
CPAP Therapy on Depressive and Anxiety Symptoms in Patients with Moderate to Severe Obstructive Sleep Apnea Syndrome

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Measurements
2.3. Self-Reported Measures
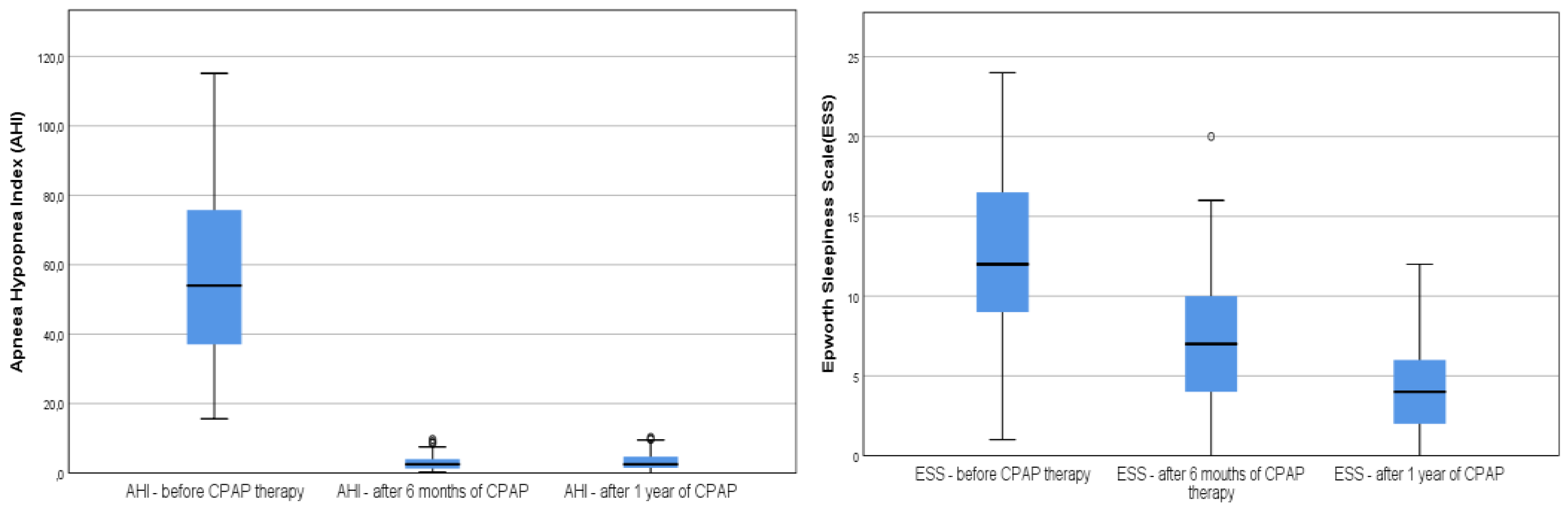
- Epworth Sleepiness Scale (ESS) was used to assess daytime sleepiness. Patients were asked to indicate the tendency to fall asleep in 8 passive or active specific situations on a 0–3 scale, with 0 meaning no chance of falling asleep and 3 showing a high chance of falling asleep. A score of 10 means excessive daytime sleepiness [16].
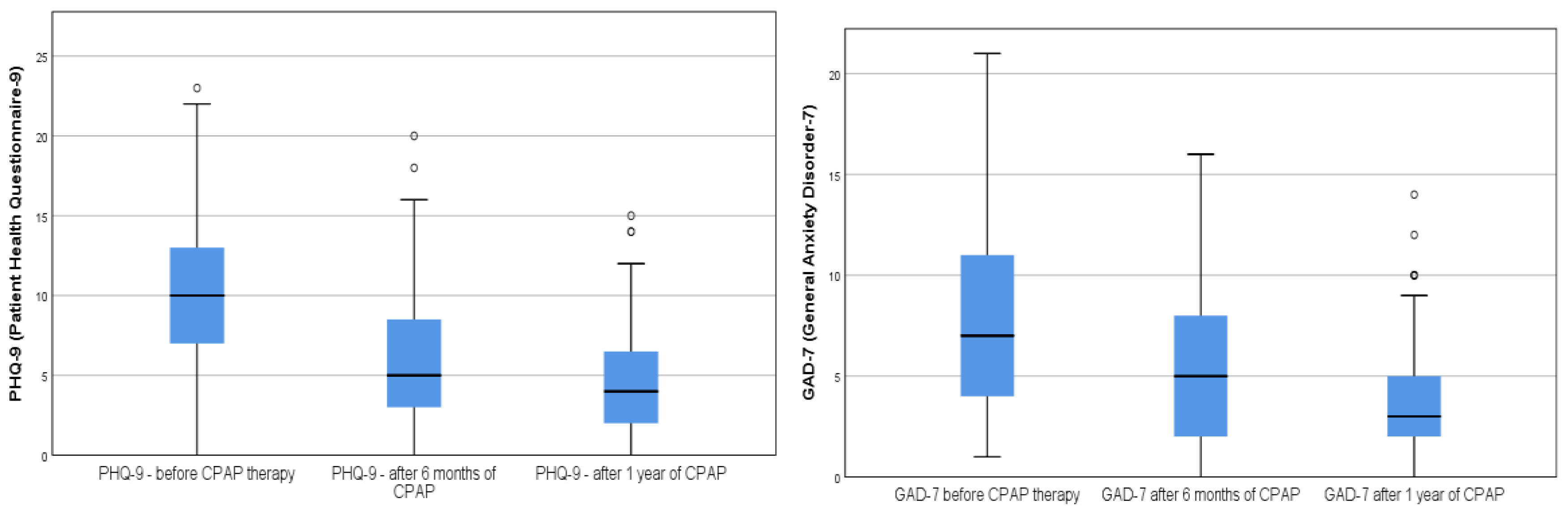
- Patient Health Questionnaire-9 Depression Scale is a self-reported validated questionnaire that is used to assess the presence and the severity of depression by primary care practitioners [17]. It can establish depressive distress as well as the grade of depressive symptoms severity. The scale consists of 9 items that assess the patient health status during the previous 2 weeks and relate to feelings of sadness, tiredness, sleepiness or sleeping too much little interest in doing things, thoughts of personal failure, poor concentration, low self-confidence, slow or fast speech, and suicidal ideation. From the maximum score of 27 points, a cut-off value ≥ 10 was used to indicate the presence of clinically significant depressive symptoms [18].
- Generalized Anxiety Disorder Questionnaire-7 Scale is a validated questionnaire that measures the severity of anxiety. Seven questions refer to feeling nervous, on edge, unable to control worrying, being worried about different things, inability to relaxbeing very restless that it is hard to sit, getting irritated easily, and feeling afraid that something horrible might happen. A total score ranges from 0 to 21, and the cut-off point for moderate anxiety symptoms is over 10 [19].
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Garbarino, S.; Bardwell, A.; Guglielmi, O.; Chiorri, C.; Bonanni, E.; Magnavita, N. Association of Anxiety and Depression in Obstructive Sleep Apnea Patients: A Systematic Review and Meta-Analysis. Behav. Sleep Med. 2018, 18, 35–37. [Google Scholar] [CrossRef] [PubMed]
- Carneiro-Barrera, A.; Amaro-Gahete, F.J.; Sáez-Roca, G.; Martín-Carrasco, C.; Ruiz, J.R.; Buela-Casal, G. Anxiety and Depression in Patients with Obstructive Sleep Apnoea before and after Continuous Positive Airway Pressure: The ADIPOSA Study. J. Clin. Med. 2019, 8, 2099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aftab, Z.; Anthony, A.T.; Rahmat, S.; Sangle, P.; Khan, S. An Updated Review on the Relationship of Depressive Symptoms in Obstructive Sleep Apnea and Continuous Positive Airway Pressure. Cureus 2021, 13, e15907. [Google Scholar] [CrossRef]
- Heinzer, R.; Vat, S.; Marques-Vidal, P.; Marti-Soler, H.; Andries, D.; Tobback, N.; Haba-Rubio, J. Prevalence of sleep-disordered breathing in the general population: The HypnoLaus study. Lancet Respir. Med. 2015, 3, 310–318. [Google Scholar] [CrossRef] [Green Version]
- Marrone, O.; Bonsignore, M.R. Blood-pressure variability in patients with obstructive sleep apnea: Current perspectives. Nat. Sci. Sleep 2018, 10, 229–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitra, A.K.; Bhuiyan, A.R.; Jones, E.A. Association and Risk Factors for Obstructive Sleep Apnea and Cardiovascular Diseases: A Systematic Review. Diseases 2021, 9, 88. [Google Scholar] [CrossRef] [PubMed]
- Le Grande, M.R.; Beauchamp, A.; Driscoll, A.; Jackson, A.C. Prevalence of obstructive sleep apnoea in acute coronary syndrome patients: Systematic review and meta-analysis. BMC Cardiovasc. Disord. 2020, 20, 147. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Hou, W.S.; Zhang, X.W.; Tang, Z.Y. Obstructive sleep apnea and risk of stroke: A meta-analysis of prospective studies. Int. J. Cardiol. 2014, 172, 466–469. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Wan, Y.; Xu, M.; Ming, J.; Xing, Y.; An, F.; Ji, Q. The association between obstructive sleep apnea and metabolic syndrome: A systematic review and meta-analysis. BMC Pulm. Med. 2015, 15, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Tan, J.; Miao, Y.; Zhang, Q. Obstructive sleep apnea, prediabetes and progression of type 2 diabetes: A systematic review and meta-analysis. J. Diabetes Investig. 2022, 13, 1396–1411. [Google Scholar] [CrossRef]
- Kamphuis, J.; Meerlo, P.; Koolhaas, J.M.; Lancel, M. Poor sleep as a potential causal factor in aggression and violence. Sleep Med. 2012, 13, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Lehto, S.M.; Sahlman, J.; Soini, E.J.; Gylling, H.; Vanninen, E.; Seppä, J.; Viinamäki, H.; Tuomilehto, H. The association between anxiety and the degree of illness in mild obstructive sleep apnoea. Clin. Respir. J. 2012, 7, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Lundetræ, R.S.; Saxvig, I.W.; Lehmann, S. Effect of continuous positive airway pressure on symptoms of anxiety and depression in patients with obstructive sleep apnea. Sleep Breath. 2021, 25, 1277–1283. [Google Scholar] [CrossRef] [PubMed]
- Walker, A.; Naughton, M.T.; Shaw, L.; Jeklin, A.T.; Martin, C.; Dabscheck, E. Depression scores improve with continuous positive airway pressure in specialized sleep clinics: Real-world data. J. Clin. Sleep Med. 2021, 17, 1201–1209. [Google Scholar] [CrossRef] [PubMed]
- El-Sherbini, A.M.; Bediwy, A.S.; El-Mitwalli, A. Association between obstructive sleep apnea (OSA) and depression and the effect of continuous positive airway pressure (CPAP) treatment. Neuropsychiatr Dis. Treat. 2011, 7, 715–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johns, M.W. A new method for measuring daytime sleepiness: The epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L. The PHQ-9: A new depression diagnostic and severity measure. Psychiatr. Ann. 2002, 32, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Edwards, C.; Mukherjee, S.; Simpson, L.; Palmer, L.J.; Almeida, O.P.; Hillman, D.R. Depressive symptoms before and after treatment of obstructive sleep apnea in men and women. J. Clin. Sleep Med. 2015, 11, 1029–1038. [Google Scholar] [CrossRef] [PubMed]
- McCall, W.V.; Harding, D.; O’Donovan, C. Correlates of depressive symptoms in patients with obstructive sleep apnea. J. Clin. Sleep Med. 2006, 2, 424–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawahara, S.; Akashiba, T.; Akahoshit, T.; Horie, T. Nasal CPAP improves the quality of life and lessens the depressive symptoms in patients with obstructive sleep apnea syndrome. Intern. Med. 2005, 44, 422–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenberg, R.; Doghramji, P. Optimal treatment of obstructive sleep apnea and excessive sleepiness. Adv. Ther. 2009, 26, 295–312. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Cheng, Y.; Li, Y.; Han, J.; Yuan, Z.; Li, Q.; Zhong, F.; Wu, Y.; Fan, X.; Bo, T.; et al. The Relationship Between Obesity and Depression Is Partly Dependent on Metabolic Health Status: A Nationwide Inpatient Sample Database Study. Front. Endocrinol. 2022, 13, 880230. [Google Scholar] [CrossRef] [PubMed]
- Karamanl, H.; Kayhan, F.; Akgedik, R. Depressive Symptoms in Patients with Obstructive Sleep Apnea. Turk. Thorac. J. 2016, 17, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.A.; Han, S.H.; Ryu, H.U. Anxiety and its relationship to quality of life independent of depression in patients with obstructive sleep apnea. J. Psychosom. Res. 2015, 79, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Povitz, M.; Bolo, C.E.; Heitman, S.J.; Tsai, W.H.; Wang, J.; James, M.T. Effect of treatment of obstructive sleep apnea on depressive symptoms: Systematic review and meta-analysis. PLoS Med. 2014, 11, e1001762. [Google Scholar] [CrossRef] [Green Version]
- Aro, M.M.; Anttalainen, U.; Polo, O.; Saaresranta, T. Mood, sleepiness, and weight gain after three years on CPAP therapy for sleep apnoea. Eur. Clin. Respir. J. 2021, 8, 1888394. [Google Scholar] [CrossRef]
- Chou, M.S.H.; Ting, N.C.H.; El-Turk, N.; Harrington, Z.; Dobler, C.C. Treatment burden experienced by patients with obstructive sleep apnoea using continuous positive airway pressure therapy. PLoS ONE 2021, 16, e0252915. [Google Scholar] [CrossRef]
- Bock, J.M.; Needham, K.A.; Gregory, D.A.; Ekono, M.M.; Wickwire, E.M.; Somers, V.K.; Lerman, A. Continuous Positive Airway Pressure Adherence and Treatment Cost in Patients With Obstructive Sleep Apnea and Cardiovascular Disease. Mayo Clin. Proc. Innov. Qual. Outcomes 2022, 6, 166–175. [Google Scholar] [CrossRef]
- Sweetman, A.; Lack, L.; McEvoy, R.D. Effect of depression, anxiety, and stress symptoms on response to cognitive behavioral therapy for insomnia in patients with comorbid insomnia and sleep apnea: A randomized controlled trial. J. Clin. Sleep Med. 2021, 17, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, A.; Routray, D.; Swain, S.; Das, A.K. Prevalence and risk factors of people at-risk of obstructive sleep apnea in a rural community of Odisha, India: A community based cross-sectional study. Sleep Med. 2019, 58, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Hsu, W.Y.; Chiu, N.Y.; Chang, C.C.; Chang, T.G.; Lane, H.Y. The association between cigarette smoking and obstructive sleep apnea. Tob. Induc. Dis. 2019, 17, 27. [Google Scholar] [CrossRef] [PubMed]
- Simpson, L.; McArdle, N.; Eastwood, P.R.; Ward, K.L.; Cooper, M.N.; Wilson, A.C.; Hillman, D.R.; Palmer, L.J.; Mukherjee, S. Physical inactivity is associated with moderate-severe obstructive sleep apnea. J. Clin. Sleep Med. 2015, 11, 1091–1099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reid, M.; Maras, J.E.; Shea, S.; Wood, A.C.; Castro-Diehl, C.; Johnson, D.A.; Huang, T.; Jacobs, D.R., Jr.; Crawford, A.; St-Onge, M.P.; et al. Association between diet quality and sleep apnea in the Multi-Ethnic Study of Atherosclerosis. Sleep 2019, 42, zsy194. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total (n = 99) | Male (n = 66) | Female (n = 33) | p-Value | |
|---|---|---|---|---|
| Age | 56 (48, 65) | 55 (44, 63) | 62 (54, 68) | <0.001 |
| BMI | 36 (31, 40) | 36 (31, 40) | 37 (34, 41) | 0.24 |
| Neck (cm) | 44.0 (41.0, 47.0) | 44.5 (41.2, 47.8) | 43.0 (40.0, 46.0) | 0.041 |
| Abdomen (cm) | 127 (112, 136) | 130 (114, 136) | 122 (109, 134) | 0.14 |
| AHI | 54 (37, 76) | 54 (35, 77) | 54 (39, 73) | 0.92 |
| ODI | 54 (30, 71) | 55 (29, 73) | 52 (33, 58) | 0.64 |
| [t90] | 21 (4, 46) | 22 (4, 56) | 20 (4, 39) | 0.68 |
| ESS | 12.0 (9.0, 16.5) | 8.0 (3.2, 10.0) | 6.0 (4.0, 8.0) | 0.48 |
| PHQ-9 score | 10.0 (7.0, 13.0) | 9.5 (7.0, 12.0) | 12.0 (10.0, 15.0) | <0.001 |
| PHQ-9 ≥10 n (%) | 48 (48.48) | 39 (39.39) | 12 (12.12) | 0.033 |
| GAD-7 score | 7.0 (4.0, 11.0) | 7.0 (3.0, 10.0) | 7.0 (5.0, 12.0) | 0.25 |
| GAD-7 ≥10 n (%) | 27 (27.22) | 16 (16.16) | 11 (11.11) | 0.343 |
| Total (n= 99) | Men (n = 66) | Women (n = 33) | p-Value | |
|---|---|---|---|---|
| Baseline | ||||
| PHQ-9 score <10 | 51.0 (51.5%) | 39.0 (59.1%) | 12.0 (36.4%) | 0.033 1 |
| PHQ-9 score ≥ 10 | 48.0 (48.5%) | 27.0 (40.9%) | 21.0 (63.6%) | |
| GAD-7 score < 10 | 72.0 (72.7%) | 50.0 (75.8 %) | 22.0 (66.7%) | 0.338 1 |
| GAD-7 score ≥ 10 | 27.0 (27.3%) | 16.0 (24.2%) | 11.0 (33.3%) | |
| After 6 months | <0.001 1 | |||
| PHQ-9 score < 10 | 87.0 (87.9%) | 63.0 (95.5%) | 24.0 (72.7%) | |
| PHQ-9 score ≥ 10 | 12.0 (12.1%) | 3.0 (4.5%) | 9.0 (27.3%) | |
| GAD-7 score < 10 | 88.0 (89.9%) | 60.0 (90.9%) | 28.0 (84.8%) | 0.366 1 |
| GAD-7 score ≥ 10 | 11.0 (11.1%) | 6.0 (9.1%) | 5.0 (15.2%) | |
| After 1 year | 0.027 1 | |||
| PHQ-9 score < 10 | 92.0 (92.9%) | 64.0 (97.0%) | 28.0 (84.8%) | |
| PHQ-9 score ≥ 10 | 7.0 (7.1%) | 2.0 (3.0%) | 5.0 (15.2%) | |
| GAD-7 score < 10 | 97.0 (98.0%) | 65.0 (98.5%) | 32.0 (97.0%) | 0.631 1 |
| GAD-7 score ≥ 10 | 2.0 (2.0%) | 1.0 (1.5%) | 1.0 (3.0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velescu, D.R.; Marc, M.; Manolescu, D.; Trăilă, D.; Oancea, C. CPAP Therapy on Depressive and Anxiety Symptoms in Patients with Moderate to Severe Obstructive Sleep Apnea Syndrome. Medicina 2022, 58, 1402. https://doi.org/10.3390/medicina58101402
Velescu DR, Marc M, Manolescu D, Trăilă D, Oancea C. CPAP Therapy on Depressive and Anxiety Symptoms in Patients with Moderate to Severe Obstructive Sleep Apnea Syndrome. Medicina. 2022; 58(10):1402. https://doi.org/10.3390/medicina58101402
Chicago/Turabian StyleVelescu, Diana Raluca, Monica Marc, Diana Manolescu, Daniel Trăilă, and Cristian Oancea. 2022. "CPAP Therapy on Depressive and Anxiety Symptoms in Patients with Moderate to Severe Obstructive Sleep Apnea Syndrome" Medicina 58, no. 10: 1402. https://doi.org/10.3390/medicina58101402