
The Association of Peripheral T Lymphocyte Subsets Disseminated Infection by Mycobacterium Tuberculosis in HIV-Negative Patients: A Retrospective Observational Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
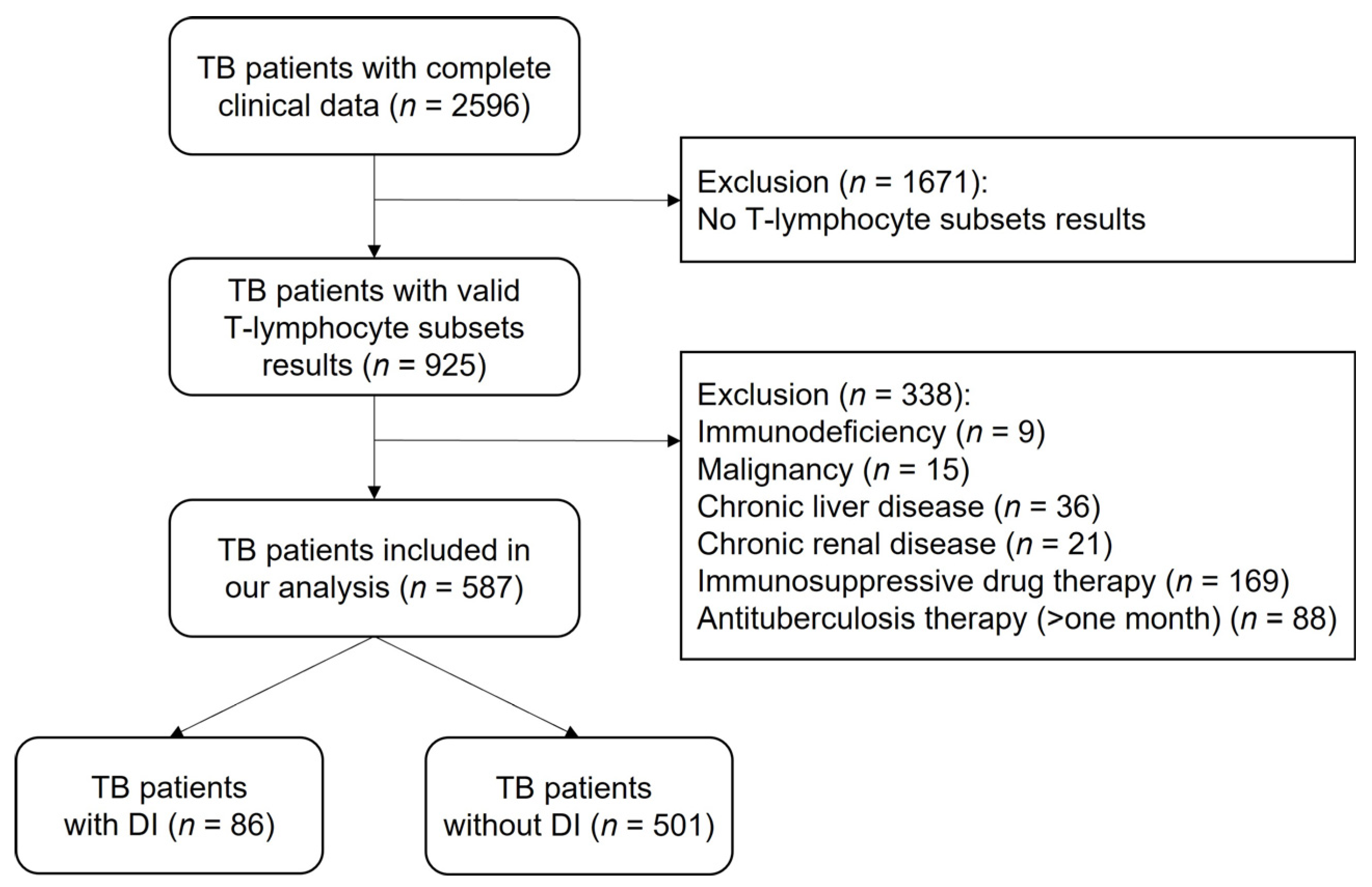
2.1. Study Population and Ethics Approval
2.2. Case Definitions
2.3. Lymphocyte Subset Assays
2.4. Data Management and Statistical Analysis
3. Results
3.1. Participant Characteristics
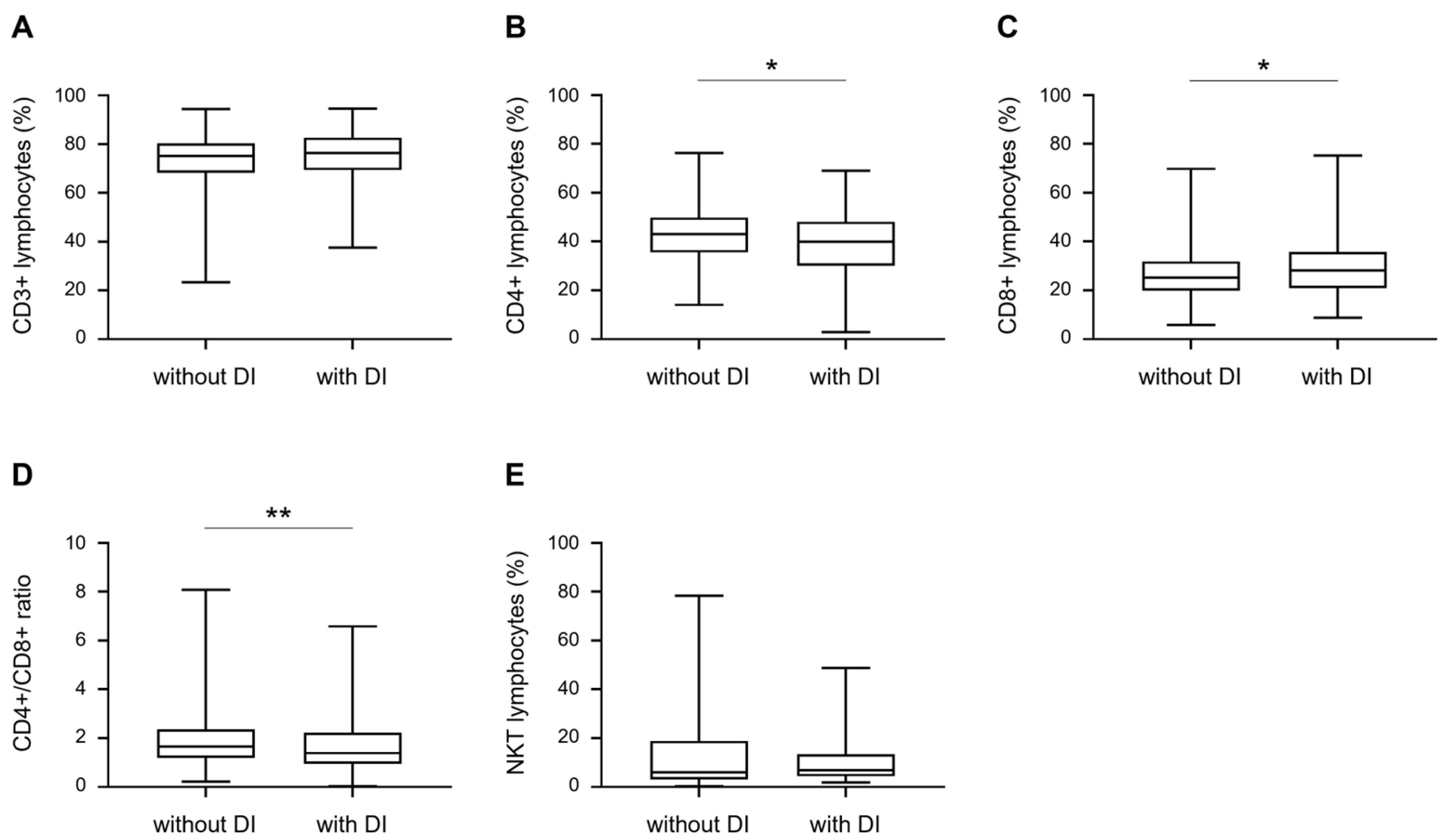
3.2. Comparison of T Lymphocyte Subsets between TB Patients with and without DI
3.3. Univariate Analysis of the Other Factors Associated with DI
3.4. Multiple Logistic Regression Analysis of the Factors Associated with DI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2021. Available online: https://www.aidsdatahub.org/resource/global-tuberculosis-report-2021 (accessed on 30 August 2022).
- Peloquin, C.A.; Davies, G.R. The Treatment of Tuberculosis. Clin Pharmacol. Ther. 2021, 110, 1455–1466. [Google Scholar] [CrossRef] [PubMed]
- Furin, J.; Cox, H.; Pai, M. Tuberculosis. Lancet 2019, 393, 1642–1656. [Google Scholar] [CrossRef]
- Pang, Y.; An, J.; Shu, W.; Huo, F.; Chu, N.; Gao, M.; Qin, S.; Huang, H.; Chen, X.; Xu, S. Epidemiology of Extrapulmonary Tuberculosis among Inpatients, China, 2008-2017. Emerg. Infect. Dis. 2019, 25, 457–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravesloot-Chavez, M.M.; Van Dis, E.; Stanley, S.A. The Innate Immune Response to Mycobacterium tuberculosis Infection. Annu. Rev. Immunol. 2021, 39, 611–637. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.K.; Mohan, A.; Kohli, M. Extrapulmonary tuberculosis. Expert Rev. Respir. Med. 2021, 15, 931–948. [Google Scholar] [CrossRef] [PubMed]
- Corleis, B.; Bucsan, A.N.; Deruaz, M.; Vrbanac, V.D.; Lisanti-Park, A.C.; Gates, S.J.; Linder, A.; Paer, J.M.; Olson, G.; Bowman, B.A.; et al. HIV-1 and SIV Infection Are Associated with Early Loss of Lung Interstitial CD4+ T Cells and Dissemination of Pulmonary Tuberculosis. Cell Rep. 2019, 26, 1409–1418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moule, M.G.; Cirillo, J.D. Mycobacterium tuberculosis Dissemination Plays a Critical Role in Pathogenesis. Front. Cell Infect. Microbiol. 2020, 10, 65. [Google Scholar] [CrossRef]
- Sharma, S.K.; Mohan, A.; Sharma, A.; Mitra, D.K. Miliary tuberculosis: New insights into an old disease. Lancet Infect. Dis. 2005, 5, 415–430. [Google Scholar] [CrossRef]
- Donovan, J.; Figaji, A.; Imran, D.; Phu, N.H.; Rohlwink, U.; Thwaites, G.E. The neurocritical care of tuberculous meningitis. Lancet Neurol. 2019, 18, 771–783. [Google Scholar] [CrossRef]
- Manyelo, C.M.; Solomons, R.S.; Walzl, G.; Chegou, N.N. Tuberculous Meningitis: Pathogenesis, Immune Responses, Diagnostic Challenges, and the Potential of Biomarker-Based Approaches. J. Clin. Microbiol. 2021, 59, e01771-20. [Google Scholar] [CrossRef]
- Scriba, T.J.; Coussens, A.K.; Fletcher, H.A. Human Immunology of Tuberculosis. Microbiol. Spectr. 2016, 5, 1. [Google Scholar]
- Sia, J.K.; Rengarajan, J. Immunology of Mycobacterium tuberculosis Infections. Microbiol. Spectr. 2019, 7, 4. [Google Scholar] [CrossRef] [PubMed]
- Yao, S.; Huang, D.; Chen, C.Y.; Halliday, L.; Wang, R.C.; Chen, Z.W. CD4+ T cells contain early extrapulmonary tuberculosis (TB) dissemination and rapid TB progression and sustain multieffector functions of CD8+ T and CD3- lymphocytes: Mechanisms of CD4+ T cell immunity. J. Immunol. 2014, 192, 2120–2132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, J.S.; Potts, R.C.; Kardjito, T.; Grange, J.M. T4 lymphopenia in patients with active pulmonary tuberculosis. Clin. Exp. Immunol. 1985, 60, 49–54. [Google Scholar]
- Jones, B.E.; Oo, M.M.; Taikwel, E.K.; Qian, D.; Kumar, A.; Maslow, E.R.; Barnes, P.F. CD4 cell counts in human immunodeficiency virus-negative patients with tuberculosis. Clin. Infect. Dis. 1997, 24, 988–991. [Google Scholar] [CrossRef] [Green Version]
- Morgan, J.; Muskat, K.; Tippalagama, R.; Sette, A.; Burel, J.; Arlehamn, C.S.L. Classical CD4 T cells as the cornerstone of antimycobacterial immunity. Immunol. Rev. 2021, 301, 10–29. [Google Scholar] [CrossRef]
- Veenstra, H.; Baumann, R.; Carroll, N.M.; Lukey, P.T.; Kidd, M.; Beyers, N.; Bolliger, C.T.; Van Helden, P.D.; Walzl, G. Changes in leucocyte and lymphocyte subsets during tuberculosis treatment; prominence of CD3dimCD56+ natural killer T cells in fast treatment responders. Clin. Exp. Immunol. 2006, 145, 252–260. [Google Scholar] [CrossRef]
- Venturini, E.; Lodi, L.; Francolino, I.; Ricci, S.; Chiappini, E.; de Martino, M.; Galli, L. CD3, CD4, CD8, CD19 and CD16/CD56 positive cells in tuberculosis infection and disease: Peculiar features in children. Int. J. Immunopathol. Pharmacol. 2019, 33, 2058738419840241. [Google Scholar] [CrossRef]
- Gaifer, Z. Epidemiology of extrapulmonary and disseminated tuberculosis in a tertiary care center in Oman. Int. J. Mycobacteriol. 2017, 6, 162–166. [Google Scholar] [CrossRef]
- de Almeida, A.S.; Fiske, C.T.; Sterling, T.R.; Kalams, S.A. Increased frequency of regulatory T cells and T lymphocyte activation in persons with previously treated extrapulmonary tuberculosis. Clin. Vaccine Immunol. 2012, 19, 45–52. [Google Scholar] [CrossRef] [Green Version]
- Lin, P.L.; Rutledge, T.; Green, A.M.; Bigbee, M.; Fuhrman, C.; Klein, E.; Flynn, J.L. CD4 T cell depletion exacerbates acute Mycobacterium tuberculosis while reactivation of latent infection is dependent on severity of tissue depletion in cynomolgus macaques. AIDS Res. Hum. Retroviruses 2012, 28, 1693–1702. [Google Scholar] [CrossRef] [Green Version]
- Sakai, S.; Kauffman, K.D.; Sallin, M.A.; Sharpe, A.H.; Young, H.A.; Ganusov, V.V.; Barber, D.L. CD4 T Cell-Derived IFN-gamma Plays a Minimal Role in Control of Pulmonary Mycobacterium tuberculosis Infection and Must Be Actively Repressed by PD-1 to Prevent Lethal Disease. PLoS Pathog. 2016, 12, e1005667. [Google Scholar] [CrossRef] [PubMed]
- Kony, S.J.; Hane, A.A.; Larouze, B.; Samb, A.; Cissoko, S.; Sow, P.; Sané, M.; Maynart, M.; Diouf, G.; Murray, J.; et al. Tuberculosis-associated severe CD4+ T-lymphocytopenia in HIV-seronegative patients from Dakar. SIDAK Research Group. J. Infect. 2000, 41, 167–171. [Google Scholar] [CrossRef] [PubMed]
- O'Garra, A.; Redford, P.S.; McNab, F.W.; Bloom, C.I.; Wilkinson, R.J.; Berry, M.P.R. The immune response in tuberculosis. Annu. Rev. Immunol. 2013, 31, 475–527. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.K.; Mitra, D.K.; Balamurugan, A.; Pandey, R.M.; Mehra, N.K. Cytokine polarization in miliary and pleural tuberculosis. J. Clin. Immunol. 2002, 22, 345–352. [Google Scholar] [CrossRef]
- Sharma, S.K.; Mohan, A. Miliary Tuberculosis. Microbiol. Spectr. 2017, 5, 2. [Google Scholar] [CrossRef]
- Chen, C.Y.; Huang, D.; Wang, R.C.; Shen, L.; Zeng, G.; Yao, S.; Shen, Y.; Halliday, L.; Fortman, J.; McAllister, M.; et al. A critical role for CD8 T cells in a nonhuman primate model of tuberculosis. PLoS Pathog. 2009, 5, e1000392. [Google Scholar] [CrossRef]
- Grotzke, J.E.; Lewinsohn, D.M. Role of CD8+ T lymphocytes in control of Mycobacterium tuberculosis infection. Microbes Infect. 2005, 7, 776–788. [Google Scholar] [CrossRef]
- Silva, B.D.S.; Trentini, M.M.; da Costa, A.C.; Kipnis, A.; Junqueira-Kipnis, A.P. Different phenotypes of CD8+ T cells associated with bacterial load in active tuberculosis. Immunol. Lett. 2014, 160, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Rozot, V.; Patrizia, A.; Vigano, S.; Mazza-Stalder, J.; Idrizi, E.; Day, C.L.; Perreau, M.; Lazor-Blanchet, C.; Ohmiti, K.; Goletti, D.; et al. Combined use of Mycobacterium tuberculosis-specific CD4 and CD8 T-cell responses is a powerful diagnostic tool of active tuberculosis. Clin. Infect. Dis. 2014, 60, 432–437. [Google Scholar] [CrossRef]
- Li, K.; Ran, R.; Jiang, Z.; Fan, C.; Li, T.; Yin, Z. Changes in T-lymphocyte subsets and risk factors in human immunodeficiency virus-negative patients with active tuberculosis. Infection 2020, 48, 585–595. [Google Scholar] [CrossRef] [PubMed]
- Cyktor, J.C.; Carruthers, B.; Beamer, G.L.; Turner, J. Clonal expansions of CD8+ T cells with IL-10 secreting capacity occur during chronic Mycobacterium tuberculosis infection. PLoS ONE 2013, 8, e58612. [Google Scholar] [CrossRef] [PubMed]
- Kviatcovsky, D.; Rivadeneyra, L.; Balboa, L.; Yokobori, N.; López, B.; Ritacco, V.; Schattner, M.; Sasiain, M.D.C.; de la Barrera, S. Mycobacterium tuberculosis Multidrug-Resistant Strain M Induces Low IL-8 and Inhibits TNF-alpha Secretion by Bronchial Epithelial Cells Altering Neutrophil Effector Functions. Mediat. Inflamm. 2017, 2017, 2810606. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Cases (n = 587) | Value | |
|---|---|---|---|
| Missing Cases | Valid Cases | ||
| Male gender, No. (%) | 0 | 587 | 390 (66.4) |
| Median age (IQR), years | 0 | 587 | 48 (29–63) |
| BMI < 18.5, No. (%) | 127 | 460 | 123 (26.7) |
| Alcohol use, No. (%) | 0 | 587 | 155 (26.4) |
| Cigarette smoking, No. (%) | 0 | 587 | 232 (39.5) |
| BCG vaccination, No. (%) | 0 | 587 | 384 (65.4) |
| Diabetes, No. (%) | 0 | 587 | 117 (19.9) |
| Retreatment *, No. (%) | 0 | 587 | 186 (31.7) |
| Number of symptoms ≥4, No. (%) | 0 | 587 | 243 (41.4) |
| Smear, positive, No. (%) | 0 | 587 | 256 (43.6) |
| Culture, positive, No. (%) | 46 | 541 | 334 (61.7) |
| Rifampicin resistant, No. (%) | 0 | 587 | 164 (27.9) |
| Albumin decreased, No. (%) | 0 | 587 | 310 (52.8%) |
| Factor | Without DI | With DI | p Value |
|---|---|---|---|
| Male gender, No. (%) | 339 (67.7) | 51 (59.3) | 0.129 |
| Age ≥ 60, No. (%) | 153 (30.5) | 23 (36.7) | 0.478 |
| BMI < 18.5, No. (%) | 106 (26.2) | 17 (30.9) | 0.456 |
| Alcohol use, No. (%) | 141 (28.1) | 14 (16.3) | 0.021 |
| Cigarette smoking, No. (%) | 211 (42.1) | 21 (24.4) | 0.002 |
| BCG vaccination, No. (%) | 321 (64.1) | 63 (73.3) | 0.098 |
| Diabetes, No. (%) | 104 (20.8) | 13 (15.1) | 0.226 |
| * Retreatment, No. (%) | 180 (35.9) | 6 (7.0) | <0.001 |
| Number of symptoms ≥ 4, No. (%) | 202 (40.3) | 41 (47.7) | 0.201 |
| Smear, positive, No. (%) | 241 (48.1) | 15 (17.4) | <0.001 |
| Culture, positive, No. (%) | 306 (64.0) | 28 (44.4) | 0.003 |
| Rifampicin resistant, No. (%) | 160 (31.9) | 4 (4.7) | <0.001 |
| Albumin decreased, No. (%) | 259 (51.7) | 51 (59.3) | 0.192 |
| Factor | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Alcohol use | |||||||||
| No | Reference | Reference | Reference | ||||||
| Yes | 0.760 | 0.320–1.800 | 0.532 | 0.753 | 0.317–1.788 | 0.520 | 0.789 | 0.331–1.879 | 0.593 |
| Cigarette smoking | |||||||||
| No | Reference | Reference | Reference | ||||||
| Yes | 0.767 | 0.367–1.601 | 0.480 | 0.766 | 0.365–1.608 | 0.481 | 0.739 | 0.350–1.557 | 0.426 |
| * Retreatment | |||||||||
| No | Reference | Reference | Reference | ||||||
| Yes | 0.297 | 0.118–0.749 | 0.010 | 0.316 | 0.126–0.793 | 0.014 | 0.305 | 0.120–0.777 | 0.013 |
| Smear | |||||||||
| Negative | Reference | Reference | Reference | ||||||
| Positive | 0.373 | 0.175–0.794 | 0.010 | 0.355 | 0.165–0.761 | 0.008 | 0.357 | 0.166–0.768 | 0.008 |
| Culture | |||||||||
| Negative | Reference | Reference | Reference | ||||||
| Positive | 0.786 | 0.405–1.524 | 0.476 | 0.841 | 0.432–1.636 | 0.610 | 0.788 | 0.403–1.541 | 0.486 |
| Rifampicin resistant | |||||||||
| No | Reference | Reference | Reference | ||||||
| Yes | 0.269 | 0.091–0.799 | 0.018 | 0.237 | 0.080–0.697 | 0.009 | 0.261 | 0.088–0.774 | 0.015 |
| CD4+ % | 0.968 | 0.936–1.002 | 0.067 | 0.967 | 0.934–1.001 | 0.054 | |||
| CD8+ % | 1.041 | 1.005–1.079 | 0.026 | 1.041 | 1.006–1.077 | 0.022 | |||
| CD4+/CD8+ ratio | 1.204 | 0.846–1.713 | 0.303 | 1.267 | 0.894–1.794 | 0.183 | 1.602 | 1.077–2.383 | 0.020 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Q.; Liu, S.; Li, X.; Yang, R.; Liang, C.; Yu, J.; Lin, W.; Liu, Y.; Yao, C.; Pang, Y.; et al. The Association of Peripheral T Lymphocyte Subsets Disseminated Infection by Mycobacterium Tuberculosis in HIV-Negative Patients: A Retrospective Observational Study. Medicina 2022, 58, 1606. https://doi.org/10.3390/medicina58111606
Li Q, Liu S, Li X, Yang R, Liang C, Yu J, Lin W, Liu Y, Yao C, Pang Y, et al. The Association of Peripheral T Lymphocyte Subsets Disseminated Infection by Mycobacterium Tuberculosis in HIV-Negative Patients: A Retrospective Observational Study. Medicina. 2022; 58(11):1606. https://doi.org/10.3390/medicina58111606
Chicago/Turabian StyleLi, Qiao, Shengsheng Liu, Xiaomeng Li, Ruifang Yang, Chen Liang, Jiajia Yu, Wenhong Lin, Yi Liu, Cong Yao, Yu Pang, and et al. 2022. "The Association of Peripheral T Lymphocyte Subsets Disseminated Infection by Mycobacterium Tuberculosis in HIV-Negative Patients: A Retrospective Observational Study" Medicina 58, no. 11: 1606. https://doi.org/10.3390/medicina58111606