
High Percentage of Complications and Re-Operations Following Dynamic Locking Plate Fixation with the Targon® FN for Intracapsular Proximal Femoral Fractures: An Analysis of Risk Factors

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Implant, Surgical Technique, Rehabilitation and Follow Up
2.3. Data Analysis
2.4. Statistical Analysis
3. Results
3.1. Complications and Re-Operations
3.2. Analysis of Risk Factors for Complications
3.3. Analysis of Risk Factors for Re-Operation
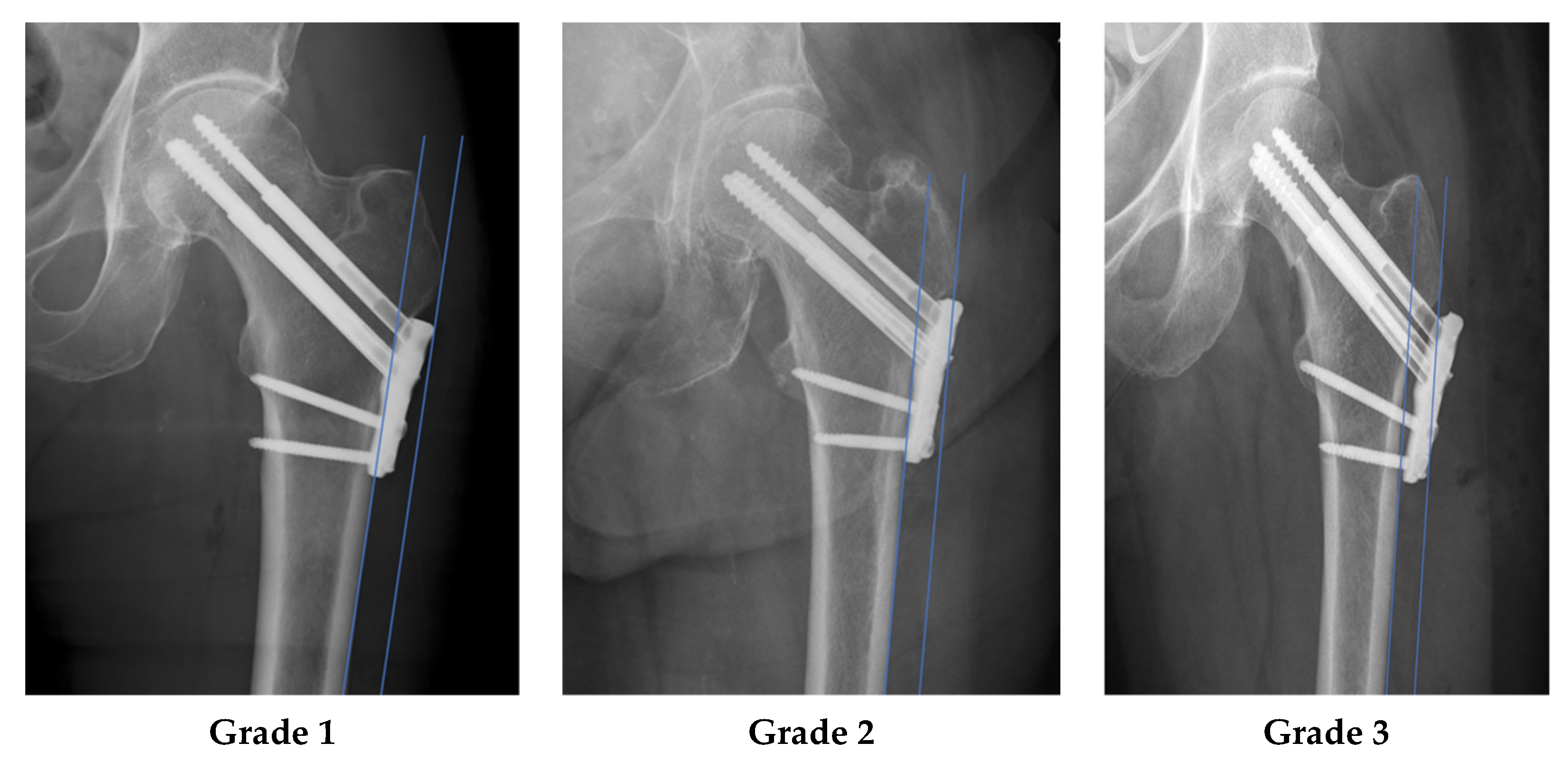
3.4. Plate Position as a Risk Factor for Plate Removal
4. Discussion
4.1. Key Results
4.2. Limitations
4.3. Interpretation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Parker, M.J.; Cawley, S. Cemented or uncemented hemiarthroplasty for displaced intracapsular fractures of the hip: A randomized trial of 400 patients. Bone Jt. J. 2019, 102-B, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Stöckle, U.; Lucke, M.; Haas, N.P. Der Oberschenkelhalsbruch. Dtsch. Arztebl. 2005, 102, 3426–3434. [Google Scholar]
- Knobe, M.; Siebert, C.H. Hüftgelenknahe Frakturen im hohen Lebensalter. Orthopäde 2014, 43, 314–324. [Google Scholar] [CrossRef] [PubMed]
- Blomfeldt, R.; Törnkvist, H.; Ponzer, S.; Söderqvist, A.; Tidermark, J. Comparison of Internal Fixation with Total Hip Replacement for Displaced Femoral Neck Fractures: Randomized, Controlled Trial Performed at Four Years. JBJS 2005, 87, 1680–1688. [Google Scholar] [CrossRef]
- Nilsson, L.T.; Johansson, Å.; Strömqvist, B. Factors predicting healing complications in femoral neck fractures: 138 patients followed for 2 years. Acta Orthop. Scand. 1993, 64, 175–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alho, A.; Benterud, J.G.; Rønningen, H.; Høiseth, A. Prediction of disturbed healing in femoral neck fracture. Acta Orthop. Scand. 1992, 63, 639–644. [Google Scholar] [CrossRef]
- Dolatowski, F.C.; Frihagen, F.; Bartels, S.; Opland, V.; Benth, J.Š.; Talsnes, O.; Hoelsbrekken, S.E.; Utvåg, S.E. Screw Fixation Versus Hemiarthroplasty for Nondisplaced Femoral Neck Fractures in Elderly Patients: A Multicenter Randomized Controlled Trial. J. Bone Joint Surg. Am. 2019, 101, 136–144. [Google Scholar] [CrossRef]
- Maffulli, N.; Aicale, R. Proximal Femoral Fractures in the Elderly: A Few Things to Know, and Some to Forget. Medicina Mex 2022, 58, 1314. [Google Scholar] [CrossRef]
- Ly, T.; Swiontkowski, M. Treatment of femoral neck fractures in young adults. J. Bone Jt. Surg. Am. 2008, 90, 2254–2266. [Google Scholar] [CrossRef]
- Parker, M.J.; Raghavan, R.; Gurusamy, K. Incidence of fracture-healing complications after femoral neck fractures. Clin. Orthop. 2007, 458, 175–179. [Google Scholar] [CrossRef]
- Lu-Yao, G.L.; Keller, R.B.; Littenberg, B.; Wennberg, J.E. Outcomes after displaced fractures of the femoral neck. A meta-analysis of one hundred and six published reports. J. Bone Jt. Surg.—Ser. A 1994, 76, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Knobe, M.; Altgassen, S.; Maier, K.-J.; Gradl-Dietsch, G.; Kaczmarek, C.; Nebelung, S.; Klos, K.; Kim, B.; Gueorguiev, B.; Horst, K.; et al. Screw-blade fixation systems in Pauwels three femoral neck fractures: A biomechanical evaluation. Int. Orthop. 2018, 42, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Hsueh, K.-K.; Fang, C.-K.; Chen, C.-M.; Su, Y.-P.; Wu, H.-F.; Chiu, F.-Y. Risk factors in cutout of sliding hip screw in intertrochanteric fractures: An evaluation of 937 patients. Int. Orthop. 2010, 34, 1273–1276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, H.K.; Choi, H.J.; Yang, K.H. Risk factors of avascular necrosis of the femoral head and fixation failure in patients with valgus angulated femoral neck fractures over the age of 50 years. Injury 2016, 47, 2743–2748. [Google Scholar] [CrossRef] [PubMed]
- Van Embden, D.; Roukema, G.R.; Rhemrev, S.J.; Genelin, F.; Meylaerts, S.A.G. The Pauwels classification for intracapsular hip fractures: Is it reliable? Injury 2011, 42, 1238–1240. [Google Scholar] [CrossRef] [PubMed]
- Caviglia, H.A.; Quintana Osorio, P.; Comando, D. Classification and diagnosis of intracapsular fractures of the proximal femur. Clin. Orthop. 2002, 399, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Hoshino, C.M.; O’Toole, R.V. Fixed angle devices versus multiple cancellous screws: What does the evidence tell us? Injury 2015, 46, 474–477. [Google Scholar] [CrossRef]
- Linde, F.; Andersen, E.; Hvass, I.; Madsen, F.; Pallesen, R. Avascular femoral head necrosis following fracture fixation. Injury 1986, 17, 159–163. [Google Scholar] [CrossRef]
- Nauth, A.; Creek, A.T.; Zellar, A.; Lawendy, A.R.; Dowrick, A.; Gupta, A.; Dadi, A.; van Kampen, A.; Yee, A.; de Vries, A.C.; et al. Fracture fixation in the operative management of hip fractures (FAITH): An international, multicentre, randomised controlled trial. Lancet 2017, 389, 1519–1527. [Google Scholar] [CrossRef] [Green Version]
- Thein, R.; Herman, A.; Kedem, P.; Chechik, A.; Shazar, N. Osteosynthesis of unstable intracapsular femoral neck fracture by dynamic locking plate or screw fixation: Early results. J. Orthop. Trauma 2014, 28, 70–76. [Google Scholar] [CrossRef]
- Parker, M.; Cawley, S.; Palial, V. Internal fixation of intracapsular fractures of the hip using a dynamic locking plate: Two-year follow-up of 320 patients. Bone Jt. J. 2013, 95, 1402–1405. [Google Scholar] [CrossRef] [PubMed]
- Körver, R.J.P.; Wieland, A.W.J.; Kaarsemaker, S.; Nieuwenhuis, J.J.; Janzing, H.M.J. Clinical experience, primary results and pitfalls in the treatment of intracapsular hip fractures with the Targon® FN locking plate. Injury 2013, 44, 1926–1929. [Google Scholar] [CrossRef] [PubMed]
- Takigawa, N.; Yasui, K.; Eshiro, H.; Moriuchi, H.; Abe, M.; Tsujinaka, S.; Kinoshita, M. Clinical results of surgical treatment for femoral neck fractures with the Targon® FN. Injury 2016, 47, S44–S48. [Google Scholar] [CrossRef] [PubMed]
- Osarumwense, D.; Tissingh, E.; Wartenberg, K.; Aggarwal, S.; Ismail, F.; Orakwe, S.; Khan, F. The targon FN system for the management of intracapsular neck of femur fractures: Minimum 2-year experience and outcome in an independent hospital. CiOS Clin. Orthop. Surg. 2015, 7, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Alshameeri, Z.; Elbashir, M.; Parker, M.J. The outcome of intracapsular hip fracture fixation using the Targon Femoral Neck (TFN) locking plate system or cannulated cancellous screws: A comparative study involving 2004 patients. Injury 2017, 48, 2555–2562. [Google Scholar] [CrossRef] [PubMed]
- Hou, X.; Shi, G.; Zhang, Y.; Xing, B.; Xu, D. Comparison between Three Cannulated Screws and Targon Locking Plate for Displaced Intracapsular Hip Fracture: A Retrospective Stud. Res. Sq. 2022, preprint. [Google Scholar] [CrossRef]
- Parker, M.J.; Pryor, G.; Gurusamy, K. Hemiarthroplasty versus internal fixation for displaced intracapsular hip fractures: A long-term follow-up of a randomised trial. Injury 2010, 41, 370–373. [Google Scholar] [CrossRef]
- Griffin, X.L.; Parsons, N.; Achten, J.; Costa, M.L. The Targon Femoral Neck hip screw versus cannulated screws for internal fixation of intracapsular fractures of the hip. Bone. Jt. J. 2014, 96-B, 652–657. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Parker, M.J.; Stedtfeld, H.-W. Internal fixation of intracapsular hip fractures with a dynamic locking plate: Initial experience and results for 83 patients treated with a new implant. Injury 2010, 41, 348–351. [Google Scholar] [CrossRef]
- Garden, R.S. Low-Angle Fixation in Fractures of the Femoral Neck. Bone Jt. J. 1961, 43-B, 647–663. [Google Scholar] [CrossRef]
- Müller, M.E.; Koch, P.; Nazarian, S.; Schatzker, J. The Comprehensive Classification of Fractures of Long Bones; Springer: Berlin/Heidelberg, Germany, 1990. [Google Scholar] [CrossRef]
- Wilson, J.D.; Eardley, W.; Odak, S.; Jennings, A. To what degree is digital imaging reliable? Validation of femoral neck shaft angle measurement in the era of picture archiving and communication systems. Br. J. Radiol. 2011, 84, 375–379. [Google Scholar] [CrossRef] [Green Version]
- Nash, W.; Harris, A. The Dorr type and cortical thickness index of the proximal femur for predicting peri-operative complications during hemiarthroplasty. J. Orthop. Surg. 2014, 22, 92–95. [Google Scholar] [CrossRef] [PubMed]
- Baumgaertner, M.R.; Curtin, S.L.; Lindskog, D.M.; Keggi, J.M. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J. Bone Jt. Surg. 1995, 77, 1058–1064. [Google Scholar] [CrossRef] [PubMed]
- Link, B.-C.; van Veelen, N.M.; Boernert, K.; Kittithamvongs, P.; Beeres, F.J.P.; de Boer, H.H.; Migliorini, F.; Nebelung, S.; Knobe, M.; Ruchholtz, S.; et al. The radiographic relationship between the cortical overlap view (COV) and the tip of the greater trochanter. Sci. Rep. 2021, 11, 18404. [Google Scholar] [CrossRef]
- Horan, T.C.; Gaynes, R.P.; Martone, W.J.; Jarvis, W.R.; Emori, T.G. CDC Definitions of Nosocomial Surgical Site Infections, 1992, A Modification of CDC Definitions of Surgical Wound Infections. Infect. Control Hosp. Epidemiol. 1992, 13, 606–608. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, M.E.; Hayken, G.D.; Steinberg, D.R. A quantitative system for staging avascular necrosis. J. Bone Jt. Surg. Br. 1995, 77, 34–41. [Google Scholar] [CrossRef]
- Parker Martyn, J.; Gurusamy Kurinchi, S. Internal fixation implants for intracapsular hip fractures in adults. Cochrane Database Syst. Rev. 2011, 4, 1465–1858. [Google Scholar] [CrossRef]
- Loizou, C.L.; Parker, M.J. Avascular necrosis after internal fixation of intracapsular hip fractures; a study of the outcome for 1023 patients. Injury 2009, 40, 1143–1146. [Google Scholar] [CrossRef]
- Damany, D.S.; Parker, M.J.; Chojnowski, A. Complications after intracapsular hip fractures in young adults: A meta-analysis of 18 published studies involving 564 fractures. Injury 2005, 36, 131–141. [Google Scholar] [CrossRef]
- Saß, M.; Mittlmeier, T. Joint-preserving treatment of medial femoral neck fractures with an angular stable implant. Oper. Orthop. Traumatol. 2016, 28, 291–308. [Google Scholar] [CrossRef] [PubMed]
- Parker, M.J. Hemiarthroplasty versus internal fixation for displaced intracapsular fractures of the hip in elderly men. Bone Jt. J. 2015, 97-B, 992–996. [Google Scholar] [CrossRef] [PubMed]
- Kolaczko, J.G.; McMellen, C.J.; Magister, S.J.; Wetzel, R.J. Comparison of time to healing and major complications after surgical fixation of nondisplaced femoral neck stress fractures: A systematic review. Injury 2021, 52, 647–652. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient Dependent Factors | Hospital Dependent Factors | ||
|---|---|---|---|
| Sex, No. (%) | Time to surgery hours (SD) | ||
| Male | 35 (48.6) | Mean | 19.99 (20.65) |
| Female | 37 (51.4) | postoperative CCD angle No. | |
| Age, y | <125 | 5 (6.94) | |
| Mean (SD) | 61.36 (16.35) | 125–135 | 29 (40.28) |
| Median (range) | 60.50 (25–89) | >135 | 38 (52.78) |
| Age group, No. (%) | measured TAD (SD) | ||
| <65 y | 42 (58.33) | Mean | 18.79 (5.05) |
| ≥65 y | 30 (41.66) | Reduction No. (%) | |
| ASA, No. (%) | Open | 23 (31.94) | |
| I | 10 (13.9) | Closed | 29 (40.28) |
| II | 38 (52.8) | Not necessary | 20 (27.78) |
| III | 23 (31.9) | Time to full weight bearing weeks No. (%) | |
| IV | 1 (1.4) | Immediately | 27 (37.50) |
| V | 0 (0) | 6 weeks postoperative | 26 (36.11) |
| Diabetes, No. (%) | 10–12 weeks postoperative | 19 (26.39) | |
| Type-I | 1 (1.4) | Out of office operation No. (%) | |
| Type-II | 3 (4.2) | Yes | 33 (45.83) |
| No | 68 (94.4) | No | 39 (54.17) |
| Dementia No. (%) | |||
| Yes | 5 (6.9) | ||
| No | 67 (93.1) | ||
| Osteoporosis No. (%) | |||
| Yes | 10 (86.1) | ||
| No | 62 (13.9) | ||
| Smoking status, No. (%) | |||
| Yes | 17 (23.6) | ||
| No | 55 (76.4) | ||
| AO fracture classification No. (%) | |||
| 31-B1 | 30 (41.7) | ||
| 31-B2 | 35 (48.6) | ||
| 31-B3 | 7 (9.7) | ||
| Garden fracture classification (%) | |||
| Non-displaced | 41 (56.9) | ||
| Displaced | 31 (43.1) | ||
| Trauma intensity * No. (%) | |||
| Low | 51 (70.8) | ||
| High | 21 (29.2) | ||
| Complications | Cat. A | Cat. B | All | % * | Reoperations ** |
|---|---|---|---|---|---|
| Hematoma and bleeding | |||||
| hematoma | - | 1 | 1 | 1.4 | 3 |
| Soft tissue | |||||
| tractus irritation | 17 | - | 17 | 23.6 | 17 |
| Reduction | |||||
| Secondary loss of reduction | - | 2 | 2 | 2.8 | 2 |
| Plate and screws | |||||
| screw perforation through the cortex of the femoral head | - | 5 | 5 | 6.9 | 5 |
| Loosening Tele Screw | - | 2 | 2 | 2.8 | 5 |
| Loosening Screw base plate | - | 1 | 1 | 1.4 | 1 |
| Osseus disorders | |||||
| avascular necrosis of the femoral head | - | 4 | 4 | 5.6 | 5 |
| nonunion | - | 4 | 4 | 5.6 | 4 |
| postoperative femoroactetabular impingement | - | 2 | 2 | 2.8 | 4 |
| Total number | 17 | 21 | 38 | 52.8 | 46 |
| Complete Implant Removal | Partial Implant Removal | Total Hip Arthroplasty | Hip Arthroscopy | Revision 90° Blade Plate | Girdlestone Procedure | Revision Total Hip Replacement | Wound Revision | Revision of ITB | |
|---|---|---|---|---|---|---|---|---|---|
| Complete implant removal | 20 | ||||||||
| Partial implant removal | 4 | ||||||||
| Total hip arthroplasty | 6 | 2 | |||||||
| Monopolar hip arthroplasty | 1 | ||||||||
| Hip arthroscopy | 1 | 1 | |||||||
| Cement spacer interposition | 1 | ||||||||
| Removal of cement spacer | 1 | ||||||||
| Valgus osteotomy with 90° blade plate | 1 | ||||||||
| Revision 90° blade plate | 1 | ||||||||
| Girdlestone procedure | 1 | ||||||||
| Exchange of one TeleScrew | 1 | ||||||||
| Revision total hip replacement | 1 | ||||||||
| Wound revision | 3 | ||||||||
| Revision of ITB | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuner, E.; Gütler, J.; Delagrammaticas, D.E.; van de Wall, B.J.M.; Knobe, M.; Beeres, F.J.P.; Babst, R.; Link, B.-C. High Percentage of Complications and Re-Operations Following Dynamic Locking Plate Fixation with the Targon® FN for Intracapsular Proximal Femoral Fractures: An Analysis of Risk Factors. Medicina 2022, 58, 1812. https://doi.org/10.3390/medicina58121812
Kuner E, Gütler J, Delagrammaticas DE, van de Wall BJM, Knobe M, Beeres FJP, Babst R, Link B-C. High Percentage of Complications and Re-Operations Following Dynamic Locking Plate Fixation with the Targon® FN for Intracapsular Proximal Femoral Fractures: An Analysis of Risk Factors. Medicina. 2022; 58(12):1812. https://doi.org/10.3390/medicina58121812
Chicago/Turabian StyleKuner, Emanuel, Jens Gütler, Dimitri E. Delagrammaticas, Bryan J. M. van de Wall, Matthias Knobe, Frank J. P. Beeres, Reto Babst, and Björn-Christian Link. 2022. "High Percentage of Complications and Re-Operations Following Dynamic Locking Plate Fixation with the Targon® FN for Intracapsular Proximal Femoral Fractures: An Analysis of Risk Factors" Medicina 58, no. 12: 1812. https://doi.org/10.3390/medicina58121812