
Extracorporeal Cardiopulmonary Resuscitation: A Narrative Review and Establishment of a Sustainable Program
 , , , ,
, , , , {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Cardiac Arrest
3. ECPR for In-Hospital Cardiac Arrest
4. ECPR for Out-of-Hospital Cardiac Arrest
5. ECPR Program Development
5.1. Community Approach to OHCA
5.2. Simulation
6. ECPR Program Deployment
6.1. Prehospital Candidate Patient Identification and Transport
6.2. Hospital-Based Consult and Activation Process
6.3. Mechanical Compression Devices
6.4. Hospital Arrival
6.5. Equipment and Cannulation
6.6. Ongoing Resuscitation
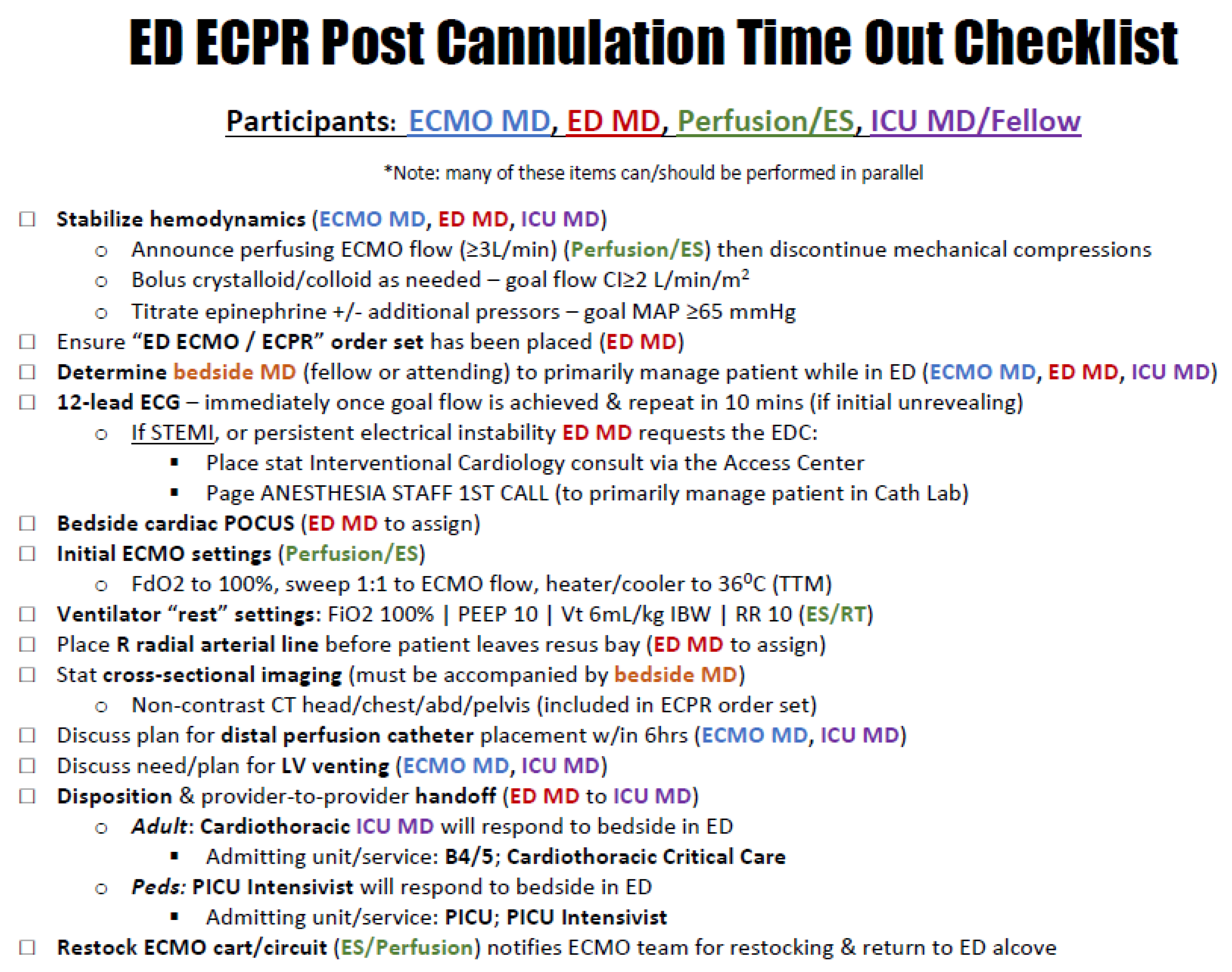
6.7. Immediate Post-Cannulation Diagnostics and Therapeutics
6.8. Cardiac Catheterization Lab
7. ECPR Quality Improvement and Patient Safety (QI/PS)
7.1. ECPR Registry Maintenance and Participation
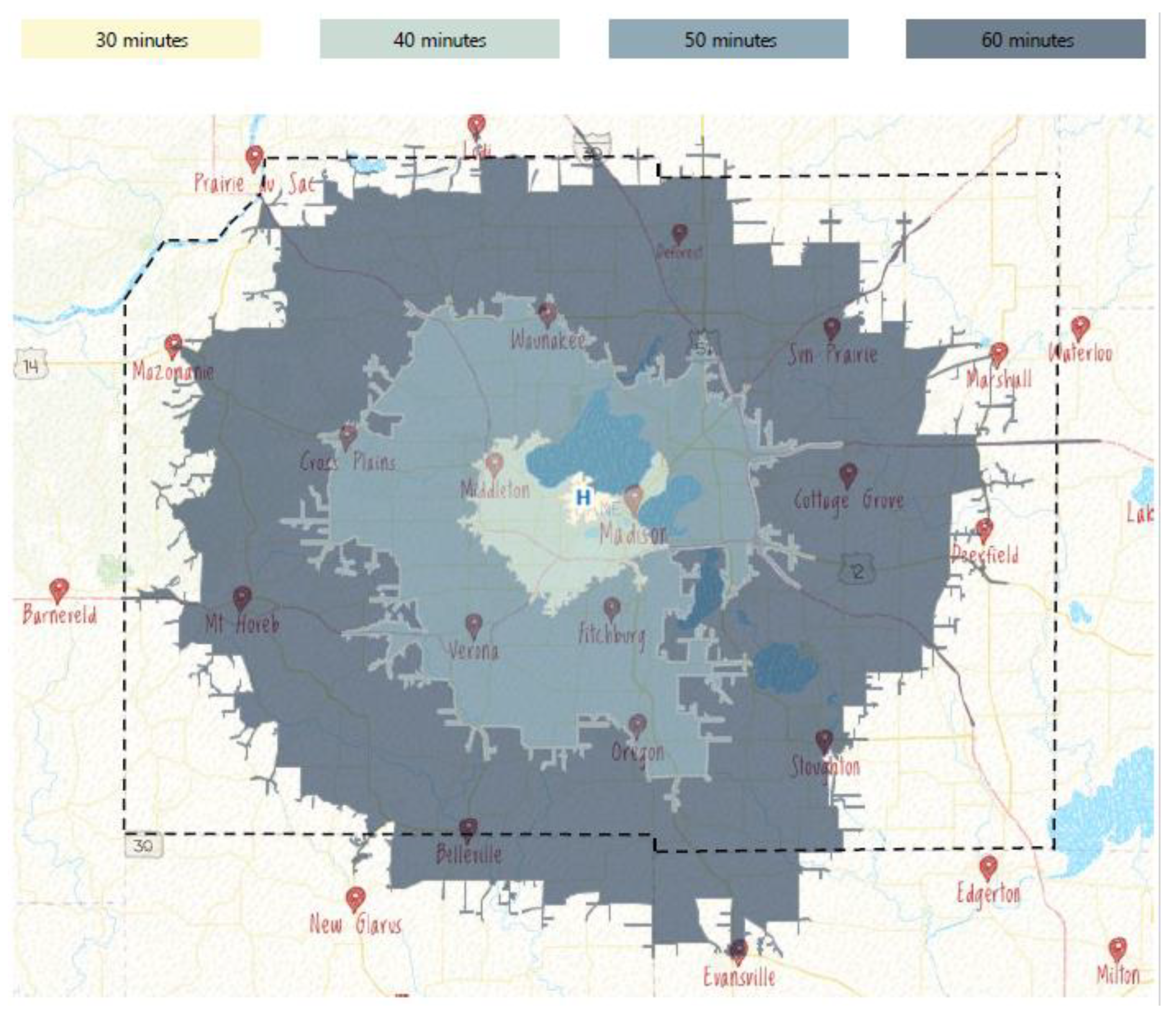
7.2. Geospatial Mapping
7.3. Multidisciplinary QI
8. Post-Cannulation ICU Management
8.1. Coronary Imaging and Intervention
8.2. Temperature
8.3. Blood Pressure
8.4. Anticoagulation
8.5. Left Ventricular Venting
8.6. Limb Ischemia
8.7. Prognostication of Neurologic Recovery
9. Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef] [PubMed]
- Spangenberg, T.; Schewel, J.; Dreher, A.; Meincke, F.; Bahlmann, E.; van der Schalk, H.; Kreidel, F.; Frerker, C.; Stoeck, M.; Bein, B.; et al. Health related quality of life after extracorporeal cardiopulmonary resuscitation in refractory cardiac arrest. Resuscitation 2018, 127, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, I.; Nadkarni, V.; Bahr, J.; Berg, R.A.; Billi, J.E.; Bossaert, L.; Cassan, P.; Coovadia, A.; D’Este, K.; Finn, J.; et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: Update and simplification of the Utstein templates for resuscitation registries: A statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Councils of Southern Africa). Circulation 2004, 110, 3385–3397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haywood, K.; Whitehead, L.; Nadkarni, V.M.; Achana, F.; Beesems, S.; Böttiger, B.W.; Brooks, A.; Castrén, M.; Ong, M.E.; Hazinski, M.F.; et al. COSCA (Core Outcome Set for Cardiac Arrest) in Adults: An Advisory Statement From the International Liaison Committee on Resuscitation. Circulation 2018, 137, e783–e801. [Google Scholar] [CrossRef] [PubMed]
- Parnia, S.; Yang, J.; Nguyen, R.; Ahn, A.; Zhu, J.; Inigo-Santiago, L.; Nasir, A.; Golder, K.; Ravishankar, S.; Bartlett, P.; et al. Cerebral Oximetry During Cardiac Arrest: A Multicenter Study of Neurologic Outcomes and Survival. Crit. Care Med. 2016, 44, 1663–1674. [Google Scholar] [CrossRef]
- Roellke, E.; Parnia, S.; Patel, J.; Friedman, S.; Mengotto, A. The impact of extracorporeal membrane oxygenation on cerebral oxygen delivery during cardiac arrest: A case series. Resusc. Plus 2021, 5, 100068. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, C.-S.; Yuan, X.-L.; Ling, J.-Y.; Zhang, Q.; Liang, Y.; Liu, B.; Zhao, L.-X. ECMO attenuates inflammation response and increases ATPase activity in brain of swine model with cardiac arrest compared with CCPR. Biosci. Rep. 2019, 39, BSR20182463. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-S.; Lin, J.-W.; Yu, H.-Y.; Ko, W.-J.; Jerng, J.-S.; Chang, W.-T.; Chen, W.-J.; Huang, S.-C.; Chi, N.-H.; Wang, C.-H.; et al. Cardiopulmonary resuscitation with assisted extracorporeal life-support versus conventional cardiopulmonary resuscitation in adults with in-hospital cardiac arrest: An observational study and propensity analysis. Lancet 2008, 372, 554–561. [Google Scholar] [CrossRef]
- Kim, S.J.; Kim, H.J.; Lee, H.Y.; Ahn, H.S.; Lee, S.W. Comparing extracorporeal cardiopulmonary resuscitation with conventional cardiopulmonary resuscitation: A meta-analysis. Resuscitation 2016, 103, 106–116. [Google Scholar] [CrossRef]
- Downing, J.; Al Falasi, R.; Cardona, S.; Fairchild, M.; Lowie, B.; Chan, C.; Powell, E.; Pourmand, A.; Tran, Q.K. How effective is extracorporeal cardiopulmonary resuscitation (ECPR) for out-of-hospital cardiac arrest? A systematic review and meta-analysis. Am. J. Emerg. Med. 2022, 51, 127–138. [Google Scholar] [CrossRef]
- Granfeldt, A.; Holmberg, M.J.; Donnino, M.W.; Andersen, L.W.; the CARES Surveillance Group. 2015 Guidelines for Cardiopulmonary Resuscitation and survival after adult and paediatric out-of-hospital cardiac arrest. Eur. Heart J. Qual. Care Clin. Outcomes 2021, 7, 407–415. [Google Scholar] [CrossRef]
- Kagawa, E. Extracorporeal cardiopulmonary resuscitation for adult cardiac arrest patients. World J. Crit. Care Med. 2012, 1, 46–49. [Google Scholar] [CrossRef] [Green Version]
- Lamhaut, L.; Hutin, A.; Puymirat, E.; Jouan, J.; Raphalen, J.-H.; Jouffroy, R.; Jaffry, M.; Dagron, C.; An, K.; Dumas, F.; et al. A Pre-Hospital Extracorporeal Cardio Pulmonary Resuscitation (ECPR) strategy for treatment of refractory out hospital cardiac arrest: An observational study and propensity analysis. Resuscitation 2017, 117, 109–117. [Google Scholar] [CrossRef] [Green Version]
- Avalli, L.; Maggioni, E.; Formica, F.; Redaelli, G.; Migliari, M.; Scanziani, M.; Celotti, S.; Coppo, A.; Caruso, R.; Ristagno, G.; et al. Favourable survival of in-hospital compared to out-of-hospital refractory cardiac arrest patients treated with extracorporeal membrane oxygenation: An Italian tertiary care centre experience. Resuscitation 2012, 83, 579–583. [Google Scholar] [CrossRef]
- Pozzi, M.; Koffel, C.; Armoiry, X.; Pavlakovic, I.; Neidecker, J.; Prieur, C.; Bonnefoy, E.; Robin, J.; Obadia, J.-F. Extracorporeal life support for refractory out-of-hospital cardiac arrest: Should we still fight for? A single-centre, 5-year experience. Int. J. Cardiol. 2016, 204, 70–76. [Google Scholar] [CrossRef]
- Yannopoulos, D.; Bartos, J.A.; Raveendran, G.; Conterato, M.; Frascone, R.J.; Trembley, A.; John, R.; Connett, J.; Benditt, D.G.; Lurie, K.G.; et al. Coronary Artery Disease in Patients With Out-of-Hospital Refractory Ventricular Fibrillation Cardiac Arrest. J. Am. Coll. Cardiol. 2017, 70, 1109–1117. [Google Scholar] [CrossRef]
- Stub, D.; Bernard, S.; Pellegrino, V.; Smith, K.; Walker, T.; Sheldrake, J.; Hockings, L.; Shaw, J.; Duffy, S.J.; Burrell, A.; et al. Refractory cardiac arrest treated with mechanical CPR, hypothermia, ECMO and early reperfusion (the CHEER trial). Resuscitation 2015, 86, 88–94. [Google Scholar] [CrossRef]
- Leick, J.; Liebetrau, C.; Szardien, S.; Fischer-Rasokat, U.; Willmer, M.; Van Linden, A.; Blumenstein, J.; Nef, H.; Rolf, A.; Arlt, M.; et al. Door-to-implantation time of extracorporeal life support systems predicts mortality in patients with out-of-hospital cardiac arrest. Clin. Res. Cardiol. 2013, 102, 661–669. [Google Scholar] [CrossRef]
- Maekawa, K.; Tanno, K.; Hase, M.; Mori, K.; Asai, Y. Extracorporeal Cardiopulmonary Resuscitation for Patients With Out-of-Hospital Cardiac Arrest of Cardiac Origin: A propensity-matched study and predictor analysis. Crit. Care Med. 2013, 41, 1186–1196. [Google Scholar] [CrossRef]
- Yannopoulos, D.; Bartos, J.; Raveendran, G.; Walser, E.; Connett, J.; A Murray, T.; Collins, G.; Zhang, L.; Kalra, R.; Kosmopoulos, M.; et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): A phase 2, single centre, open-label, randomised controlled trial. Lancet 2020, 396, 1807–1816. [Google Scholar] [CrossRef]
- Belohlavek, J.; Smalcova, J.; Rob, D.; Franek, O.; Smid, O.; Pokorna, M.; Horák, J.; Mrazek, V.; Kovarnik, T.; Zemanek, D.; et al. Effect of Intra-arrest Transport, Extracorporeal Cardiopulmonary Resuscitation, and Immediate Invasive Assessment and Treatment on Functional Neurologic Outcome in Refractory Out-of-Hospital Cardiac Arrest: A Randomized Clinical Trial. JAMA 2022, 327, 737–747. [Google Scholar] [CrossRef] [PubMed]
- Massion, P.B.; Joachim, S.; Morimont, P.; Dulière, G.; Betz, R.; Benoit, A.; Amabili, P.; Lagny, M.; Lizin, J.; Np, A.M.; et al. Feasibility of extracorporeal membrane oxygenation cardiopulmonary resuscitation by low volume centers in Belgium. J. Am. Coll. Emerg. Physicians Open 2021, 2, e12484. [Google Scholar] [CrossRef] [PubMed]
- Richardson, A.C.; Tonna, J.E.; Nanjayya, V.; Nixon, P.; Abrams, D.C.; Raman, L.; Bernard, S.; Finney, S.J.; Grunau, B.; Youngquist, S.T.; et al. Extracorporeal Cardiopulmonary Resuscitation in Adults. Interim Guideline Consensus Statement From the Extracorporeal Life Support Organization. ASAIO J. 2021, 67, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Grunau, B.; Kime, N.; Leroux, B.; Rea, T.; Van Belle, G.; Menegazzi, J.J.; Kudenchuk, P.J.; Vaillancourt, C.; Morrison, L.J.; Elmer, J.; et al. Association of Intra-arrest Transport vs Continued On-Scene Resuscitation With Survival to Hospital Discharge Among Patients With Out-of-Hospital Cardiac Arrest. JAMA 2020, 324, 1058–1067. [Google Scholar] [CrossRef] [PubMed]
- Sip, M.; Puslecki, M.; Dabrowski, M.; Klosiewicz, T.; Zalewski, R.; Ligowski, M.; Goszczynska, E.; Paprocki, C.; Grygier, M.; Lesiak, M.; et al. Extended cardiopulmonary resuscitation: From high fidelity simulation scenario to the first clinical applications in Poznan out-of-hospital cardiac arrest program. Perfusion 2022, 37, 46–55. [Google Scholar] [CrossRef]
- Chonde, M.; Escajeda, J.; Elmer, J.; Callaway, C.W.; Guyette, F.X.; Boujoukos, A.; Sappington, P.L.; Smith, A.J.; Schmidhofer, M.; Sciortino, C.; et al. Challenges in the development and implementation of a healthcare system based extracorporeal cardiopulmonary resuscitation (ECPR) program for the treatment of out of hospital cardiac arrest. Resuscitation 2020, 148, 259–265. [Google Scholar] [CrossRef] [Green Version]
- Grunau, B.; Carrier, S.; Bashir, J.; Dick, W.; Harris, L.; Boone, R.; Kalla, D.; Scheuermeyer, F.; Twaites, B.; Straight, R.; et al. A comprehensive regional clinical and educational ECPR protocol decreases time to ECMO in patients with refractory out-of-hospital cardiac arrest. Can. J. Emerg. Med. 2017, 19, 424–433. [Google Scholar] [CrossRef] [Green Version]
- Stampfl, M.; McCarthy, D.; Koch, J.; Lohmeier, M.; Anderson, E.; Glazer, J. 1365: On-Scene Resuscitation Time is Highly Correlated with Neuro-Intact Survival For ECPR. Crit. Care Med. 2022, 50, 684. [Google Scholar] [CrossRef]
- Grunau, B.; Reynolds, J.; Scheuermeyer, F.; Stenstom, R.; Stub, D.; Pennington, S.; Cheskes, S.; Ramanathan, K.; Christenson, J. Relationship between Time-to-ROSC and Survival in Out-of-hospital Cardiac Arrest ECPR Candidates: When is the Best Time to Consider Transport to Hospital? Prehosp. Emerg. Care 2016, 20, 615–622. [Google Scholar] [CrossRef]
- Stampfl, M.; McCarthy, D.; Koch, J.; Long, M.; Glazer, J. 1371: Novel Tool for ECPR Consult, Activation, And Automated Repository Generation. Crit. Care Med. 2022, 50, 687. [Google Scholar] [CrossRef]
- Rubertsson, S.; Silfverstolpe, J.; Rehn, L.; Nyman, T.; Lichtveld, R.; Boomars, R.; Bruins, W.; Ahlstedt, B.; Puggioli, H.; Lindgren, E.; et al. The Study Protocol for the LINC (LUCAS in Cardiac Arrest) Study: A study comparing conventional adult out-of-hospital cardiopulmonary resuscitation with a concept with mechanical chest compressions and simultaneous defibrillation. Scand. J. Trauma Resusc. Emerg. Med. 2013, 21, 5. [Google Scholar] [CrossRef] [Green Version]
- Tonna, J.E.; Selzman, C.H.; Mallin, M.P.; Smith, B.R.; Youngquist, S.T.; Koliopoulou, A.; Welt, F.; Stoddard, K.D.; Nirula, R.; Barton, R.; et al. Development and Implementation of a Comprehensive, Multidisciplinary Emergency Department Extracorporeal Membrane Oxygenation Program. Ann. Emerg. Med. 2017, 70, 32–40. [Google Scholar] [CrossRef]
- Nee, J.; Koerner, R.; Zickler, D.; Schroeder, T.; Enghard, P.; Nibbe, L.; Hasper, D.; Buder, R.; Leithner, C.; Ploner, C.J.; et al. Establishment of an extracorporeal cardio-pulmonary resuscitation program in Berlin—Outcomes of 254 patients with refractory circulatory arrest. Scand. J. Trauma Resusc. Emerg. Med. 2020, 28, 96. [Google Scholar] [CrossRef]
- Djordjevic, I.; Gaisendrees, C.; Adler, C.; Eghbalzadeh, K.; Braumann, S.; Ivanov, B.; Merkle, J.; Deppe, A.-C.; Kuhn, E.; Stangl, R.; et al. Extracorporeal cardiopulmonary resuscitation for out-of-hospital cardiac arrest: First results and outcomes of a newly established ECPR program in a large population area. Perfusion 2022, 37, 249–256. [Google Scholar] [CrossRef]
- Schmitzberger, F.F.; Haas, N.L.; Coute, R.A.; Bartos, J.; Hackmann, A.; Haft, J.W.; Hsu, C.H.; Hutin, A.; Lamhaut, L.; Marinaro, J.; et al. ECPR. Resuscitation 2022, 179, 214–220. [Google Scholar] [CrossRef]
- Whitmore, S.P.; Gunnerson, K.J.; Haft, J.W.; Lynch, W.R.; VanDyck, T.; Hebert, C.; Waldvogel, J.; Havey, R.; Weinberg, A.; Cranford, J.A.; et al. Simulation training enables emergency medicine providers to rapidly and safely initiate extracorporeal cardiopulmonary resuscitation (ECPR) in a simulated cardiac arrest scenario. Resuscitation 2019, 138, 68–73. [Google Scholar] [CrossRef]
- Hutin, A.; Ricard-Hibon, A.; Briole, N.; Dupin, A.; Dagron, C.; Raphalen, J.H.; Mungur, A.; An, K.; Carli, P.; Lamhaut, L. First Description of a Helicopter-Borne ECPR Team for Remote Refractory Out-of-Hospital Cardiac Arrest. Prehosp. Emerg. Care 2021, 26, 89–92. [Google Scholar] [CrossRef]
- Spigner, M.; Braude, D.; Pruett, K.; Ortiz, C.; Glazer, J.; Marinaro, J. The Use of Predictive Modeling to Compare Prehospital eCPR Strategies. Prehosp. Emerg. Care 2022, 1–8. [Google Scholar] [CrossRef]
- Bartos, J.A.; Frascone, R.; Conterato, M.; Wesley, K.; Lick, C.; Sipprell, K.; Vuljaj, N.; Burnett, A.; Peterson, B.K.; Simpson, N.; et al. The Minnesota mobile extracorporeal cardiopulmonary resuscitation consortium for treatment of out-of-hospital refractory ventricular fibrillation: Program description, performance, and outcomes. EClinicalMedicine 2020, 29–30, 100632. [Google Scholar] [CrossRef]
- Danial, P.; Hajage, D.; Nguyen, L.S.; Mastroianni, C.; Demondion, P.; Schmidt, M.; Bouglé, A.; Amour, J.; Leprince, P.; Combes, A.; et al. Percutaneous versus surgical femoro-femoral veno-arterial ECMO: A propensity score matched study. Intensiv. Care Med. 2018, 44, 2153–2161. [Google Scholar] [CrossRef]
- Grasselli, G.; Pesenti, A.; Marcolin, R.; Patroniti, N.; Isgró, S.; Tagliabue, P.; Lucchini, A.; Fumagalli, R. Percutaneous Vascular Cannulation for Extracorporeal Life Support (ECLS): A Modified Technique. Int. J. Artif. Organs 2010, 33, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, R.H. Physiology of Gas Exchange During ECMO for Respiratory Failure. J. Intensiv. Care Med. 2017, 32, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Brogan, T.V.; Lequier, L.; Lorusso, R.; MacLaren, G.; Peek, G. (Eds.) Extracorporeal Life Support Organization, issuing body. In Extracorporeal Life Support: The ELSO Red Book, 5th ed.; Extracorporeal Life Support Organization: Ann Arbor, MI, USA, 2017. [Google Scholar]
- Nielsen, N.; Wetterslev, J.; Cronberg, T.; Erlinge, D.; Gasche, Y.; Hassager, C.; Horn, J.; Hovdenes, J.; Kjaergaard, J.; Kuiper, M.; et al. Targeted Temperature Management at 33 °C versus 36 °C after Cardiac Arrest. N. Engl. J. Med. 2013, 369, 2197–2206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abrams, D.; Schmidt, M.; Pham, T.; Beitler, J.R.; Fan, E.; Goligher, E.; McNamee, J.J.; Patroniti, N.; Wilcox, M.E.; Combes, A.; et al. Mechanical Ventilation for Acute Respiratory Distress Syndrome during Extracorporeal Life Support. Research and Practice. Am. J. Respir. Crit. Care Med. 2020, 201, 514–525. [Google Scholar] [CrossRef] [PubMed]
- Chiu, L.-C.; Kao, K.-C. Mechanical Ventilation during Extracorporeal Membrane Oxygenation in Acute Respiratory Distress Syndrome: A Narrative Review. J. Clin. Med. 2021, 10, 4953. [Google Scholar] [CrossRef]
- Patroniti, N.; Bonatti, G.; Senussi, T.; Robba, C. Mechanical ventilation and respiratory monitoring during extracorporeal membrane oxygenation for respiratory support. Ann. Transl. Med. 2018, 6, 386. [Google Scholar] [CrossRef]
- Ávila-Reyes, D.; Acevedo-Cardona, A.O.; Gómez-González, J.F.; Echeverry-Piedrahita, D.R.; Aguirre-Flórez, M.; Giraldo-Diaconeasa, A. Point-of-care ultrasound in cardiorespiratory arrest (POCUS-CA): Narrative review article. Ultrasound J. 2021, 13, 46. [Google Scholar] [CrossRef]
- Chen, Y.-S.; Yu, H.-Y.; Huang, S.-C.; Lin, J.-W.; Chi, N.-H.; Wang, C.-H.; Wang, S.-S.; Lin, F.-Y.; Ko, W.-J. Extracorporeal membrane oxygenation support can extend the duration of cardiopulmonary resuscitation. Crit. Care Med. 2008, 36, 2529–2535. [Google Scholar] [CrossRef]
- Shin, T.G.; Jo, I.J.; Sim, M.S.; Song, Y.-B.; Yang, J.-H.; Hahn, J.-Y.; Choi, S.H.; Gwon, H.-C.; Jeon, E.-S.; Sung, K.; et al. Two-year survival and neurological outcome of in-hospital cardiac arrest patients rescued by extracorporeal cardiopulmonary resuscitation. Int. J. Cardiol. 2013, 168, 3424–3430. [Google Scholar] [CrossRef]
- Desch, S.; Freund, A.; Akin, I.; Behnes, M.; Preusch, M.R.; Zelniker, T.A.; Skurk, C.; Landmesser, U.; Graf, T.; Eitel, I.; et al. Angiography after Out-of-Hospital Cardiac Arrest without ST-Segment Elevation. N. Engl. J. Med. 2021, 385, 2544–2553. [Google Scholar] [CrossRef]
- Lemkes, J.S.; Janssens, G.N.; van der Hoeven, N.W.; Jewbali, L.S.; Dubois, E.A.; Meuwissen, M.; Rijpstra, T.A.; Bosker, H.A.; Blans, M.J.; Bleeker, G.B.; et al. Coronary Angiography after Cardiac Arrest without ST-Segment Elevation. N. Engl. J. Med. 2019, 380, 1397–1407. [Google Scholar] [CrossRef]
- Stampfl, M.; McCarthy, D.; Koch, J.; Lohmeier, M.; Anderson, E.; Glazer, J. 1366: ECPR prehospital opportunities identified through geospatial mapping. Crit. Care Med. 2022, 50, 684. [Google Scholar] [CrossRef]
- Carlson, J.M.; Etchill, E.; Whitman, G.; Kim, B.S.; Choi, C.W.; Tonna, J.E.; Geocadin, R.; Cho, S.-M. Early withdrawal of life sustaining therapy in extracorporeal cardiopulmonary resuscitation (ECPR): Results from the Extracorporeal Life Support Organization registry. Resuscitation 2022, 179, 71–77. [Google Scholar] [CrossRef]
- Dennis, M.; Lal, S.; Forrest, P.; Nichol, A.; Lamhaut, L.; Totaro, R.J.; Burns, B.; Sandroni, C. In-Depth Extracorporeal Cardiopulmonary Resuscitation in Adult Out-of-Hospital Cardiac Arrest. J. Am. Heart Assoc. 2020, 9, e016521. [Google Scholar] [CrossRef]
- Panchal, A.R.; Bartos, J.A.; Cabañas, J.G.; Donnino, M.W.; Drennan, I.R.; Hirsch, K.G.; Kudenchuk, P.J.; Kurz, M.C.; Lavonas, E.J.; Morley, P.T.; et al. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142 (Suppl. 2), S366–S468. [Google Scholar] [CrossRef]
- Dankiewicz, J.; Cronberg, T.; Lilja, G.; Jakobsen, J.C.; Bělohlávek, J.; Callaway, C.; Cariou, A.; Eastwood, G.; Erlinge, D.; Hovdenes, J.; et al. Targeted hypothermia versus targeted Normothermia after out-of-hospital cardiac arrest (TTM2): A randomized clinical trial—Rationale and design. Am. Heart J. 2019, 217, 23–31. [Google Scholar] [CrossRef]
- Lascarrou, J.-B.; Merdji, H.; Le Gouge, A.; Colin, G.; Grillet, G.; Girardie, P.; Coupez, E.; Dequin, P.-F.; Cariou, A.; Boulain, T.; et al. Targeted Temperature Management for Cardiac Arrest with Nonshockable Rhythm. N. Engl. J. Med. 2019, 381, 2327–2337. [Google Scholar] [CrossRef]
- Wolfrum, S.; Roedl, K.; Hanebutte, A.; Pfeifer, R.; Kurowski, V.; Riessen, R.; Daubmann, A.; Braune, S.; Söffker, G.; Bibiza-Freiwald, E.; et al. Temperature Control After In-Hospital Cardiac Arrest: A Randomized Clinical Trial. Circulation 2022, 146, 1357–1366. [Google Scholar] [CrossRef]
- Perbet, S.; Mongardon, N.; Dumas, F.; Bruel, C.; Lemiale, V.; Mourvillier, B.; Carli, P.; Varenne, O.; Mira, J.-P.; Wolff, M.; et al. Early-Onset Pneumonia after Cardiac Arrest: Characteristics, risk factors and influence on prognosis. Am. J. Respir. Crit. Care Med. 2011, 184, 1048–1054. [Google Scholar] [CrossRef]
- Polderman, K.H. Mechanisms of action, physiological effects, and complications of hypothermia. Crit. Care Med. 2009, 37, S186–S202. [Google Scholar] [CrossRef]
- Geurts, M.; Macleod, M.R.; Kollmar, R.; Kremer, P.H.C.; Van Der Worp, H.B. Therapeutic Hypothermia and the Risk of Infection: A systematic review and meta-analysis. Crit. Care Med. 2014, 42, 231–242. [Google Scholar] [CrossRef] [PubMed]
- François, B.; Cariou, A.; Clere-Jehl, R.; Dequin, P.-F.; Renon-Carron, F.; Daix, T.; Guitton, C.; Deye, N.; Legriel, S.; Plantefève, G.; et al. Prevention of Early Ventilator-Associated Pneumonia after Cardiac Arrest. N. Engl. J. Med. 2019, 381, 1831–1842. [Google Scholar] [CrossRef] [PubMed]
- Jakkula, P.; COMACARE study group; Pettilä, V.; Skrifvars, M.B.; Hästbacka, J.; Loisa, P.; Tiainen, M.; Wilkman, E.; Toppila, J.; Koskue, T.; et al. Targeting low-normal or high-normal mean arterial pressure after cardiac arrest and resuscitation: A randomised pilot trial. Intensiv. Care Med. 2018, 44, 2091–2101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ameloot, K.; De Deyne, C.; Eertmans, W.; Ferdinande, B.; Dupont, M.; Palmers, P.-J.; Petit, T.; Nuyens, P.; Maeremans, J.; Vundelinckx, J.; et al. Early goal-directed haemodynamic optimization of cerebral oxygenation in comatose survivors after cardiac arrest: The Neuroprotect post-cardiac arrest trial. Eur. Heart J. 2019, 40, 1804–1814. [Google Scholar] [CrossRef] [PubMed]
- Conrad, S.; Rycus, P. Extracorporeal membrane oxygenation for refractory cardiac arrest. Ann. Card. Anaesth. 2017, 20, S4–S10. [Google Scholar] [CrossRef] [PubMed]
- Ruggeri, L.; Franco, A.; Alba, A.C.; Lembo, R.; Frassoni, S.; Scandroglio, A.M.; Calabrò, M.G.; Zangrillo, A.; Pappalardo, F. Coagulation Derangements in Patients With Refractory Cardiac Arrest Treated With Extracorporeal Cardiopulmonary Resuscitation. J. Cardiothorac. Vasc. Anesth. 2019, 33, 1877–1882. [Google Scholar] [CrossRef]
- Cartwright, B.; Bruce, H.M.; Kershaw, G.; Cai, N.; Othman, J.; Gattas, D.; Robson, J.L.; Hayes, S.; Alicajic, H.; Hines, A.; et al. Hemostasis, coagulation and thrombin in venoarterial and venovenous extracorporeal membrane oxygenation: The HECTIC study. Sci. Rep. 2021, 11, 7975. [Google Scholar] [CrossRef]
- Bonicolini, E.; Martucci, G.; Simons, J.; Raffa, G.M.; Spina, C.; Coco, V.L.; Arcadipane, A.; Pilato, M.; Lorusso, R. Limb ischemia in peripheral veno-arterial extracorporeal membrane oxygenation: A narrative review of incidence, prevention, monitoring, and treatment. Crit. Care 2019, 23, 266. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, D.; Hirose, H.; Cavarocchi, N.; Entwistle, J.W. The Impact of Vascular Complications on Survival of Patients on Venoarterial Extracorporeal Membrane Oxygenation. Ann. Thorac. Surg. 2016, 101, 1729–1734. [Google Scholar] [CrossRef] [Green Version]
- Yen, C.-C.; Kao, C.-H.; Tsai, C.-S.; Tsai, S.-H. Identifying the Risk Factor and Prevention of Limb Ischemia in Extracorporeal Membrane Oxygenation with Femoral Artery Cannulation. Heart Surg. Forum 2018, 21, E018–E022. [Google Scholar] [CrossRef]
- Lorusso, R.; Shekar, K.; MacLaren, G.; Schmidt, M.; Pellegrino, V.; Meyns, B.; Haft, J.; Vercaemst, L.; Pappalardo, F.; Bermudez, C.; et al. ELSO Interim Guidelines for Venoarterial Extracorporeal Membrane Oxygenation in Adult Cardiac Patients. ASAIO J. 2021, 67, 827–844. [Google Scholar] [CrossRef]
- Callaway, C.W.; Donnino, M.W.; Fink, E.L.; Geocadin, R.G.; Golan, E.; Kern, K.B.; Leary, M.; Meurer, W.J.; Peberdy, M.A.; Thompson, T.M.; et al. Part 8: Post–Cardiac Arrest Care: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2015, 132 (Suppl. 2), S465–S482. [Google Scholar] [CrossRef] [Green Version]
- Elmer, J.; Torres, C.; Aufderheide, T.P.; Austin, M.A.; Callaway, C.W.; Golan, E.; Herren, H.; Jasti, J.; Kudenchuk, P.J.; Scales, D.C.; et al. Association of early withdrawal of life-sustaining therapy for perceived neurological prognosis with mortality after cardiac arrest. Resuscitation 2016, 102, 127–135. [Google Scholar] [CrossRef] [Green Version]
- Tjepkema-Cloostermans, M.C.; Hofmeijer, J.; Beishuizen, A.; Hom, H.W.; Blans, M.J.; Bosch, F.H.; Van Putten, M.J.A.M. Cerebral Recovery Index: Reliable Help for Prediction of Neurologic Outcome After Cardiac Arrest. Crit. Care Med. 2017, 45, e789–e797. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cassara, C.M.; Long, M.T.; Dollerschell, J.T.; Chae, F.; Hall, D.J.; Demiralp, G.; Stampfl, M.J.; Bernardoni, B.; McCarthy, D.P.; Glazer, J.M. Extracorporeal Cardiopulmonary Resuscitation: A Narrative Review and Establishment of a Sustainable Program. Medicina 2022, 58, 1815. https://doi.org/10.3390/medicina58121815
Cassara CM, Long MT, Dollerschell JT, Chae F, Hall DJ, Demiralp G, Stampfl MJ, Bernardoni B, McCarthy DP, Glazer JM. Extracorporeal Cardiopulmonary Resuscitation: A Narrative Review and Establishment of a Sustainable Program. Medicina. 2022; 58(12):1815. https://doi.org/10.3390/medicina58121815
Chicago/Turabian StyleCassara, Chris M., Micah T. Long, John T. Dollerschell, Floria Chae, David J. Hall, Gozde Demiralp, Matthew J. Stampfl, Brittney Bernardoni, Daniel P. McCarthy, and Joshua M. Glazer. 2022. "Extracorporeal Cardiopulmonary Resuscitation: A Narrative Review and Establishment of a Sustainable Program" Medicina 58, no. 12: 1815. https://doi.org/10.3390/medicina58121815