42 (45.2%) | 298 (22.5%) | <0.0001 |
| Chronic kidney disease | 11 (11.8%) | 124 (9.4%) | 0.4314 |
| Preoperative laboratory tests | |||
| Haemoglobin, g·dL−1 | 13.1 ± 1.7 | 13.4 ± 1.7 | 0.1929 |
| Platelet count, 103·μL−1 | 176.8 ± 78.9 | 179.5 ± 78.4 | 0.7501 |
| Thrombocytopenia | 34 (36.6%) | 531 (40.1%) | 0.5068 |
| International normalised ratio | 1.05 ± 0.07 | 1.07 ± 0.82 | 0.3066 |
| Total bilirubin ≥ 1.0 mg·dL−1 | 24 (25.8%) | 298 (22.5%) | 0.4630 |
| AST > 40 IU·L−1 | 57 (61.3%) | 593 (44.9%) | 0.0022 |
| ALT > 40 IU·L−1 | 51 (54.8%) | 623 (47.0%) | 0.1425 |
| Alpha-fetoprotein > 20 ng·mL−1 | 44 (48.9%) | 655 (50.8%) | 0.7239 |
| Albumin ≤ 3.5 g·dL−1 | 12 (13.0%) | 95 (7.2%) | 0.0421 |
| Serum creatinine, mg·dL−1 | 0.99 ± 0.72 | 1.02 ± 0.83 | 0.7167 |
| BCLC stage | 0.0284 | ||
| Stage 0 | 8 (8.6%) | 180 (13.6%) | |
| Stage A | 33 (35.5%) | 589 (44.4%) | |
| Stage B | 52 (55.9%) | 557 (42.0%) | |
| Pathologic characteristics | |||
| Tumour diameter > 5 cm | 38 (40.9%) | 479 (36.1%) | 0.3589 |
| Multifocal cancer | 36 (38.7%) | 273 (20.6%) | <0.0001 |
| Poor or undifferentiated histology | 30 (32.3%) | 468 (35.3%) | 0.7674 |
| Microvascular invasion | 65 (69.9%) | 906 (68.3%) | 0.7534 |
| Extracapsular invasion | 33 (35.5%) | 563 (42.5%) | 0.1877 |
| Positive surgical margin | 10 (10.8%) | 78 (5.9%) | 0.0598 |
| Preoperative TACE/RFA/PEI | 9 (9.7%) | 117 (8.8%) | 0.7796 |
| Surgical and anaesthetic management | |||
| Hepatectomy > 2 segments | 49 (52.7%) | 463 (34.9%) | 0.0006 |
| Laparoscopic or robotic surgery | 4 (4.3%) | 83 (6.3%) | 0.4467 |
| Epidural analgesia | 35 (37.6%) | 509 (38.4%) | 0.8854 |
| Intraoperative blood loss, mL | 1050 (600–2100) | 600 (300–1150) | <0.0001 |
| Blood transfusion rate | 81 (87.1%) | 799 (60.3%) | <0.0001 |
| Anaesthesia duration, min | 420 (315–540) | 335 (285–420) | <0.0001 |
| Operation period (2011–2016) | 54 (58.1%) | 691 (52.1%) | 0.2664 |
| Clavien–Dindo Grade III | Count (Percentage) † |
|---|---|
| Bile leakage | 30 (35%) |
| Pleural effusion | 16 (19%) |
| Wound complication | 12 (14%) |
| Intra-abdominal abscess | 8 (9%) |
| Massive ascites | 4 (5%) |
| Hepatic haemorrhage | 4 (5%) |
| Obstructive jaundice | 2 (2%) |
| Liver abscess | 2 (2%) |
| Pneumothorax | 2 (2%) |
| Occlusion of common hepatic duct | 1 (1%) |
| Oedematous change of bile duct wall | 1 (1%) |
| Peritonitis | 1 (1%) |
| Duodenal ulcer bleeding | 1 (1%) |
| Intestinal obstruction | 1 (1%) |
| Acute kidney injury | 1 (1%) |
| Clavien–Dindo Grade IV | Count (Percentage) |
| Respiratory failure | 13 (62%) |
| Cerebral infarction | 2 (10%) |
| Sepsis | 2 (10%) |
| Multiorgan failure | 2 (10%) |
| Hepatic failure | 1 (5%) |
| Myocardial infarction | 1 (5%) |
| All-Cause Mortality | Cancer-Specific Mortality | Cancer Recurrence | ||||
|---|---|---|---|---|---|---|
| cHR (95% CI) | p | cHR (95% CI) | p | cHR (95% CI) | p | |
| Clavien–Dindo grade ≥ III vs. controls | 1.72 (1.16–2.55) | 0.0069 | 1.35 (0.85–2.15) | 0.2081 | 1.15 (0.87–1.52) | 0.3307 |
| Age, year | 1.01 (1.00–1.02) | 0.0392 | 1.01 (1.00–1.02) | 0.1303 | 1.00 (1.00–1.01) | 0.2228 |
| Sex, male | 1.04 (0.80–1.36) | 0.7479 | 1.02 (0.77–1.34) | 0.9093 | 1.08 (0.92–1.27) | 0.3644 |
| ASA class ≥ 3 | 1.24 (0.98–1.57) | 0.0737 | 1.18 (0.92–1.52) | 0.2016 | 1.07 (0.92–1.24) | 0.3653 |
| HBsAg-positive | 1.00 (0.79–1.26) | 0.9694 | 1.03 (0.80–1.32) | 0.8221 | 1.10 (0.95–1.28) | 0.1866 |
| Anti-HCV Ab-positive | 1.09 (0.84–1.42) | 0.4963 | 1.02 (0.77–1.35) | 0.8773 | 1.16 (0.99–1.36) | 0.0625 |
| Alcoholism | 0.79 (0.49–1.26) | 0.3184 | 0.84 (0.52–1.38) | 0.4970 | 0.88 (0.68–1.15) | 0.3593 |
| Liver cirrhosis | 1.62 (1.30–2.01) | <0.0001 | 1.63 (1.29–2.05) | <0.0001 | 1.38 (1.21–1.58) | <0.0001 |
| Child–Pugh class B | 2.32 (1.53–3.52) | <0.0001 | 2.29 (1.47–3.57) | 0.0003 | 1.74 (1.25–2.43) | 0.0009 |
| Clinically significant portal hypertension | 1.85 (1.37–2.52) | <0.0001 | 1.90 (1.38–2.62) | <0.0001 | 1.56 (1.26–1.93) | <0.0001 |
| Oesophageal varices | 2.31 (1.61–3.31) | <0.0001 | 2.39 (1.64–3.49) | <0.0001 | 1.53 (1.17–2.02) | 0.0022 |
| Diabetes mellitus | 1.42 (1.12–1.81) | 0.0040 | 1.35 (1.04–1.75) | 0.0226 | 1.11 (0.95–1.29) | 0.1988 |
| Chronic kidney disease | 1.64 (1.20–2.23) | 0.0018 | 1.43 (1.02–2.02) | 0.0410 | 0.95 (0.75–1.20) | 0.6496 |
| Haemoglobin, g·dL−1 | 0.88 (0.83–0.94) | <0.0001 | 0.89 (0.84–0.96) | 0.0009 | 0.96 (0.93–1.00) | 0.0470 |
| Platelet count, 103·μL−1 | 1.00 (1.00–1.00) | 0.8567 | 1.00 (1.00–1.00) | 0.7302 | 1.00 (1.00–1.00) | 0.8497 |
| Thrombocytopenia | 1.15 (0.92–1.44) | 0.2092 | 1.14 (0.90–1.44) | 0.2878 | 1.13 (0.99–1.30) | 0.0790 |
| International normalised ratio | 1.09 (1.02–1.16) | 0.0103 | 1.09 (1.01–1.17) | 0.0265 | 1.04 (0.98–1.11) | 0.2155 |
| Total bilirubin ≥ 1.0 mg·dL−1 | 1.36 (1.06–1.73) | 0.0141 | 1.44 (1.11–1.85) | 0.0056 | 1.09 (0.93–1.28) | 0.3000 |
| AST > 40 IU·L−1 | 1.98 (1.59–2.47) | <0.0001 | 2.05 (1.62–2.59) | <0.0001 | 1.71 (1.50–1.96) | <0.0001 |
| ALT > 40 IU·L−1 | 1.19 (0.96–1.48) | 0.1137 | 1.26 (1.00–1.59) | 0.0482 | 1.24 (1.09–1.42) | 0.0015 |
| Alpha-fetoprotein > 20 ng·mL−1 | 1.62 (1.29–2.02) | <0.0001 | 1.75 (1.38–2.23) | <0.0001 | 1.63 (1.42–1.86) | <0.0001 |
| Albumin ≤ 3.5 g·dL−1 | 1.74 (1.19–2.54) | 0.0040 | 1.65 (1.09–2.49) | 0.0180 | 1.48 (1.16–1.88) | 0.0013 |
| Serum creatinine, mg·dL−1 | 1.08 (0.96–1.21) | 0.2076 | 1.01 (0.85–1.19) | 0.9380 | 0.98 (0.89–1.07) | 0.6319 |
| BCLC stage | <0.0001 | <0.0001 | <0.0001 | |||
| Stage A vs. 0 | 1.27 (0.85–1.90) | 0.2529 | 1.40 (0.90–2.19) | 0.1410 | 1.28 (1.01–1.61) | 0.0382 |
| Stage B vs. 0 | 2.57 (1.75–3.79) | <0.0001 | 2.89 (1.88–4.44) | <0.0001 | 2.03 (1.62–2.54) | <0.0001 |
| Tumour diameter > 5 cm | 2.13 (1.72–2.65) | <0.0001 | 2.18 (1.73–2.75) | <0.0001 | 1.56 (1.36–1.79) | <0.0001 |
| Multifocal cancer | 1.57 (1.23–2.00) | 0.0003 | 1.58 (1.22–2.04) | 0.0006 | 1.80 (1.55–2.09) | <0.0001 |
| Poor or undifferentiated histology | 1.37 (1.10–1.72) | 0.0057 | 1.46 (1.15–1.85) | 0.0018 | 1.43 (1.25–1.64) | <0.0001 |
| Microvascular invasion | 1.96 (1.52–2.52) | <0.0001 | 2.24 (1.70–2.97) | <0.0001 | 1.71 (1.47–1.99) | <0.0001 |
| Extracapsular invasion | 1.36 (1.09–1.69) | 0.0057 | 1.39 (1.10–1.75) | 0.0054 | 1.29 (1.13–1.48) | 0.0002 |
| Positive surgical margin | 2.79 (1.96–3.99) | <0.0001 | 2.80 (1.92–4.09) | <0.0001 | 2.13 (1.65–2.76) | <0.0001 |
| Preoperative TACE/RFA/PEI | 1.49 (1.06–2.10) | 0.0222 | 1.61 (1.13–2.30) | 0.0080 | 1.23 (0.98–1.54) | 0.0806 |
| Hepatectomy > 2 segments | 1.51 (1.22–1.88) | 0.0002 | 1.55 (1.23–1.95) | 0.0002 | 1.27 (1.11–1.46) | 0.0007 |
| Laparoscopic or robotic surgery | 0.58 (0.30–1.13) | 0.1082 | 0.66 (0.34–1.29) | 0.2261 | 0.77 (0.57–1.06) | 0.1098 |
| Epidural blockade | 1.05 (0.85–1.31) | 0.6367 | 1.04 (0.82–1.31) | 0.7487 | 1.04 (0.91–1.20) | 0.5363 |
| Intraoperative blood loss, mL † | 1.35 (1.24–1.47) | <0.0001 | 1.36 (1.24–1.49) | <0.0001 | 1.23 (1.17–1.30) | <0.0001 |
| Blood transfusion rate | 2.45 (1.90–3.17) | <0.0001 | 2.68 (2.02–3.54) | <0.0001 | 1.64 (1.42–1.90) | <0.0001 |
| Anaesthesia duration, min † | 1.94 (1.51–2.49) | <0.0001 | 1.97 (1.51–2.57) | <0.0001 | 1.59 (1.36–1.85) | <0.0001 |
| Operation period (2011–2016 vs. 2005–2010) | 0.69 (0.54–0.88) | 0.0024 | 0.70 (0.54–0.90) | 0.0059 | 0.82 (0.72–0.95) | 0.0055 |
| OR | 95% CI | p | |
|---|---|---|---|
| Sex, male vs. female | 0.48 | 0.28–0.84 | 0.0102 |
| Diabetes mellitus | 2.76 | 1.66–4.57 | 0.0001 |
| Clinically significant portal hypertension | 0.25 | 0.08–0.79 | 0.0177 |
| Oesophageal varices | 3.19 | 1.26–8.09 | 0.0144 |
| Multifocal cancer | 2.18 | 1.30–3.67 | 0.0033 |
| Intraoperative blood loss, mL † | 1.61 | 1.29–2.02 | <0.0001 |
| Anaesthesia duration, min † | 2.35 | 1.25–4.40 | 0.0077 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuo, C.-W.; Wu, H.-L.; Li, C.-C.; Cata, J.P.; Liu, H.-Y.; Hou, M.-C.; Cherng, Y.-G.; Tai, Y.-H. Long-Term Survival Impact of High-Grade Complications after Liver Resection for Hepatocellular Carcinoma: A Retrospective Single-Centre Cohort Study. Medicina 2022, 58, 534. https://doi.org/10.3390/medicina58040534
Kuo C-W, Wu H-L, Li C-C, Cata JP, Liu H-Y, Hou M-C, Cherng Y-G, Tai Y-H. Long-Term Survival Impact of High-Grade Complications after Liver Resection for Hepatocellular Carcinoma: A Retrospective Single-Centre Cohort Study. Medicina. 2022; 58(4):534. https://doi.org/10.3390/medicina58040534
Chicago/Turabian StyleKuo, Chin-Wen, Hsiang-Ling Wu, Chun-Cheng Li, Juan P. Cata, Hsin-Yi Liu, Ming-Chih Hou, Yih-Giun Cherng, and Ying-Hsuan Tai. 2022. "Long-Term Survival Impact of High-Grade Complications after Liver Resection for Hepatocellular Carcinoma: A Retrospective Single-Centre Cohort Study" Medicina 58, no. 4: 534. https://doi.org/10.3390/medicina58040534