
Silodosin versus Tamsulosin for Medical Expulsive Therapy of Ureteral Stones: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials
 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Search Strategy
2.3. Study Selection and Data Extraction
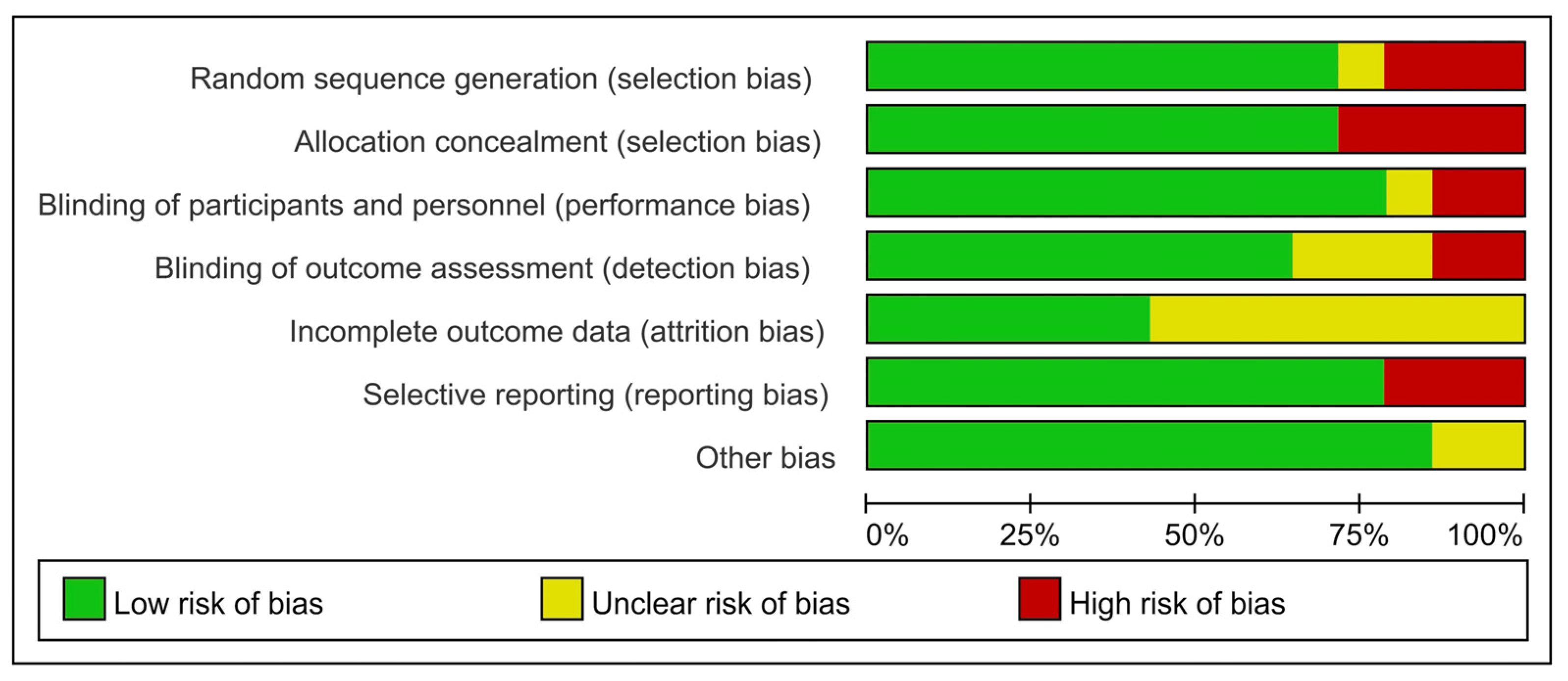
2.4. Study Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Eligible Studies
3.2. Characteristic of Included Studies
3.3. Quality Assessment
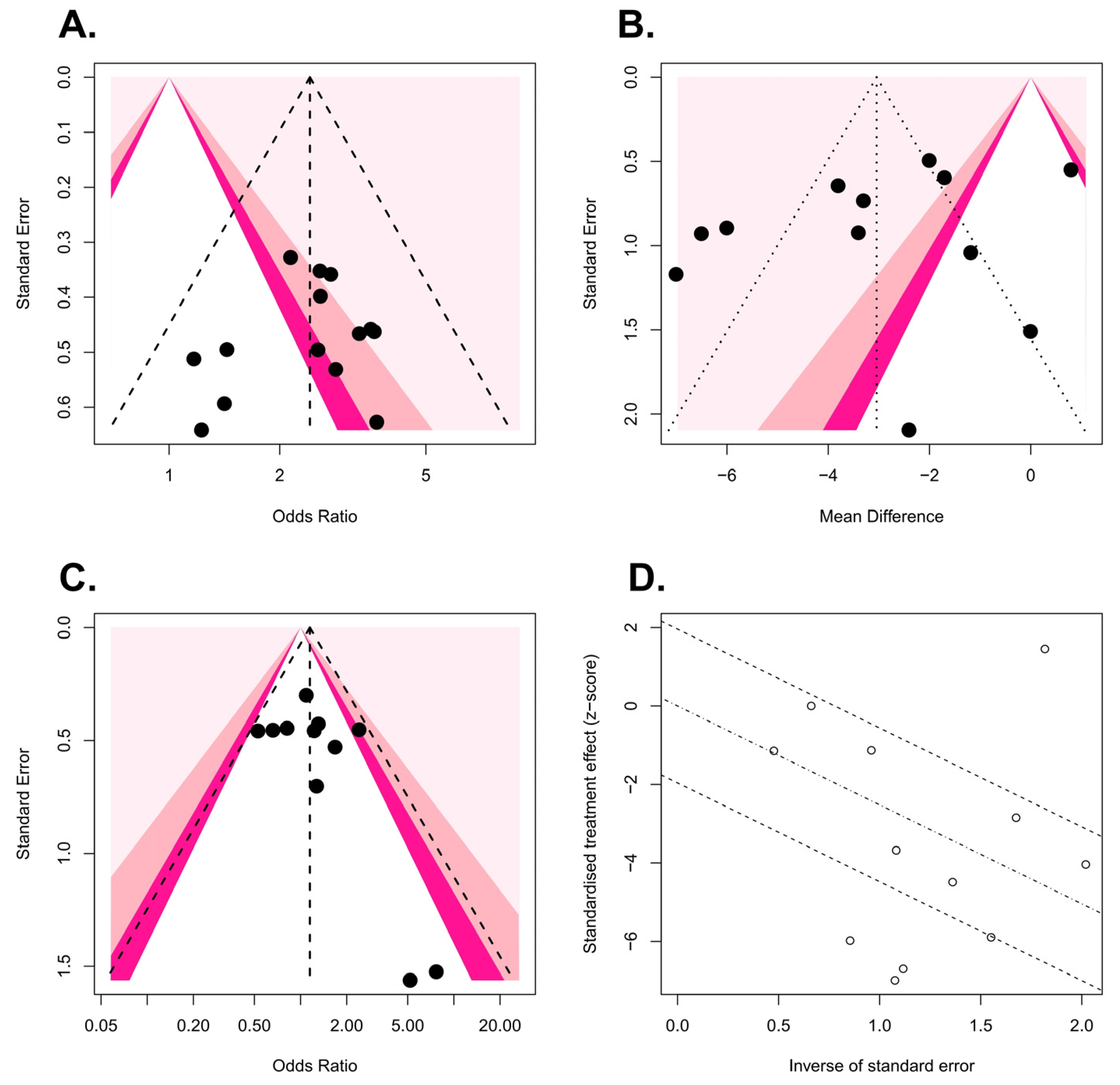
3.4. Publication Bias and Heterogeneity Assessment
3.5. Stone Expulsion Rate
3.6. Stone Expulsion Time
3.7. Total Complication Rate
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jung, H.D.; Seo, I.Y.; Lee, J.Y. Large database study of urinary stone composition in south korea: Korean society of endourology and robotics (kser) research series. Investig. Clin. Urol. 2021, 62, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.Y.; Jung, H.D.; Kwon, S.H.; Lee, E.K.; Lee, J.Y.; Lee, S.H. Does early retrograde intrarenal surgery improve the cost-effectiveness of renal stone management? Yonsei Med. J. 2020, 61, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Tefik, T.; Guven, S.; Villa, L.; Gokce, M.I.; Kallidonis, P.; Petkova, K.; Kiremit, M.C.; Sonmez, M.G.; de Lorenzis, E.; Eryildirim, B.; et al. Urolithiasis practice patterns following the COVID-19 pandemic: Overview from the eulis collaborative research working group. Eur. Urol. 2020, 78, e21–e24. [Google Scholar] [CrossRef] [PubMed]
- Türk, C.; Skolarikos, A.; Neisius, A.; Petrik, A.; Seitz, C.; Thomas, K. EAU guidelines on urolithiasis, EAU guidelines. In Proceedings of the EAU Annual Congress Amsterdam 2020, Amsterdam, The Netherlands, 20–24 March 2020. [Google Scholar]
- Assimos, D.; Krambeck, A.; Miller, N.L.; Monga, M.; Murad, M.H.; Nelson, C.P.; Pace, K.T.; Pais, V.M., Jr.; Pearle, M.S.; Preminger, G.M.; et al. Surgical management of stones: American urological association/endourological society guideline, part ii. J. Urol. 2016, 196, 1161–1169. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Priyanka, P.; Jadhav, R.R. Comparison between tamsulosin and silodosin in lower ureteric stone—A randomised controlled study. J. Evol. Med. Dent. Sci. 2017, 6, 6766–6769. [Google Scholar] [CrossRef]
- Reddy, S.; Prathvi, P.; Kulshreshtha, M.; Singh, P. A prospective study comparing tamsulosin and silodosin in medical expulsive therapy for lower ureteric stones. J. Evol. Med. Dent. Sci. 2016, 5, 4108–4111. [Google Scholar] [CrossRef]
- Sharma, G.; Khadav, B.; Sandhasukhi, T.C.; Gupta, M.; Gupta, H.L. Comparative analysis of silodosin and tamsulosin in distal ureteric calculus treatment. J. Evid. Based Med. Healthc 2016, 3, 4647–4649. [Google Scholar] [CrossRef] [PubMed]
- Antony, D. Comparative efficacy of silodosin vs tamsulosin for ureteric calculus: A single centre double blind randomised controlled trial. J. Med. Sci. Clin. Res. 2017, 5, 31928–31932. [Google Scholar] [CrossRef]
- AS, A.; Pillai, S.R.; Mary, A.; Aravindakshan, R. Efficacy of tamsulosin and silodosin as medical expulsive therapy in the management of distal ureteral stones: A randomized controlled study. Int. Surg. J. 2016, 3, 4. [Google Scholar] [CrossRef]
- Dell’Atti, L. Silodosin versus tamsulosin as medical expulsive therapy for distal ureteral stones: A prospective randomized study. Urologia 2015, 82, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Elgalaly, H.; Sakr, A.; Fawzi, A.; Salem, E.A.; Desoky, E.; Shahin, A.; Kamel, M. Silodosin vs tamsulosin in the management of distal ureteric stones: A prospective randomised study. Arab J. Urol. 2016, 14, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Georgescu, D.; Ionita Radu, F.; Multescu, R.; Dragutescu, M.; Geavlete, B.; Geavlete, P.; Negrei, C.; Mischianu, D.; Georgescu, M.; Ginghina, O. The role of alpha 1-blockers in the medical expulsive therapy for ureteral calculi—A prospective controlled randomized study comparing tamsulosin and silodosint. Farmacia 2015, 63, 184–188. [Google Scholar]
- Gharib, T.; Mohey, A.; Fathi, A.; Alhefnawy, M.; Alazaby, H.; Eldakhakhny, A. Comparative study between silodosin and tamsulosin in expectant therapy of distal ureteral stones. Urol. Int. 2018, 101, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Lodh, B.; Singh, A.K.; Somarendra, K.; Meitei, K.S.; Singh, S.R. Comparing the efficacy of tamsulosin and silodosin in the medical expulsion therapy for ureteral calculi. J. Clin. Diagn. Res. 2013, 7, 1672–1674. [Google Scholar] [CrossRef]
- Gur, M.; Ulu, M.B.; Caliskan, S.T.; Ozturk, K.; Akdeniz, E. Dexketoprofen vs. Tamsulosin vs. Silodosin vs. Tadalafil as medical expulsive therapy for distal ureteral stones in men. J. Coll. Physicians Surg. Pak. 2021, 31, 947–952. [Google Scholar]
- Kumar, S.; Jayant, K.; Agrawal, M.M.; Singh, S.K.; Agrawal, S.; Parmar, K.M. Role of tamsulosin, tadalafil, and silodosin as the medical expulsive therapy in lower ureteric stone: A randomized trial (a pilot study). Urology 2015, 85, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.J.; Faridi, M.S.; Mibang, N.; Singh, R.S. Comparing tamsulosin, silodosin versus silodosin plus tadalafil as medical expulsive therapy for lower ureteric stones: A randomised trial. Arab J. Urol. 2018, 16, 245–249. [Google Scholar] [CrossRef]
- Soliman, M.G.; El-Gamal, O.; El-Gamal, S.; Abdel Raheem, A.; Abou-Ramadan, A.; El-Abd, A. Silodosin versus tamsulosin as medical expulsive therapy for children with lower-third ureteric stones: Prospective randomized placebo-controlled study. Urol. Int. 2021, 105, 568–573. [Google Scholar] [CrossRef]
- Zoumpourlis, V.; Goulielmaki, M.; Rizos, E.; Baliou, S.; Spandidos, D.A. [comment] the COVID-19 pandemic as a scientific and social challenge in the 21st century. Mol. Med. Rep. 2020, 22, 3035–3048. [Google Scholar] [CrossRef] [PubMed]
- Shin, W.Y.; Kim, C.; Lee, S.Y.; Lee, W.; Kim, J.H. Role of primary care and challenges for public-private cooperation during the coronavirus disease 2019 pandemic: An expert delphi study in south korea. Yonsei Med. J. 2021, 62, 660–669. [Google Scholar] [CrossRef]
- Kim, J.; Gewertz, B. Teleurology and digital health app in COVID-19 pandemic. Investig. Clin. Urol. 2020, 61, 333–334. [Google Scholar] [CrossRef]
- Impact of the COVID-19 Pandemic on the Hospital and Outpatient Clinician Workforce: Challenges and Policy Responses (issue brief no. Hp-2022-13); Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services: Washington, DC, USA, 2022.
- Ribal, M.J.; Cornford, P.; Briganti, A.; Knoll, T.; Gravas, S.; Babjuk, M.; Harding, C.; Breda, A.; Bex, A.; Rassweiler, J.J.; et al. European association of urology guidelines office rapid reaction group: An organisation-wide collaborative effort to adapt the european association of urology guidelines recommendations to the coronavirus disease 2019 era. Eur. Urol. 2020, 78, 21–28. [Google Scholar] [CrossRef]
- Campschroer, T.; Zhu, X.; Vernooij, R.W.M.; Lock, T. A-blockers as medical expulsive therapy for ureteric stones: A cochrane systematic review. BJU Int. 2018, 122, 932–945. [Google Scholar] [CrossRef] [PubMed]
- Seitz, C.; Liatsikos, E.; Porpiglia, F.; Tiselius, H.G.; Zwergel, U. Medical therapy to facilitate the passage of stones: What is the evidence? Eur. Urol. 2009, 56, 455–471. [Google Scholar] [CrossRef]
- Wang, H.; Man, L.B.; Huang, G.L.; Li, G.Z.; Wang, J.W. Comparative efficacy of tamsulosin versus nifedipine for distal ureteral calculi: A meta-analysis. Drug. Des. Devel. 2016, 10, 1257–1265. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Yang, Y.; Wang, X.; Tang, Y.; Han, P.; Wang, J. Tadalafil facilitates the distal ureteral stone expulsion: A meta-analysis. J. Endourol. 2017, 31, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Borghi, L.; Meschi, T.; Amato, F.; Novarini, A.; Giannini, A.; Quarantelli, C.; Mineo, F. Nifedipine and methylprednisolone in facilitating ureteral stone passage: A randomized, double-blind, placebo-controlled study. J. Urol. 1994, 152, 1095–1098. [Google Scholar] [CrossRef]
- Parsons, J.K.; Hergan, L.A.; Sakamoto, K.; Lakin, C. Efficacy of alpha-blockers for the treatment of ureteral stones. J. Urol. 2007, 177, 983–987, discussion 987. [Google Scholar] [CrossRef]
- Yilmaz, E.; Batislam, E.; Basar, M.M.; Tuglu, D.; Ferhat, M.; Basar, H. The comparison and efficacy of 3 different alpha1-adrenergic blockers for distal ureteral stones. J. Urol. 2005, 173, 2010–2012. [Google Scholar] [CrossRef] [PubMed]
- Griwan, M.S.; Singh, S.K.; Paul, H.; Pawar, D.S.; Verma, M. The efficacy of tamsulosin in lower ureteral calculi. Urol. Ann. 2010, 2, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Itoh, Y.; Kojima, Y.; Yasui, T.; Tozawa, K.; Sasaki, S.; Kohri, K. Examination of alpha 1 adrenoceptor subtypes in the human ureter. Int. J. Urol. 2007, 14, 749–753. [Google Scholar] [CrossRef]
- Tomiyama, Y.; Kobayashi, K.; Tadachi, M.; Kobayashi, S.; Inada, Y.; Kobayashi, M.; Yamazaki, Y. Expressions and mechanical functions of alpha1-adrenoceptor subtypes in hamster ureter. Eur. J. Pharm. 2007, 573, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, S.; Tomiyama, Y.; Kobayashi, S.; Kojima, Y.; Kubota, Y.; Kohri, K. Characterization of α1-adrenoceptor subtypes mediating contraction in human isolated ureters. Urology 2011, 77, 762.e13–762.e17. [Google Scholar] [CrossRef] [PubMed]
- Itoh, Y.; Okada, A.; Yasui, T.; Hamamoto, S.; Hirose, M.; Kojima, Y.; Tozawa, K.; Sasaki, S.; Kohri, K. Efficacy of selective α1a adrenoceptor antagonist silodosin in the medical expulsive therapy for ureteral stones. Int. J. Urol. 2011, 18, 672–674. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.P.; Hsu, C.W.; Bai, C.H.; Cheng, S.W.; Chen, K.C.; Chen, C. Silodosin versus tamsulosin for medical expulsive treatment of ureteral stones: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0203035. [Google Scholar] [CrossRef]
- Liu, X.J.; Wen, J.G.; Wan, Y.D.; Hu, B.W.; Wang, Q.W.; Wang, Y. Role of silodosin as medical expulsive therapy in ureteral calculi: A meta-analysis of randomized controlled trials. Urolithiasis 2018, 46, 211–218. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Design | Medication | No. of Patients | Age: Mean (SD), Years | Stone Size: Mean (SD), mm | Inclusion Criteria | Quality Assessment |
|---|---|---|---|---|---|---|---|
| Soliman et al. 2021 [21] | RCT | Silodosin 4 mg | 56 | 11.1 (1.8) | 6.2 (1.2) | Distal ureteral stone <1 cm | 1+ |
| Tamsulosin 0.4 mg | 55 | 11.4 (2.4) | 6.3 (0.9) | ||||
| Placebo | 56 | 11.2 (2.6) | 6.5 (1) | ||||
| Gur et al. 2021 [18] | RCT | Dexketoprofen 50 mg | 50 | 38 (31.5–48) | 5.75 (4.77–8.12) | Distal ureteral stone 4–9.9 mm | 1− |
| Tamsulosin 0.4 mg | 48 | 41 (30.25–51.75) | 6.2 (4.62–7.67) | ||||
| Silodosin 8 mg | 49 | 41 (33–0.5) | 6.2 (5.1–7.55) | ||||
| Tadalafil 5 mg | 46 | 39 (31.75–48) | 6.1 (5.17–7.37) | ||||
| Rahman et al. 2018 [20] | RCT | Tamsulosin 0.4 mg | 40 | 38 (10) | 7.5 (1.2) | Distal ureteral stone 5–10 mm | 1+ |
| Silodosin 8 mg | 40 | 34 (12) | 7.4 (1.3) | ||||
| Silodosin 8 mg and tadalafil 5 mg | 40 | 35 (10) | 7.6 (1.35) | ||||
| Gharib et al. 2018 [16] | RCT | Silodosin 8 mg | 75 | 34.5 (9.8) | 7.47 (1.41) | Lower third of the ureter 5–10 mm | 1− |
| Tamsulosin 0.4 mg | 75 | 34.8 (9.7) | 7.54 (4.3) | ||||
| Antony et al. 2017 [11] | RCT | Silodosin 8 mg | 79 | NA | NA | Ureteral stone <10 mm | 1+ |
| Tamsulosin 0.4 mg | 78 | NA | NA | ||||
| Priyanka et al. 2017 [8]. | RCT | Tamsulosin 0.4 mg | 27 | 34.8 (12.7) | NA | Distal ureteral stones <10 mm | 1− |
| Silodosin 8 mg | 28 | 36.4 (12.7) | NA | ||||
| Reddy et al. 2016 [9] | RCT | Tamsulosin 0.4 mg | 50 | 39.4 (21–70) | NA | Lower ureteral stone <10 mm | 1− |
| Silodosin 8 mg | 50 | 38.2 (21–70) | NA | ||||
| Sharma et al. 2016 [10] | RCT | Silodosin 8 mg | 52 | NA | NA | Distal ureteral stone <10 mm | 1− |
| Tamsulosin 0.4 mg | 54 | NA | NA | ||||
| Elgalaly et al. 2016 [14] | RCT | Silodosin 8 mg | 52 | 33.6 (9.9) | 5.4 (1.5) | Distal ureteral stones <10 mm | 1− |
| Tamsulosin 0.4 mg | 51 | 35.5 (11.3) | 5.6 (1.2) | ||||
| AS et al. 2016 [12] | RCT | Tamsulosin 0.4 mg | 40 | 35 (8.5) | 7 (2) | Distal ureteral stones <10 mm | 1− |
| Silodosin 8 mg | 40 | 32 (7.5) | 7 (1.5) | ||||
| Control (diclofenac 50 mg to 100 mg prn) | 40 | 34 (8.5) | 6.8 (1.8) | ||||
| Dell’Atti et al. 2015 [13] | RCT | Tamsulosin 0.4 mg | 67 | 35 (21–64) | 5.37 (1.33) | Lower ureteral stone 4–10 mm | 1− |
| Silodosin 8 mg | 66 | 36 (19–72) | 5.82 (1.66) | ||||
| Georgescu et al. 2015 [15] | RCT | Tamsulosin 0.4 mg and diclofenac 50 mg | 50 | 43.5 (13.31) | 5.08 (2.09) | Ureteral stone <10 mm | 1− |
| Silodosin 8 mg and diclofenac 50 mg | 50 | 44.26 (13) | 5.32 (2.09) | ||||
| Anti-inflammatory drugs | 50 | 45.14 (11.58) | 5.1 (2.02) | ||||
| Kumar et al. 2015 [19] | RCT | Tamsulosin 0.4 mg | 90 | 36.4 (10.03) | 7.44 (1.2) | Distal ureteral stones 5–10 mm | 1+ |
| Silodosin 8 mg | 90 | 36.73 (12) | 7.5 (1.3) | ||||
| Tadalafil 10 mg | 90 | 37.5 (13.5) | 7.77 (1.35) | ||||
| Gupta et al. 2013 [17] | RCT | Tamsulosin 0.4 mg | 50 | NA | 7 (2.3) | Middle or lower ureteral stones <1 cm | 1+ |
| Silodosin 8 mg | 50 | NA | 6.6 (1.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, H.D.; Cho, K.S.; Jun, D.Y.; Jeong, J.Y.; Moon, Y.J.; Chung, D.Y.; Kang, D.H.; Cho, S.; Lee, J.Y. Silodosin versus Tamsulosin for Medical Expulsive Therapy of Ureteral Stones: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials. Medicina 2022, 58, 1794. https://doi.org/10.3390/medicina58121794
Jung HD, Cho KS, Jun DY, Jeong JY, Moon YJ, Chung DY, Kang DH, Cho S, Lee JY. Silodosin versus Tamsulosin for Medical Expulsive Therapy of Ureteral Stones: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials. Medicina. 2022; 58(12):1794. https://doi.org/10.3390/medicina58121794
Chicago/Turabian StyleJung, Hae Do, Kang Su Cho, Dae Young Jun, Jae Yong Jeong, Young Joon Moon, Doo Yong Chung, Dong Hyuk Kang, Seok Cho, and Joo Yong Lee. 2022. "Silodosin versus Tamsulosin for Medical Expulsive Therapy of Ureteral Stones: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials" Medicina 58, no. 12: 1794. https://doi.org/10.3390/medicina58121794