

Mode of Delivery and Neonatal Outcome in Adolescent Pregnancy (13–16 Years Old) Associated with Anemia
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
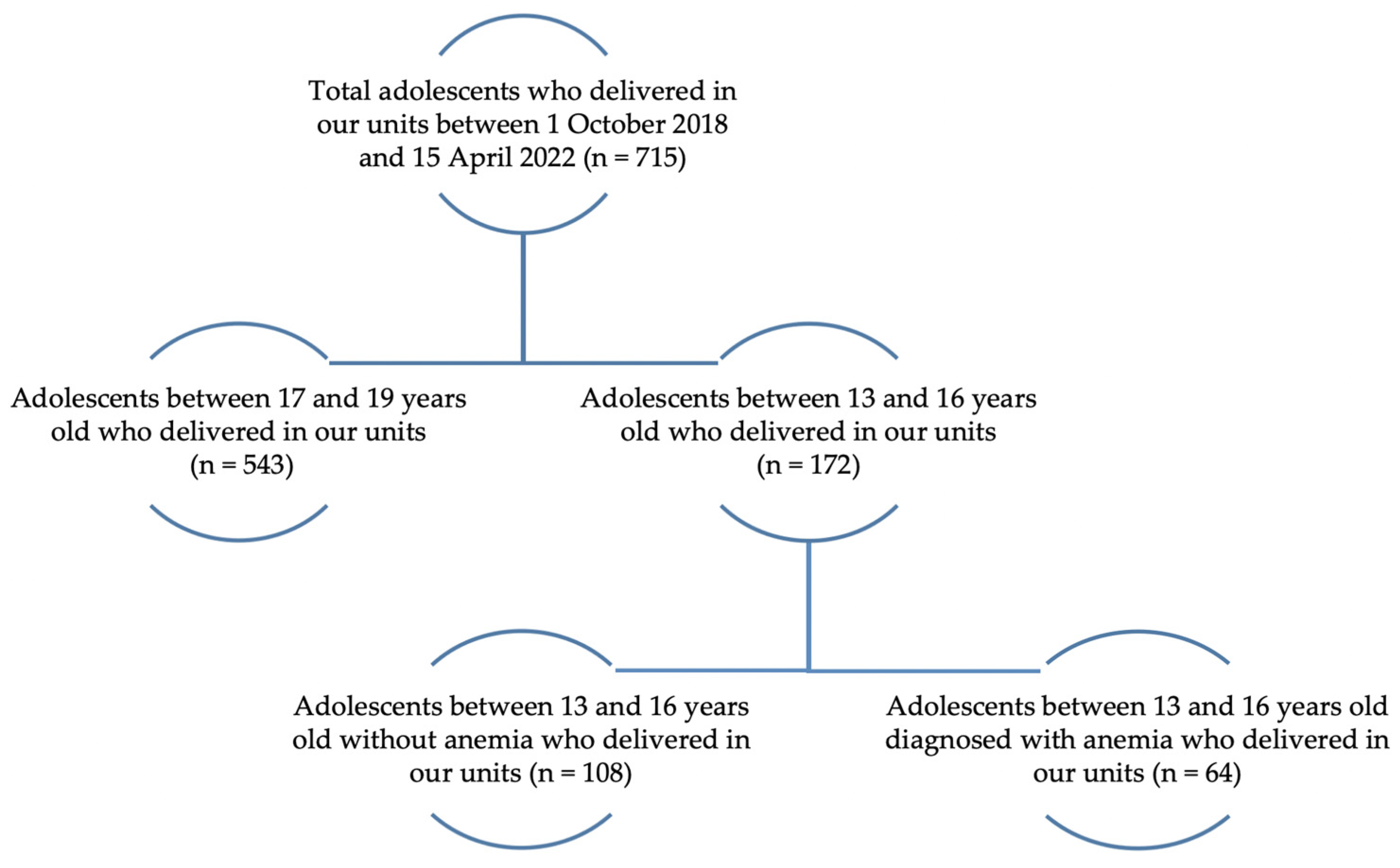
2.1. Study Design
2.2. Clinical Evaluation and Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kassa, G.M.; Arowojolu, A.O.; Odukogbe, A.A.; Yalew, A.W. Prevalence and Determinants of Adolescent Pregnancy in Africa: A Systematic Review and Meta-Analysis. Reprod. Health 2018, 15, 195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganchimeg, T.; Ota, E.; Morisaki, N.; Laopaiboon, M.; Lumbiganon, P.; Zhang, J.; Yamdamsuren, B.; Temmerman, M.; Say, L.; Tunçalp, Ö.; et al. Pregnancy and Childbirth Outcomes among Adolescent Mothers: A World Health Organization Multicountry Study. BJOG Int. J. Obstet. Gynaecol. 2014, 121 (Suppl. S1), 40–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genç, S.; Ciftci, M.A.; Cingillioglu, B.; Akturk, E.; Sahin, O.; Kukrer, S.; Yurci, A.; Mihmanli, V. Adverse Obstetric Outcomes in Early and Late Adolescent Pregnancy. J. Exp. Clin. Med. 2022, 391, 237–244. [Google Scholar] [CrossRef]
- WHO. Guidelines on Preventing Early Pregnancy and Poor Reproductive Health Outcomes among Adolescents in Developing Countries; WHO Guidelines Approved by the Guidelines Review Committee; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Wado, Y.D.; Sully, E.A.; Mumah, J.N. Pregnancy and Early Motherhood among Adolescents in Five East African Countries: A Multi-Level Analysis of Risk and Protective Factors. BMC Pregnancy Childbirth 2019, 19, 59. [Google Scholar] [CrossRef] [PubMed]
- Darroch, J.E.; Woog, V.; Bankole, A.; Ashford, L.S. Adding It up: Costs and Benefits of Meeting the Contraceptive Needs of Adolescents; Guttmacher Institute: Washington, DC, USA, 2016. [Google Scholar]
- Torvie, A.J.; Callegari, L.S.; Schiff, M.A.; Debiec, K.E. Labor and Delivery Outcomes among Young Adolescents. Am. J. Obstet. Gynecol. 2015, 213, e1–e95. [Google Scholar] [CrossRef]
- Chen, C.-W.; Tsai, C.-Y.; Sung, F.-C.; Lee, Y.-Y.; Lu, T.-H.; Li, C.-Y.; Ko, M.-C. Adverse Birth Outcomes among Pregnancies of Teen Mothers: Age-Specific Analysis of National Data in Taiwan. Child Care Health Dev. 2010, 36, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Archived: Iron Deficiency Anaemia: Assessment, Prevention and Control. Available online: https://www.who.int/publications/m/item/iron-children-6to23--archived-iron-deficiency-anaemia-assessment-prevention-and-control (accessed on 10 November 2022).
- Neal, S.; Matthews, Z.; Frost, M.; Fogstad, H.; Camacho, A.V.; Laski, L. Childbearing in Adolescents Aged 12-15 Years in Low Resource Countries: A Neglected Issue. New Estimates from Demographic and Household Surveys in 42 Countries. Acta Obstet. Gynecol. Scand. 2012, 91, 1114–1118. [Google Scholar] [CrossRef]
- Moran, V.H. A Systematic Review of Dietary Assessments of Pregnant Adolescents in Industrialised Countries. Br. J. Nutr. 2007, 97, 411–425. [Google Scholar] [CrossRef] [Green Version]
- Msuya, S.E.; Hussein, T.H.; Uriyo, J.; Sam, N.E.; Stray-Pedersen, B. Anaemia among Pregnant Women in Northern Tanzania: Prevalence, Risk Factors and Effect on Perinatal Outcomes. Tanzan. J. Health Res. 2011, 13, 33–39. [Google Scholar] [CrossRef] [Green Version]
- Balcı, E.; Sonkaya, Z.İ.; Göçer, Ş. Assessment of Maternal and Fetal Outcomes in Adolescent and Non-Adolescent Pregnant Women. East J. Med. 2020, 25, 19–25. [Google Scholar] [CrossRef]
- Conde-Agudelo, A.; Belizán, J.M.; Lammers, C. Maternal-Perinatal Morbidity and Mortality Associated with Adolescent Pregnancy in Latin America: Cross-Sectional Study. Am. J. Obstet. Gynecol. 2005, 192, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, T.; Rehman, A.U.; Tserenpil, G.; Siddiqui, F.; Ahmed, M.; Siraj, F.; Kumar, B. The Association between Iron-Deficiency Anemia and Adverse Pregnancy Outcomes: A Retrospective Report from Pakistan. Cureus 2019, 11, e5854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parks, S.; Hoffman, M.K.; Goudar, S.S.; Patel, A.; Saleem, S.; Ali, S.A.; Goldenberg, R.L.; Hibberd, P.L.; Moore, J.; Wallace, D.; et al. Maternal Anaemia and Maternal, Fetal, and Neonatal Outcomes in a Prospective Cohort Study in India and Pakistan. BJOG Int. J. Obstet. Gynaecol. 2019, 126, 737–743. [Google Scholar] [CrossRef] [PubMed]
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.-B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, Regional, and National Estimates of Levels of Preterm Birth in 2014: A Systematic Review and Modelling Analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Recommended Definitions, Terminology and Format for Statistical Tables Related to the Perinatal Period and Use of a New Certificate for Cause of Perinatal Deaths. Modifications Recommended by FIGO as Amended 14 October 1976. Acta Obstet. Gynecol. Scand. 1977, 56, 247–253. [Google Scholar]
- Nair, M.; Choudhury, M.K.; Choudhury, S.S.; Kakoty, S.D.; Sarma, U.C.; Webster, P.; Knight, M. Association between Maternal Anaemia and Pregnancy Outcomes: A Cohort Study in Assam, India. BMJ Glob. Health 2016, 1, e000026. [Google Scholar] [CrossRef] [Green Version]
- Bora, R.; Sable, C.; Wolfson, J.; Boro, K.; Rao, R. Prevalence of Anemia in Pregnant Women and Its Effect on Neonatal Outcomes in Northeast India. J. Matern.-Fetal Neonatal Med. 2014, 27, 887–891. [Google Scholar] [CrossRef]
- Akhter, S.; Momen, M.A.; Rahman, M.M.; Parveen, T.; Karim, R.K. Effect of Maternal Anemia on Fetal Outcome. Mymensingh Med. J. 2010, 19, 391–398. [Google Scholar]
- Mahamuda, B.; Tanira, S.; Feroza, W.; Perven, H.; Shamim, A. Effects of Maternal Anaemia on Neonatal Outcome—A Study Done in the Specialized Urban Hospital Set up in Bangladesh. Bangladesh J. Med. Sci. 2011, 10, 177–180. [Google Scholar] [CrossRef]
- Elhassan, E.M.; Abbaker, A.O.; Haggaz, A.D.; Abubaker, M.S.; Adam, I. Anaemia and Low Birth Weight in Medani, Hospital Sudan. BMC Res. Notes 2010, 3, 181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adam, I.; Elhassan, E.M.; Haggaz, A.E.D.; Ali, A.A.A.; Adam, G.K. A Perspective of the Epidemiology of Malaria and Anaemia and Their Impact on Maternal and Perinatal Outcomes in Sudan. J. Infect. Dev. Ctries. 2011, 5, 83–87. [Google Scholar] [CrossRef] [Green Version]
- Ali, A.A.; Rayis, D.A.; Abdallah, T.M.; Elbashir, M.I.; Adam, I. Severe Anaemia Is Associated with a Higher Risk for Preeclampsia and Poor Perinatal Outcomes in Kassala Hospital, Eastern Sudan. BMC Res. Notes 2011, 4, 311. [Google Scholar] [CrossRef]
- Pathak, P.; Singh, P.; Kapil, U.; Raghuvanshi, R.S. Prevalence of Iron, Vitamin A, and Iodine Deficiencies amongst Adolescent Pregnant Mothers. Indian J. Pediatr. 2003, 70, 299–301. [Google Scholar] [CrossRef]
- Aruda, M.M.; Waddicor, K.; Frese, L.; Cole, J.C.M.; Burke, P. Early Pregnancy in Adolescents: Diagnosis, Assessment, Options Counseling, and Referral. J. Pediatr. Health Care 2010, 24, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Young, M.F.; Oaks, B.M.; Tandon, S.; Martorell, R.; Dewey, K.G.; Wendt, A.S. Maternal Hemoglobin Concentrations across Pregnancy and Maternal and Child Health: A Systematic Review and Meta-Analysis. Ann. N. Y. Acad. Sci. 2019, 1450, 47–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronkainen, J.; Lowry, E.; Heiskala, A.; Uusitalo, I.; Koivunen, P.; Kajantie, E.; Vääräsmäki, M.; Järvelin, M.-R.; Sebert, S. Maternal Hemoglobin Associates with Preterm Delivery and Small for Gestational Age in Two Finnish Birth Cohorts. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 238, 44–48. [Google Scholar] [CrossRef]
- Badfar, G.; Shohani, M.; Soleymani, A.; Azami, M. Maternal Anemia during Pregnancy and Small for Gestational Age: A Systematic Review and Meta-Analysis. J. Matern.-Fetal Neonatal Med. 2019, 32, 1728–1734. [Google Scholar] [CrossRef] [PubMed]
- Drukker, L.; Hants, Y.; Farkash, R.; Ruchlemer, R.; Samueloff, A.; Grisaru-Granovsky, S. Iron Deficiency Anemia at Admission for Labor and Delivery Is Associated with an Increased Risk for Cesarean Section and Adverse Maternal and Neonatal Outcomes. Transfusion 2015, 55, 2799–2806. [Google Scholar] [CrossRef]
- Yılmaz, E.; Işıtan, Ö.Y.; Soysal, Ç.; Yılmaz, Z.V.; Kara, O.F.; Küçüközkan, T. The Influence of Anemia on Maternal and Neonatal Outcomes in Adolescent Pregnant. J. Surg. Med. 2018, 2, 69–73. [Google Scholar] [CrossRef] [Green Version]
- Adolescent Pregnancy in Romania Report.Pdf. Available online: https://www.unicef.org/romania/media/4081/file/Adolescent%20Pregnancy%20in%20Romania%20Report.pdf (accessed on 15 November 2022).
- Mahavarkar, S.H.; Madhu, C.K.; Mule, V.D. A Comparative Study of Teenage Pregnancy. J. Obstet. Gynaecol. J. Inst. Obstet. Gynaecol. 2008, 28, 604–607. [Google Scholar] [CrossRef]
- Leppälahti, S.; Gissler, M.; Mentula, M.; Heikinheimo, O. Is Teenage Pregnancy an Obstetric Risk in a Welfare Society? A Population-Based Study in Finland, from 2006 to 2011. BMJ Open 2013, 3, e003225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneck, M.E.; Sideras, K.S.; Fox, R.A.; Dupuis, L. Low-Income Pregnant Adolescents and Their Infants: Dietary Findings and Health Outcomes. J. Am. Diet. Assoc. 1990, 90, 555–558. [Google Scholar] [CrossRef] [PubMed]
- Gadowsky, S.L.; Gale, K.; Wolfe, S.A.; Jory, J.; Gibson, R.; O’Connor, D.L. Biochemical Folate, B12, and Iron Status of a Group of Pregnant Adolescents Accessed through the Public Health System in Southern Ontario. J. Adolesc. Health 1995, 16, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Reifsnider, E.; Gill, S.L. Nutrition for the Childbearing Years. J. Obstet. Gynecol. Neonatal Nurs. 2000, 29, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Seymour, J. Poverty in Plenty: A Human Development Report for the UK, 1st ed.; Routledge: London, UK, 2000. [Google Scholar] [CrossRef]
- Tomashek, K.M.; Ananth, C.V.; Cogswell, M.E. Risk of Stillbirth in Relation to Maternal Haemoglobin Concentration during Pregnancy. Matern. Child. Nutr. 2006, 2, 19–28. [Google Scholar] [CrossRef]
- Basbug, A.; Sonmez, C.İ. Iron Deficiency Anemia in Adolescent Pregnancy: Investigation of Its Effects and the Related Factors. Fam. Pract. Palliat. Care 2018, 3, 108–112. [Google Scholar] [CrossRef] [Green Version]
- Sekhar, D.L.; Murray-Kolb, L.E.; Kunselman, A.R.; Weisman, C.S.; Paul, I.M. Differences in Risk Factors for Anemia Between Adolescent and Adult Women. J. Womens Health 2016, 25, 505–513. [Google Scholar] [CrossRef] [Green Version]
- Casanueva, E.; Magaña, L.; Pfeffer, F.; Baez, A. Incidence of Premature Rupture of Membranes in Pregnant Women with Low Leukocyte Levels of Vitamin C. Eur. J. Clin. Nutr. 1991, 45, 401–405. [Google Scholar]
- Shi, H.; Chen, L.; Wang, Y.; Sun, M.; Guo, Y.; Ma, S.; Wang, X.; Jiang, H.; Wang, X.; Lu, J.; et al. Severity of Anemia During Pregnancy and Adverse Maternal and Fetal Outcomes. JAMA Netw. Open 2022, 5, e2147046. [Google Scholar] [CrossRef]
- Kawakita, T.; Wilson, K.; Grantz, K.L.; Landy, H.J.; Huang, C.-C.; Gomez-Lobo, V. Adverse Maternal and Neonatal Outcomes in Adolescent Pregnancy. J. Pediatr. Adolesc. Gynecol. 2016, 29, 130–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinho-Pompeu, M.; Surita, F.G.; Pastore, D.A.; Paulino, D.S.M.; Pinto, E.; Silva, J.L. Anemia in Pregnant Adolescents: Impact of Treatment on Perinatal Outcomes. J. Matern.-Fetal Neonatal Med. 2017, 30, 1158–1162. [Google Scholar] [CrossRef]
- Shipala, E.K.; Sowayi, G.; Kagwiria, M.P.; Were, E.O. Prevalence of Anemia Among Teenage Pregnant Girls Attending Antenatal Clinic in Two Health Facilities in Bungoma District, Western Kenya. J. Biol. Agric. Healthc. 2013, 3, 23–40. [Google Scholar]
- Toteja, G.S.; Singh, P.; Dhillon, B.S.; Saxena, B.N.; Ahmed, F.U.; Singh, R.P.; Prakash, B.; Vijayaraghavan, K.; Singh, Y.; Rauf, A.; et al. Prevalence of Anemia among Pregnant Women and Adolescent Girls in 16 Districts of India. Food Nutr. Bull. 2006, 27, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Shah, T.; Khaskheli, M.S.; Ansari, S.; Lakhan, H.; Shaikh, F.; Zardari, A.A.; Warsi, J.; Rind, N.A.; Rind, K.H.; Shar, A.H. Gestational Anemia and Its Effects on Neonatal Outcome, in the Population of Hyderabad, Sindh, Pakistan. Saudi J. Biol. Sci. 2022, 29, 83–87. [Google Scholar] [CrossRef]
- Uzunov, A.V.; Bohiltea, R.E.; Munteanu, O.; Nemescu, D.; Cirstoiu, M.M. A Retrospective Study Regarding the Method of Delivery of Adolescents in a Romanian Hospital. Exp. Ther. Med. 2020, 20, 2444–2448. [Google Scholar] [CrossRef]
- Khaniya, B. Maternal and Perinatal Outcome in Adolescent Pregnancies as Compared to Adult Pregnancies. Nepal J. Health Sci. 2021, 1, 43–47. [Google Scholar] [CrossRef]
- Ferguson, M.T.; Dennis, A.T. Defining Peri-Operative Anaemia in Pregnant Women-Challenging the Status Quo. Anaesthesia 2019, 74, 237–245. [Google Scholar] [CrossRef] [Green Version]
- Weiser, T.G.; Haynes, A.B.; Molina, G.; Lipsitz, S.R.; Esquivel, M.M.; Uribe-Leitz, T.; Fu, R.; Azad, T.; Chao, T.E.; Berry, W.R.; et al. Estimate of the Global Volume of Surgery in 2012: An Assessment Supporting Improved Health Outcomes. Lancet Lond. Engl. 2015, 385 (Suppl. 2), S11. [Google Scholar] [CrossRef] [PubMed]
- Youssry, M.; Radwan, A.; Gebreel, M.; Patel, T. Prevalence of Maternal Anemia in Pregnancy: The Effect of Maternal Hemoglobin Level on Pregnancy and Neonatal Outcome. Open J. Obstet. Gynecol. 2018, 8, 676–687. [Google Scholar] [CrossRef] [Green Version]
- Muñoz, M.; Acheson, A.G.; Auerbach, M.; Besser, M.; Habler, O.; Kehlet, H.; Liumbruno, G.M.; Lasocki, S.; Meybohm, P.; Rao Baikady, R.; et al. International Consensus Statement on the Peri-Operative Management of Anaemia and Iron Deficiency. Anaesthesia 2017, 72, 233–247. [Google Scholar] [CrossRef] [Green Version]
- Hammad, I.A.; Chauhan, S.P.; Magann, E.F.; Abuhamad, A.Z. Peripartum Complications with Cesarean Delivery: A Review of Maternal-Fetal Medicine Units Network Publications. J. Matern.-Fetal Neonatal Med. 2014, 27, 463–474. [Google Scholar] [CrossRef]
- Brosens, I.; Pijnenborg, R.; Vercruysse, L.; Romero, R. The “Great Obstetrical Syndromes” Are Associated with Disorders of Deep Placentation. Am. J. Obstet. Gynecol. 2011, 204, 193–201. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, K.; Matsushima, S.; Urayama, K.Y.; Kikuchi, N.; Nakamura, N.; Tanigaki, S.; Sago, H.; Satoh, S.; Saito, S.; Morisaki, N. Association between Adolescent Pregnancy and Adverse Birth Outcomes, a Multicenter Cross Sectional Japanese Study. Sci. Rep. 2019, 9, 2365. [Google Scholar] [CrossRef]
- Yadav, S.; Choudhary, D.; Narayan, K.C.; Mandal, R.K.; Sharma, A.; Chauhan, S.S.; Agrawal, P. Adverse Reproductive Outcomes Associated with Teenage Pregnancy. McGill J. Med. 2008, 11, 141–144. [Google Scholar] [CrossRef]
- Labib, H.; Ahmed, A.; Abdelmoaty, M. Effect of Moderate Iron Deficiency Anemia during Pregnancy on Maternal and Fetal Outcome. Al-Azhar Int. Med. J. 2021, 2, 41–45. [Google Scholar] [CrossRef]
- Marvin-Dowle, K.; Kilner, K.; Burley, V.J.; Soltani, H. Impact of Adolescent Age on Maternal and Neonatal Outcomes in the Born in Bradford Cohort. BMJ Open 2018, 8, e016258. [Google Scholar] [CrossRef]
- Asrat, D.T.; Below, E.H.; Teklay, H.A.; Tesfamaryam, L.S.; Weldemaryam, R.Z.; Teweldebrhan, S.S.; Gebreweldi, F.H.; Gebregziabher, N.K.; Giliu, S.M. Adverse Reproductive Outcomes Associated with Teenage Pregnancy in Three Maternity Hospitals in Asmara, Eritrea. Am. J. Nurs. Health Sci. 2020, 1, 15. [Google Scholar] [CrossRef]
- Jusoh, N.; Ismail, T.A.; Daud, A. Anemia Among Teenage Pregnancy in Northwestern Malaysia: What Are the Factors? Int. J. Collab. Res. Intern. Med. Public Health 2015, 7, 196–205. [Google Scholar]
- Baş, E.K.; Bülbül, A.; Uslu, S.; Baş, V.; Elitok, G.K.; Zubarioğlu, U. Maternal Characteristics and Obstetric and Neonatal Outcomes of Singleton Pregnancies Among Adolescents. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e919922-e1. [Google Scholar] [CrossRef]
- Medhi, R.; Das, B.; Das, A.; Ahmed, M.; Bawri, S.; Rai, S. Adverse Obstetrical and Perinatal Outcome in Adolescent Mothers Associated with First Birth: A Hospital-Based Case-Control Study in a Tertiary Care Hospital in North-East India. Adolesc. Health Med. Ther. 2016, 7, 37–42. [Google Scholar] [CrossRef]


{kind=link}
| Study Group (<11 g/dL) (n = 64) | Control Group (>11 g/dL) (n = 108) | p-Value * | |
|---|---|---|---|
| Maternal age (mean ± SD) | 15.26 ± 0.78 | 15.41 ± 0.72 | <0.001 |
| Area of residence (n, %) | |||
| Urban | 31 (48.43%) | 38 (35.18%) | 0.009 |
| Rural | 33 (51.57%) | 70 (64.82%) | |
| Maternal weight (n, %) | |||
| Normoponderal | 63 (98.43%) | 106 (98.14%) | 0.045 |
| Overweight (BMI—25–30 kg/m2) | 1 (1.57%) | 2 (1.86%) | |
| Type of anemia (n, %) | |||
| Iron-deficiency anemia | 57 (89.06%) | - | N/A |
| Megaloblastic anemia | 2 (3.13%) | - | |
| β-thalassemia minor | 5 (7.81%) | - | |
| Parity (n, %) | |||
| Primiparous | 55 (85.93%) | 90 (83.33%) | <0.001 |
| Multiparous | 9 (14.07%) | 18 (16.67%) | |
| Prenatal care (n, %) | |||
| Yes | 6 (9.37%) | 18 (16.67%) | 0.034 |
| No | 58 (90.63%) | 90 (83.33%) | |
| Mode of delivery (n, %) | |||
| Cesarean section | 29 (45.31%) | 42 (38.89%) | <0.001 |
| Preeclampsia | 6 (9.38%) | 4 (3.70%) | |
| Negative induction of labor | 8 (12.5%) | 2 (1.85%) | |
| Cephalo-pelvic disproportion | 4 (6.25%) | 12 (11.11%) | |
| Dystocia presentation | 2 (3.12%) | 2 (1.85%) | |
| Fetal distress | 7 (10.94%) | 16 (14.81%) | |
| Uterine scar after cesarean section | 2 (3.12%) | 6 (5.56%) | |
| Vaginal delivery | 35 (54.69%) | 66 (61.11%) | 0.411 |
| GA at delivery (weeks) (mean ± SD) | 36.73 ± 3.20 | 37.12 ± 2.47 | 0.539 |
| Neonatal outcomes | |||
| Preterm birth (n, %) | 23 (35.93%) | 23 (21.29%) | <0.001 |
| Birth weight (grams) (mean ± SD) | 2829.84 ± 620.40 | 2888.13 ± 599.24 | 0.396 |
| 1-min Apgar score (mean ± SD) | 8.48 ± 1.39 | 8.62 ± 1.65 | 0.812 |
| NICU admission, (n, %) | 6 (9.38%) | 9 (8.33%) | 0.980 |
| Patient’s Age | Hemoglobin Level (n/%) | ||||||
|---|---|---|---|---|---|---|---|
| Control Group (>11 g/dL) | Study Group (<11 g/dL) | p-Value | |||||
| Total | Mild Anemia (9–10.9 g/dL) | Moderate Anemia (7–8.9 g/dL) | Severe Anemia (<7 g/dL) | ||||
| 14 years | 26 | 15 (57.69%) | 11 (42.31%) | 11 (22.00%) | - | - | 0.251 |
| 15 years | 57 | 33 (57.89%) | 24 (42.11%) | 17 (34.00%) | 7 (53.84%) | - | 0.455 |
| 16 years | 89 | 60 (67.41%) | 29 (32.58%) | 22 (44.00%) | 6 (46.16%) | 1 (100%) | <0.001 |
| Hemoglobin Level (n/%) | |||||||
|---|---|---|---|---|---|---|---|
| Control Group (>11 g/dL) | Study Group (<11 g/dL) | p-Value | |||||
| Total | Mild Anemia (9–10.9 g/dL) | Moderate Anemia (7–8.9 g/dL) | Severe Anemia (<7 g/dL) | ||||
| Time of delivery | |||||||
| Preterm birth | 46 | 23 (21.29%) | 23 (35.93%) | 17 (34.00%) | 6 (46.15.%) | - | <0.001 |
| Term delivery | 126 | 85 (78.71%) | 41 (64.07%) | 33 (66.00%) | 7 (53.85%) | 1 (100%) | 0.037 |
| Mode of delivery | |||||||
| Cesarean section | 71 | 42 (38.88%) | 29 (45.31%) | 25 (50%) | 4 (30.76%) | - | <0.001 |
| Vaginal delivery | 101 | 66 (61.11%) | 35 (54.69%) | 25 (50%) | 9 (69.24%) | 1 (100%) | 0.411 |
| Cases | Patient’s Age | |||||
|---|---|---|---|---|---|---|
| Control Group | Study Group | p-Value | ||||
| 14 Years (n = 11) | 15 Years (n = 24) | 16 Years (n = 29) | ||||
| Time of delivery | ||||||
| Preterm birth | 46 | 23 (34.25%) | 5 (45.45%) | 11 (45.83%) | 7 (24.13%) | <0.001 |
| Term delivery | 126 | 85 (65.75%) | 6 (54.55%) | 13 (54.17%) | 22 (75.87%) | 0.014 |
| Mode of delivery | ||||||
| Cesarean section | 71 | 42 (38.88%) | 5 (45.45%) | 9 (37.5%) | 15 (51.72%) | 0.363 |
| Vaginal delivery | 101 | 66 (61.12%) | 6 (54.55%) | 15 (62.5%) | 14 (48.28%) | <0.001 |
| 1-min Apgar Score | Cases | Hemoglobin Level (n, %) | ||||||
|---|---|---|---|---|---|---|---|---|
| Control Group (>11 g/dL) | Study Group (>11 g/dL) | |||||||
| Total | Mild Anemia (9–10.9 g/dL) | Moderate Anemia (7–8.9 g/dL) | Severe Anemia (<7 g/dL) | p-Value | ||||
| Extremely low | 0–3 | 3 | 2 (1.85%) | 1 (1.56%) | 1 (2%) | - | - | 0.420 |
| Abnormal | 4–6 | 5 | 4 (3.70%) | 1 (1.56%) | 1 (2%) | - | - | 0.403 |
| Reassuring | 7–10 | 164 | 102 (94.44%) | 62 (96.87%) | 48 (96%) | 13 (100%) | 1 (100%) | 0.638 |
| 1-min Apgar Score | Cases | Patient’s Age | ||||||
|---|---|---|---|---|---|---|---|---|
| Control Group (n = 108) | Study Group | p-Value | ||||||
| Total | 14 Years (n = 11) | 15 Years (n = 24) | 16 Years (n = 29) | |||||
| Extremely low | 0–3 | 3 | 2 (1.85%) | 1 (1.56%) | - | 1 (4.16%) | - | 0.667 |
| Abnormal | 4–6 | 5 | 4 (3.70%) | 1 (1.56%) | - | 1 (4.16%) | - | 0.055 |
| Reassuring | 7–10 | 164 | 102 (94.44%) | 62 (96.87%) | 11 (100%) | 22 (91.66%) | 29 (100%) | 0.055 |
| Newborns’ Weights | Cases | Hemoglobin Levels (n, %) | ||||||
|---|---|---|---|---|---|---|---|---|
| Control Group (>11 g/dL) | Study Group | |||||||
| Total | Mild Anemia (9–10.9 g/dL) | Moderate Anemia (7–8.9 g/dL) | Severe Anemia (<7 g/dL) | p-Value | ||||
| ELBW | <1.000 g | 3 | 2 (1.85%) | 1 (1.56%) | 1 (2.00%) | - | - | 0.003 |
| VLBW | 1.000–1.499 g | 2 | - | 1 (1.56%) | 1 (2.00%) | - | - | N/A |
| LBW | 1.500–2.499 g | 32 | 20 (18.51%) | 14 (21.87%) | 11 (22.00%) | 3 (23.07%) | - | 0.632 |
| NBW | 2.500–4.000 g | 134 | 85 (78.70%) | 48 (75.00%) | 37 (74.00%) | 10 (76.93%) | 1 (100%) | 0.867 |
| >4.000 g | 1 | 1 (0.92%) | - | - | - | - | N/A | |
| Newborns’ Weights | Cases | Patients’ Ages (n/%) | |||||
|---|---|---|---|---|---|---|---|
| Control Group | 14 Years | 15 Years | 16 Years | p-Value | |||
| ELBW | <1.000 g | 3 | 2 (1.85%) | - | 1 (4.16%) | - | 0.035 |
| VLBW | 1.000–1.499 g | 2 | - | - | 2 (8.33%) | - | N/A |
| LBW | 1.500–2.499 g | 32 | 22 (20.37%) | 4 (36.36%) | 3 (12.50%) | 3 (10.34%) | <0.001 |
| NBW | 2.500–4.000 g | 134 | 83 (76.85%) | 7 (63.63%) | 18 (75.00%) | 26 (89.66%) | <0.001 |
| >4000 g | 1 | 1 (0.92%) | - | - | - | N/A | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uzunov, A.V.; Cîrstoiu, M.M.; Secară, D.C.; Crîngu-Ionescu, A.; Matei, A.; Mehedințu, C.; Varlas, V.N. Mode of Delivery and Neonatal Outcome in Adolescent Pregnancy (13–16 Years Old) Associated with Anemia. Medicina 2022, 58, 1796. https://doi.org/10.3390/medicina58121796
Uzunov AV, Cîrstoiu MM, Secară DC, Crîngu-Ionescu A, Matei A, Mehedințu C, Varlas VN. Mode of Delivery and Neonatal Outcome in Adolescent Pregnancy (13–16 Years Old) Associated with Anemia. Medicina. 2022; 58(12):1796. https://doi.org/10.3390/medicina58121796
Chicago/Turabian StyleUzunov, Ana Veronica, Monica Mihaela Cîrstoiu, Diana Cristina Secară, Antoniu Crîngu-Ionescu, Alexandra Matei, Claudia Mehedințu, and Valentin Nicolae Varlas. 2022. "Mode of Delivery and Neonatal Outcome in Adolescent Pregnancy (13–16 Years Old) Associated with Anemia" Medicina 58, no. 12: 1796. https://doi.org/10.3390/medicina58121796