
The Usefulness of Lymphadenectomy in Bladder Cancer—Current Status

 , ,
, , {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Imaging and Molecular Diagnosis of Nodal Metastases
3. Lymphadenectomy in Bladder Cancer
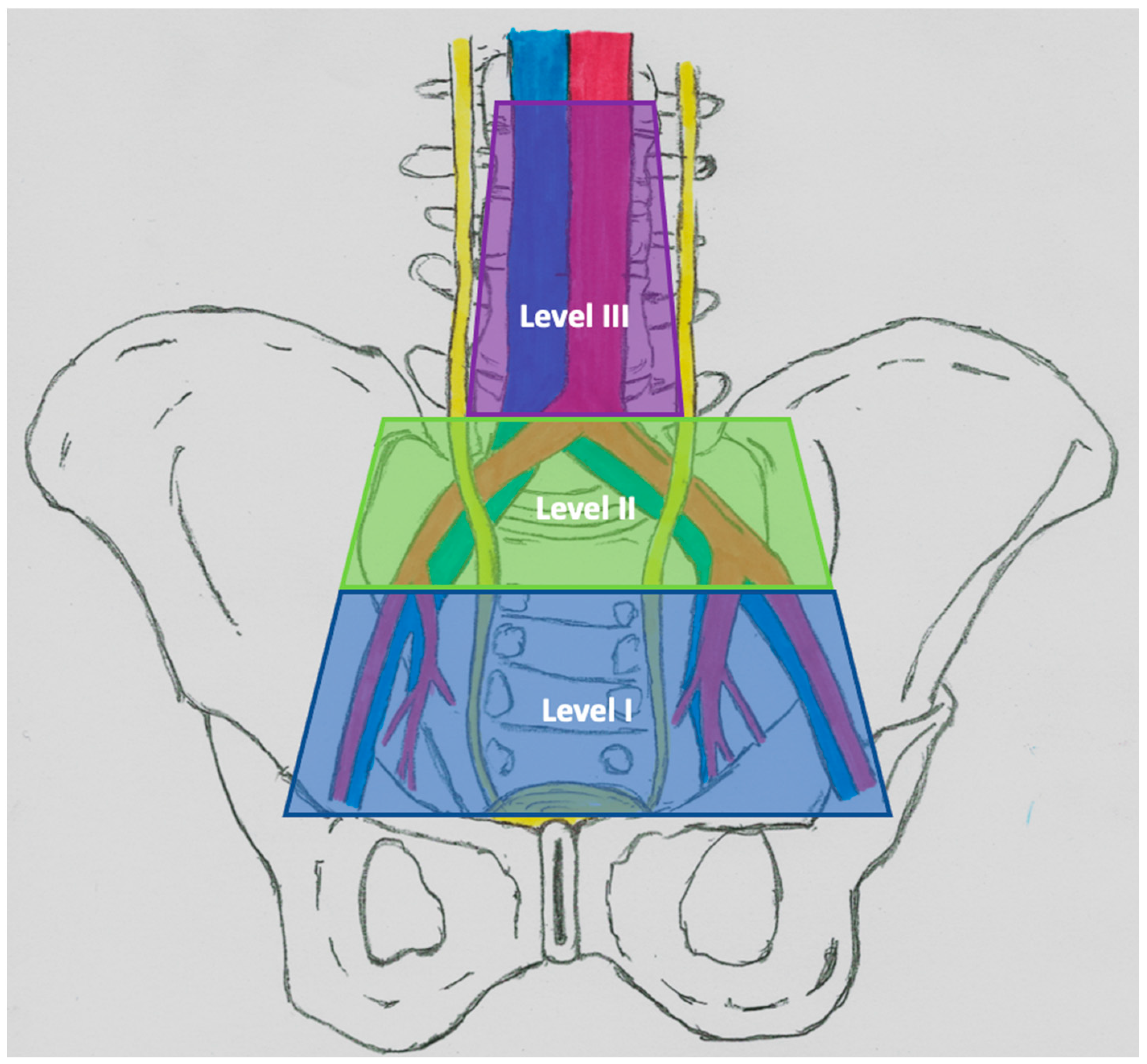
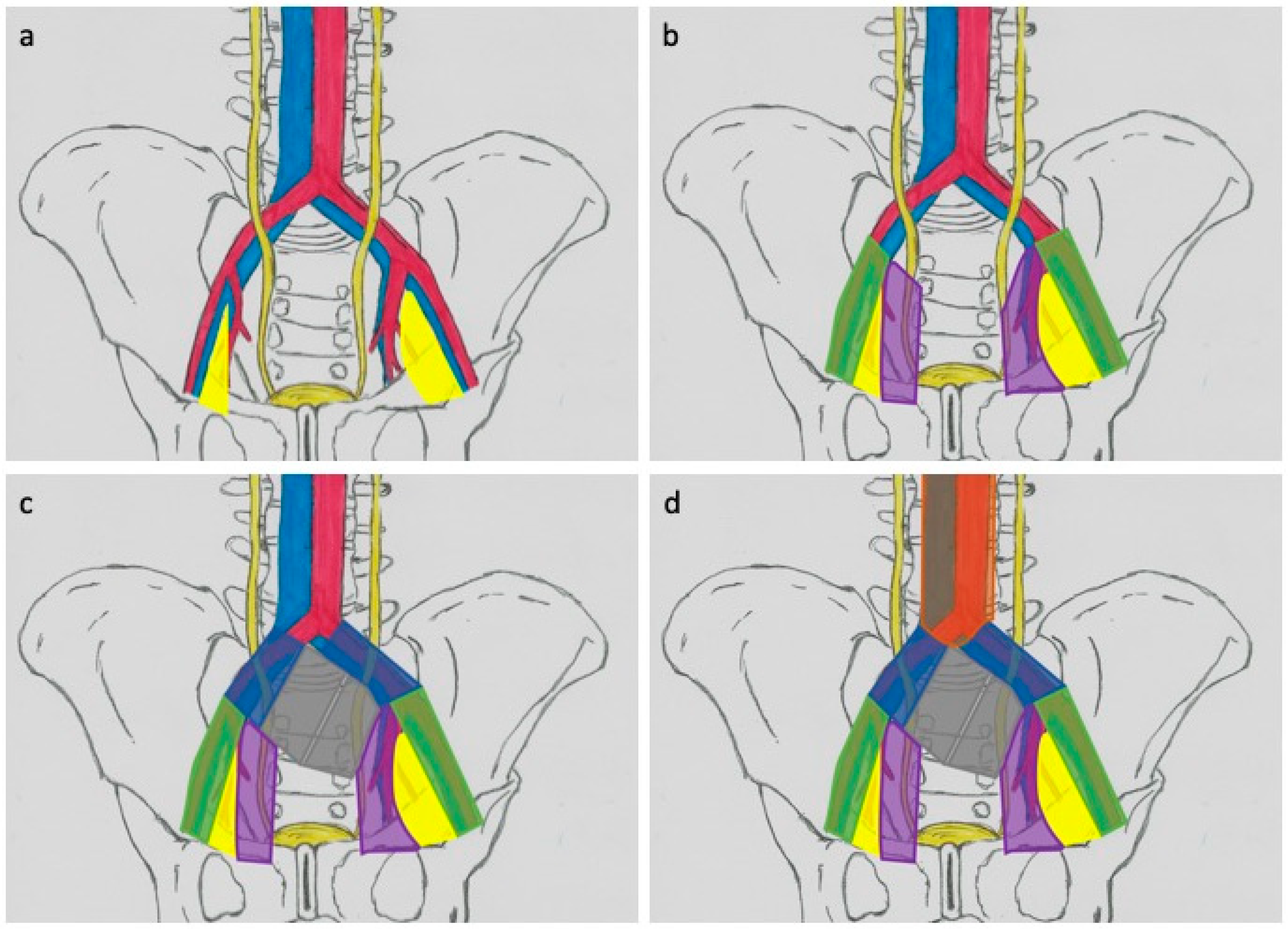
3.1. Lymphadectomy Template—Anatomical Considerations
3.2. Anatomical Boundaries and Oncological Results
3.3. Prognostic Interpretation of N+
4. Complications of Lymphadenectomy
5. Current Guidelines
6. Minimally Invasive Surgery and Lymphadenectomy
7. Future Perspectives
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hautmann, R.E.; de Petriconi, R.C.; Pfeiffer, C.; Volkmer, B.G. Radical Cystectomy for Urothelial Carcinoma of the Bladder Without Neoadjuvant or Adjuvant Therapy: Long-Term Results in 1100 Patients. Eur. Urol. 2012, 61, 1039–1047. [Google Scholar] [CrossRef]
- Rajesh, A.; Sokhi, H.; Fung, R.; Mulcahy, K.A.; Bankart, M.J. Role of Whole-Body Staging Computed Tomographic Scans for Detecting Distant Metastases in Patients With Bladder Cancer. J. Comput. Assist. Tomogr. 2011, 35, 402–405. [Google Scholar] [CrossRef] [PubMed]
- ACR Appropriateness Criteria: Pretreatment Staging of Muscle-Invasive Bladder Cancer. American College of Radiology. 2017. Available online: https://acsearch.acr.org/docs/69370/Narrative/ (accessed on 24 February 2021).
- Shankar, P.R.; Barkmeier, D.; Hadjiiski, L.; Cohan, R.H. A pictorial review of bladder cancer nodal metastases. Transl. Androl. Urol. 2018, 7, 804–813. [Google Scholar] [CrossRef] [PubMed]
- MacVicar, A. Bladder cancer staging. BJU Int. 2002, 86, 111–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMahon, C.J.; Rofsky, N.M.; Pedrosa, I. Lymphatic Metastases from Pelvic Tumors: Anatomic Classification, Characterization, and Staging. Radiology 2010, 254, 31–46. [Google Scholar] [CrossRef] [PubMed]
- Witjes, J.A.; Lebret, T.; Compérat, E.M.; Cowan, N.C.; De Santis, M.; Bruins, H.M.; Hernández, V.; Espinós, E.L.; Dunn, J.; Rouanne, M.; et al. Updated 2016 EAU Guidelines on Muscle-invasive and Metastatic Bladder Cancer. Eur. Urol. 2017, 71, 462–475. [Google Scholar] [CrossRef]
- Lam, T.B.L. Optimizing the diagnosis of pelvic lymph node metastasis in bladder cancer using computed tomography and magnetic resonance imaging. Cancer Commun. 2018, 38, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, W.T.; Lam, W.W.M.; Yu, M.Y.; Cheung, T.H.; Metreweli, C. Comparison of Dynamic Helical CT and Dynamic MR Imaging in the Evaluation of Pelvic Lymph Nodes in Cervical Carcinoma. Am. J. Roentgenol. 2000, 175, 759–766. [Google Scholar] [CrossRef]
- Baltaci, S.; Resorlu, B.; Yagcı, C.; Turkolmez, K.; Gogus, C.; Beduk, Y. Computerized Tomography for Detecting Perivesical Infiltration and Lymph Node Metastasis in Invasive Bladder Carcinoma. Urol. Int. 2008, 81, 399–402. [Google Scholar] [CrossRef]
- Tritschler, S.; Mosler, C.; Straub, J.; Buchner, A.; Karl, A.; Graser, A.; Stief, C.; Tilki, D. Staging of muscle-invasive bladder cancer: Can computerized tomography help us to decide on local treatment? World J. Urol. 2012, 30, 827–831. [Google Scholar] [CrossRef]
- Horn, T.; Zahel, T.; Adt, N.; Schmid, S.C.; Heck, M.M.; Thalgott, M.K.; Hatzichristodoulou, G.; Haller, B.; Autenrieth, M.; Kübler, H.R.; et al. Evaluation of Computed Tomography for Lymph Node Staging in Bladder Cancer Prior to Radical Cystectomy. Urol. Int. 2016, 96, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Vikram, R.; Sandler, C.M.; Ng, C.S. Imaging and Staging of Transitional Cell Carcinoma: Part 1, Lower Urinary Tract. Am. J. Roentgenol. 2009, 192, 1481–1487. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Rajesh, A.; Prasad, S.R.; Gaitonde, K.; Lall, C.G.; Mouraviev, V.; Aeron, G.; Bracken, R.B.; Sandrasegaran, K. Urinary Bladder Cancer: Role of MR Imaging. Radiographics 2012, 32, 371–387. [Google Scholar] [CrossRef]
- Salminen, A.P.; Jambor, I.; Syvanen, K.T.; Bostrom, P.J. Update on novel imaging techniques for the detection of lymph node me-tastases in bladder cancer. Minerva Urol. Nefrol. 2016, 68, 138–149. [Google Scholar]
- Woo, S.; Suh, C.H.; Kim, S.Y.; Cho, J.Y.; Kim, S.H. The Diagnostic Performance of MRI for Detection of Lymph Node Metastasis in Bladder and Prostate Cancer: An Updated Systematic Review and Diagnostic Meta-Analysis. Am. J. Roentgenol. 2018, 210, W95–W109. [Google Scholar] [CrossRef]
- Weissleder, R.; Elizondo, G.; Wittenberg, J.; Rabito, C.A.; Bengele, H.H.; Josephson, L. Ultrasmall superparamagnetic iron oxide: Characterization of a new class of contrast agents for MR imaging. Radiology 1990, 175, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Harisinghani, M.G.; Saini, S.; Weissleder, R.; Hahn, P.F.; Yantiss, R.K.; Tempany, C.; Wood, B.J.; Mueller, P.R. MR lymphangiography using ultrasmall superparamagnetic iron oxide in patients with primary abdominal and pelvic malignancies: Radiographic-pathologic correlation. Am. J. Roentgenol. 1999, 172, 1347–1351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Haas, R.J.; Steyvers, M.J.; Fütterer, J.J. Multiparametric MRI of the Bladder: Ready for Clinical Routine? Am. J. Roentgenol. 2014, 202, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- Birkhäuser, F.D.; Studer, U.E.; Froehlich, J.M.; Triantafyllou, M.; Bains, L.J.; Petralia, G.; Vermathen, P.; Fleischmann, A.; Thoeny, H.C. Combined Ultrasmall Superparamagnetic Particles of Iron Oxide–Enhanced and Diffusion-weighted Magnetic Resonance Imaging Facilitates Detection of Metastases in Normal-sized Pelvic Lymph Nodes of Patients with Bladder and Prostate Cancer. Eur. Urol. 2013, 64, 953–960. [Google Scholar] [CrossRef] [PubMed]
- Maurer, T.; Souvatzoglou, M.; Kübler, H.; Opercan, K.; Schmidt, S.; Herrmann, K.; Stollfuss, J.; Weirich, G.; Haller, B.; Gschwend, J.E.; et al. Diagnostic Efficacy of [11C]Choline Positron Emission Tomography/Computed Tomography Compared With Conventional Computed Tomography in Lymph Node Staging of Patients With Bladder Cancer Prior to Radical Cystectomy. Eur. Urol. 2012, 61, 1031–1038. [Google Scholar] [CrossRef]
- Jeong, I.G.; Hong, S.; You, D.; Hong, J.H.; Ahn, H.; Kim, C.-S. FDG PET–CT for Lymph Node Staging of Bladder Cancer: A Prospective Study of Patients with Extended Pelvic Lymphadenectomy. Ann. Surg. Oncol. 2015, 22, 3150–3156. [Google Scholar] [CrossRef] [PubMed]
- Goodfellow, H.; Viney, Z.; Hughes, P.; Rankin, S.; Rottenberg, G.; Hughes, S.; Evison, F.; Dasgupta, P.; O’Brien, T.; Khan, M.S. Role of fluorodeoxyglucose positron emission tomography (FDG PET)-computed tomography (CT) in the staging of bladder cancer. BJU Int. 2014, 114, 389–395. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.-J.; Koo, P.J.; Pak, K.; Kim, I.-J.; Kim, K. Diagnostic accuracy of C-11 choline and C-11 acetate for lymph node staging in patients with bladder cancer: A systematic review and meta-analysis. World J. Urol. 2018, 36, 331–340. [Google Scholar] [CrossRef]
- Mitra, A.P.; Almal, A.A.; George, B.; Fry, D.W.; Lenehan, P.F.; Pagliarulo, V.; Cote, R.J.; Datar, R.H.; Worzel, W.P. The use of genetic programming in the analysis of quantitative gene expression profiles for identification of nodal status in bladder cancer. BMC Cancer 2006, 6, 159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nezos, A.; Pissimisis, N.; Lembessis, P.; Sourla, A.; Dimopoulos, P.; Dimopoulos, T.; Tzelepis, K.; Koutsilieris, M. Detection of circulating tumor cells in bladder cancer patients. Cancer Treat. Rev. 2009, 35, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Naoe, M.; Ogawa, Y.; Morita, J.; Omori, K.; Takeshita, K.; Shichijyo, T.; Okumura, T.; Igarashi, A.; Yanaihara, A.; Iwamoto, S.; et al. Detection of circulating urothelial cancer cells in the blood using the CellSearch System. Cancer 2007, 109, 1439–1445. [Google Scholar] [CrossRef] [PubMed]
- Msaouel, P.; Koutsilieris, M. Diagnostic value of circulating tumor cell detection in bladder and urothelial cancer: Systematic review and meta-analysis. BMC Cancer 2011, 11, 336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hegele, A.; Mecklenburg, V.; Varga, Z.; Olbert, P.; Hofmann, R.; Barth, P. CA19.9 and CEA in transitional cell carcinoma of the bladder: Serological and immunohistochemical findings. Anticancer. Res. 2010, 30, 5195–5200. [Google Scholar] [PubMed]
- Szarvas, T.; Becker, M.; Dorp, F.V.; Gethmann, C.; Tötsch, M.; Bánkfalvi, Á.; Schmid, K.W.; Romics, I.; Rübben, H.; Ergün, S. Matrix metalloproteinase-7 as a marker of metastasis and predictor of poor survival in bladder cancer. Cancer Sci. 2010, 101, 1300–1308. [Google Scholar] [CrossRef]
- Kamat, A.M.; Hegarty, P.K.; Gee, J.R.; Clark, P.E.; Svatek, R.S.; Hegarty, N.; Shariat, S.F.; Xylinas, E.; Schmitz-Dräger, B.J.; Lotan, Y.; et al. ICUD-EAU International Consultation on Bladder Cancer 2012: Screening, Diagnosis, and Molecular Markers. Eur. Urol. 2013, 63, 4–15. [Google Scholar] [CrossRef]
- Colston, J.; Leadbetter, W. Infiltrating Carcinoma of the Bladder. J. Urol. 1936, 36, 669–683. [Google Scholar] [CrossRef]
- Jewett, H.J.; Strong, G.H. Infiltrating Carcinoma of the Bladder: Relation of Depth of Penetration of the Bladder Wall to Incidence of Local Extension and Metastases. J. Urol. 1946, 55, 366–372. [Google Scholar] [CrossRef]
- Hurle, R.; Naspro, R. Pelvic lymphadenectomy during radical cystectomy: A review of the literature. Surg. Oncol. 2010, 19, 208–220. [Google Scholar] [CrossRef] [PubMed]
- Skinner, D.G. Management of Invasive Bladder Cancer: A Meticulous Pelvic Node Dissection Can Make a Difference. J. Urol. 1982, 128, 34–36. [Google Scholar] [CrossRef]
- Abdollah, F.; Sun, M.; Schmitges, J.; Djahangirian, O.; Tian, Z.; Jeldres, C.; Perrotte, P.; Shariat, S.F.; Montorsi, F.; Karakiewicz, P.I. Stage-specific impact of pelvic lymph node dissection on survival in patients with non-metastatic bladder cancer treated with radical cystectomy. BJU Int. 2012, 109, 1147–1154. [Google Scholar] [CrossRef]
- Leadbetter, W.; Cooper, J.F. Regional Gland Dissection for Carcinoma of The Bladder: A Technique for One-stage Cystectomy, Glanddissection, and Bilateral Uretero-enterostomy. J. Urol. 1950, 63, 242–260. [Google Scholar] [CrossRef]
- Inoue, S.; Shiina, H.; Mitsui, Y.; Yasumoto, H.; Matsubara, A.; Igawa, M. Identification of lymphatic pathway involved in the spread of bladder cancer: Evidence obtained from fluorescence navigation with intraoperatively injected indocyanine green. Can. Urol. Assoc. J. 2013, 7, E322. [Google Scholar] [CrossRef] [Green Version]
- Hsu, M.C.; Itkin, M. Lymphatic Anatomy. Tech. Vasc. Interv. Radiol. 2016, 19, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Vazina, A.; Dugi, D.; Shariat, S.F.; Evans, J.; Link, R.; Lerner, S.P. Stage Specific Lymph Node Metastasis Mapping in Radical Cystectomy Specimens. J. Urol. 2004, 171, 1830–1834. [Google Scholar] [CrossRef]
- Bi, L.; Huang, H.; Fan, X.; Li, K.; Xu, K.; Jiang, C.; Liu, H.; Dong, W.; Zhang, S.; Yang, X.; et al. Extended vs non-extended pelvic lymph node dissection and their influence on recurrence-free survival in patients undergoing radical cystectomy for bladder cancer: A systematic review and meta-analysis of comparative studies. BJU Int. 2014, 113, E39–E48. [Google Scholar] [CrossRef] [Green Version]
- Leissner, J.; Ghoneim, M.; Abol-Enein, H.; Thüroff, J.; Franzaring, L.; Fisch, M.; Schulze, H.; Managadze, G.; Allhoff, E.; El-Baz, M.; et al. Extended Radical Lymphadenectomy in Patients With Urothelial Bladder Cancer:: Results of a Prospective Multicenter Study. J. Urol. 2004, 171, 139–144. [Google Scholar] [CrossRef]
- Weisbach, L.; Dahlem, R.; Simone, G.; Hansen, J.; Soave, A.; Engel, O.; Chun, F.K.; Shariat, S.F.; Fisch, M.; Rink, M. Lymph node dissection during radical cystectomy for bladder cancer treatment: Considerations on relevance and extent. Int. Urol. Nephrol. 2013, 45, 1561–1567. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.B.; Ulhøi, B.P.; Jensen, K.M.-E. Extended versus limited lymph node dissection in radical cystectomy: Impact on recurrence pattern and survival. Int. J. Urol. 2012, 19, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Dorin, R.P.; Daneshmand, S.; Eisenberg, M.S.; Chandrasoma, S.; Cai, J.; Miranda, G.; Nichols, P.W.; Skinner, D.G.; Skinner, E.C. Lymph Node Dissection Technique Is More Important Than Lymph Node Count in Identifying Nodal Metastases in Radical Cystectomy Patients: A Comparative Mapping Study. Eur. Urol. 2011, 60, 946–952. [Google Scholar] [CrossRef]
- Abol-Enein, H.; El-Baz, M.; El-Hameed, M.A.A.; Abdel-Latif, M.; Ghoneim, M.A. Lymph Node Involvement in Patients with Bladder Cancer Treated With Radical Cystectomy: A Patho-Anatomical Study—A Single Center Experience. J. Urol. 2004, 172, 1818–1821. [Google Scholar] [CrossRef] [PubMed]
- Roth, B.; Zehnder, P.; Birkhäuser, F.D.; Burkhard, F.C.; Thalmann, G.N.; Studer, U.E. Is Bilateral Extended Pelvic Lymphadenectomy Necessary for Strictly Unilateral Invasive Bladder Cancer? J. Urol. 2012, 187, 1577–1582. [Google Scholar] [CrossRef]
- Seiler, R.; Von Gunten, M.; Thalmann, G.N.; Fleischmann, A. Pelvic lymph nodes: Distribution and nodal tumour burden of urothelial bladder cancer. J. Clin. Pathol. 2010, 63, 504–507. [Google Scholar] [CrossRef] [Green Version]
- Ghoneim, M.A.; Abol-Enein, H. Lymphadenectomy with Cystectomy: Is It Necessary and What Is Its Extent? Eur. Urol. 2004, 46, 457–461. [Google Scholar] [CrossRef]
- Pedrosa, J.A.; Koch, M.O.; Cheng, L. Lymph node-positive bladder cancer: Surgical, pathologic, molecular and prognostic aspects. Expert Rev. Anticancer. Ther. 2013, 13, 1281–1295. [Google Scholar] [CrossRef]
- Herr, H.; Lee, C.; Chang, S.; Lerner, S.; Bladder Cancer Collaborative Group. Standardization of Radical Cystectomy and Pelvic Lymph Node Dissection for Bladder Cancer: A Collaborative Group Report. J. Urol. 2004, 171, 1823–1828. [Google Scholar] [CrossRef]
- Simone, G.; Papalia, R.; Ferriero, M.; Guaglianone, S.; Castelli, E.; Collura, D.; Muto, G.; Gallucci, M. Stage-specific impact of extended versus standard pelvic lymph node dissection in radical cystectomy. Int. J. Urol. 2013, 20, 390–397. [Google Scholar] [CrossRef]
- Bruins, H.M.; Huang, G.J.; Cai, J.; Skinner, D.G.; Stein, J.P.; Penson, D.F. Clinical Outcomes and Recurrence Predictors of Lymph Node Positive Urothelial Cancer After Cystectomy. J. Urol. 2009, 182, 2182–2187. [Google Scholar] [CrossRef]
- Vieweg, J.; Gschwend, J.E.; Herr, H.W.; Fair, W.R. The impact of primary stage on survival in patients with lymph node positive bladder cancer. J. Urol. 1999, 161, 72–76. [Google Scholar] [CrossRef]
- Karl, A.; Carroll, P.R.; Gschwend, J.E.; Knüchel, R.; Montorsi, F.; Stief, C.G.; Studer, U.E. The Impact of Lymphadenectomy and Lymph Node Metastasis on the Outcomes of Radical Cystectomy for Bladder Cancer. Eur. Urol. 2009, 55, 826–835. [Google Scholar] [CrossRef] [PubMed]
- Konety, B.R.; Joslyn, S.A.; O’Donnell, M.A. Extent of Pelvic Lymphadenectomy and Its Impact On Outcome in Patients Diagnosed With Bladder Cancer: Analysis of Data From the Surveillance, Epidemiology and End Results Program Data Base. J. Urol. 2003, 169, 946–950. [Google Scholar] [CrossRef] [PubMed]
- Herr, H.W. Superiority of Ratio Based Lymph Node Staging for Bladder Cancer. J. Urol. 2003, 169, 943–945. [Google Scholar] [CrossRef]
- Stein, J.P.; Cai, J.; Groshen, S.; Skinner, D.G. Risk Factors for Patients With Pelvic Lymph Node Metastases Following Radical Cystectomy With En Bloc Pelvic Lymphadenectomy: The Concept of Lymph Node Density. J. Urol. 2003, 170, 35–41. [Google Scholar] [CrossRef]
- Larcher, A.; Sun, M.; Schiffmann, J.; Tian, Z.; Shariat, S.; McCormack, M.; Saad, F.; Fossati, N.; Abdollah, F.; Briganti, A.; et al. Differential effect on survival of pelvic lymph node dissection at radical cystectomy for muscle invasive bladder cancer. Eur. J. Surg. Oncol. 2015, 41, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Bruins, H.M.; Veskimae, E.; Hernandez, V.; Imamura, M.; Neuberger, M.M.; Dahm, P.; Stewart, F.; Lam, T.B.; N’Dow, J.; van der Heijden, A.G.; et al. The Impact of the Extent of Lymphadenectomy on Oncologic Outcomes in Patients Undergoing Radical Cystectomy for Bladder Cancer: A Systematic Review. Eur. Urol. 2014, 66, 1065–1077. [Google Scholar] [CrossRef] [Green Version]
- Brossner, C.; Pycha, A.; Toth, A.; Mian, C.; Kuber, W. Does extended lymphadenectomy increase the morbidity of radical cystectomy? BJU Int. 2004, 93, 64–66. [Google Scholar] [CrossRef] [Green Version]
- May, M.; Herrmann, E.; Bolenz, C.; Brookman-May, S.; Tiemann, A.; Moritz, R.; Fritsche, H.-M.; Burger, M.; Trojan, L.; Michel, M.S.; et al. Association Between the Number of Dissected Lymph Nodes During Pelvic Lymphadenectomy and Cancer-Specific Survival in Patients with Lymph Node–Negative Urothelial Carcinoma of the Bladder Undergoing Radical Cystectomy. Ann. Surg. Oncol. 2011, 18, 2018–2025. [Google Scholar] [CrossRef] [PubMed]
- Sharir, S.; Fleshner, N.E. Lymph node assessment and lymphadenectomy in bladder cancer. J. Surg. Oncol. 2009, 99, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Buscarini, M.; Josephson, D.Y.; Stein, J.P. Lymphadenectomy in Bladder Cancer: A Review. Urol. Int. 2007, 79, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Knap, M.; Lundbeck, F.; Overgaard, J. The role of pelvic lymph node dissection as a predictive and prognostic factor in bladder cancer. Eur. J. Cancer 2003, 39, 604–613. [Google Scholar] [CrossRef]
- Dangle, P.P.; Gong, M.C.; Bahnson, R.R.; Pohar, K.S. How Do Commonly Performed Lymphadenectomy Templates Influence Bladder Cancer Nodal Stage? J. Urol. 2010, 183, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Miocinovic, R.; Gong, M.C.; Ghoneim, I.A.; Fergany, A.F.; Hansel, D.E.; Stephenson, A.J. Presacral and Retroperitoneal Lymph Node Involvement in Urothelial Bladder Cancer: Results of a Prospective Mapping Study. J. Urol. 2011, 186, 1269–1273. [Google Scholar] [CrossRef]
- Moschini, M.; Arbelaez, E.; Cornelius, J.; Mattei, A.; Shariat, S.F.; Dell′oglio, P.; Zaffuto, E.; Salonia, A.; Montorsi, F.; Briganti, A.; et al. Pattern of node metastases in patients treated with radical cystectomy and extended or superextended pelvic lymph node dissection due to bladder cancer. Urol. Oncol. Semin. Orig. Investig. 2018, 36, 307.e9–307.e14. [Google Scholar] [CrossRef]
- Dhar, N.B.; Klein, E.A.; Reuther, A.M.; Thalmann, G.N.; Madersbacher, S.; Studer, U.E. Outcome After Radical Cystectomy With Limited or Extended Pelvic Lymph Node Dissection. J. Urol. 2008, 179, 873–878. [Google Scholar] [CrossRef]
- Poulsen, A.L.; Horn, T.; Steven, K. Radical Cystectomy: Extending The Limits of Pelvic Lymph Node Dissection Improves Survival for Patients with Bladder Cancer Confined to the Bladder Wall. J. Urol. 1998, 160, 2015–2020. [Google Scholar] [CrossRef]
- Stein, J.P. Lymphadenectomy in bladder cancer: How high is “high enough”? Urol. Oncol. Semin. Orig. Investig. 2006, 24, 349–355. [Google Scholar] [CrossRef]
- Møller, M.K.; Høyer, S.; Jensen, J.B. Extended versus superextended lymph-node dissection in radical cystectomy: Subgroup analysis of possible recurrence-free survival benefit. Scand. J. Urol. 2016, 50, 1–6. [Google Scholar] [CrossRef]
- Zehnder, P.; Studer, U.E.; Skinner, E.C.; Dorin, R.P.; Cai, J.; Roth, B.; Miranda, G.; Birkhäuser, F.; Stein, J.; Burkhard, F.C.; et al. Super Extended Versus Extended Pelvic Lymph Node Dissection in Patients Undergoing Radical Cystectomy for Bladder Cancer: A Comparative Study. J. Urol. 2011, 186, 1261–1268. [Google Scholar] [CrossRef] [PubMed]
- Gschwend, J.E.; Heck, M.M.; Lehmann, J.; Rübben, H.; Albers, P.; Wolff, J.M.; Frohneberg, D.; de Geeter, P.; Heidenreich, A.; Kälble, T.; et al. Extended Versus Limited Lymph Node Dissection in Bladder Cancer Patients Undergoing Radical Cystectomy: Survival Results from a Prospective, Randomized Trial. Eur. Urol. 2019, 75, 604–611. [Google Scholar] [CrossRef]
- Burkhard, F.C.; Thalmann, G.N. No survival benefit with extended lymphadenectomy: Now what? Nat. Rev. Urol. 2019, 16, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. (Eds.) TNM Classification of Malignant Tumours, 8th ed.; John Wiley & Sons: Hoboken, NJ, USA, 2017. [Google Scholar] [CrossRef]
- Wright, J.L.; Lin, D.W.; Porter, M.P. The association between extent of lymphadenectomy and survival among patients with lymph node metastases undergoing radical cystectomy. Cancer 2008, 112, 2401–2408. [Google Scholar] [CrossRef]
- Honma, I.; Masumori, N.; Sato, E.; Maeda, T.; Hirobe, M.; Kitamura, H.; Takahashi, A.; Itoh, N.; Tamakawa, M.; Tsukamoto, T. Removal of more lymph nodes may provide better outcome, as well as more accurate pathologic findings, in patients with bladder cancer—analysis of role of pelvic lymph node dissection. Urology 2006, 68, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.P.; Lieskovsky, G.; Cote, R.; Groshen, S.; Feng, A.-C.; Boyd, S.; Skinner, E.; Bochner, B.; Thangathurai, D.; Mikhail, M.; et al. Radical Cystectomy in the Treatment of Invasive Bladder Cancer: Long-Term Results in 1,054 Patients. J. Clin. Oncol. 2001, 19, 666–675. [Google Scholar] [CrossRef]
- Koppie, T.M.; Vickers, A.J.; Vora, K.; Dalbagni, G.; Bochner, B.H. Standardization of pelvic lymphadenectomy performed at radical cystectomy. Cancer 2006, 107, 2368–2374. [Google Scholar] [CrossRef] [PubMed]
- Herr, H.W.; Bochner, B.H.; Dalbagni, G.; Donat, S.M.; Reuter, V.E.; Bajorin, D.F. Impact of the Number of Lymph Nodes Retrieved on Outcome in Patients with Muscle Invasive Bladder Cancer. J. Urol. 2002, 167, 1295–1298. [Google Scholar] [CrossRef]
- Konety, B.R.; Joslyn, S.A. Factors Influencing Aggressive Therapy for Bladder Cancer: An Analysis of Data from the SEER Program. J. Urol. 2003, 170, 1765–1771. [Google Scholar] [CrossRef] [PubMed]
- Shariat, S.F.; Ehdaie, B.; Rink, M.; Cha, E.K.; Svatek, R.S.; Chromecki, T.F.; Fajkovic, H.; Novara, G.; David, S.G.; Daneshmand, S.; et al. Clinical Nodal Staging Scores for Bladder Cancer: A Proposal for Preoperative Risk Assessment. Eur. Urol. 2012, 61, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Capitanio, U.; Suardi, N.; Shariat, S.F.; Lotan, Y.; Palapattu, G.S.; Bastian, P.J.; Gupta, A.; Vazina, A.; Schoenberg, M.; Lerner, S.P.; et al. Assessing the minimum number of lymph nodes needed at radical cystectomy in patients with bladder cancer. BJU Int. 2009, 103, 1359–1362. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Latif, M.; Abol-Enein, H.; El-Baz, M.; Ghoneim, M.A. Nodal Involvement in Bladder Cancer Cases Treated with Radical Cystectomy: Incidence and Prognosis. J. Urol. 2004, 172, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, A.; Thalmann, G.N.; Markwalder, R.; Studer, U.E. Extracapsular Extension of Pelvic Lymph Node Metastases From Urothelial Carcinoma of the Bladder Is an Independent Prognostic Factor. J. Clin. Oncol. 2005, 23, 2358–2365. [Google Scholar] [CrossRef] [PubMed]
- Lerner, S.P.; Skinner, D.G.; Lieskovsky, G.; Boyd, S.D.; Groshen, S.L.; Ziogas, A.; Skinner, E.; Nichols, P.; Hopwood, B. The Rationale for EN Bloc Pelvic Lymph Node Dissection for Bladder Cancer Patients with Nodal Metastases: Long-Term Results. J. Urol. 1993, 149, 758–764. [Google Scholar] [CrossRef]
- Lee, E.K.; Herr, H.W.; Dickstein, R.J.; Kassouf, W.; Munsell, M.F.; Grossman, H.B.; Dinney, C.P.N.; Kamat, A.M. Lymph node density for patient counselling about prognosis and for designing clinical trials of adjuvant therapies after radical cystectomy. BJU Int. 2012, 110, E590–E595. [Google Scholar] [CrossRef]
- Osawa, T.; Abe, T.; Shinohara, N.; Harabayashi, T.; Sazawa, A.; Kubota, K.; Matsuno, Y.; Shibata, T.; Shinno, Y.; Kamota, S.; et al. Role of lymph node density in predicting survival of patients with lymph node metastases after radical cystectomy: A multi-institutional study. Int. J. Urol. 2009, 16, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.W.; Ng, C.F.; Chan, C.K.; Wong, W.S.; Hui, P.E.; Wong, Y.F. A fourteen-year review of radical cystectomy for transitional cell carcinoma demonstrating the usefulness of the concept of lymp node density. Int. Braz. J. Urol. 2006, 32, 536–549. [Google Scholar] [CrossRef]
- Simone, G.; Papalia, R.; Ferriero, M.; Guaglianone, S.; Naselli, A.; Collura, D.; Introini, C.; Puppo, P.; Muto, G.; Gallucci, M. Development and external validation of lymph node density cut-off points in prospective series of radical cystectomy and pelvic lymph node dissection. Int. J. Urol. 2012, 19, 1068–1074. [Google Scholar] [CrossRef] [Green Version]
- Wiesner, C.; Pfitzenmaier, J.; Faldum, A.; Gillitzer, R.; Melchior, S.W.; Thüroff, J.W. Lymph node metastases in non-muscle invasive bladder cancer are correlated with the number of transurethral resections and tumour upstaging at radical cystectomy. BJU Int. 2005, 95, 301–305. [Google Scholar] [CrossRef]
- Jeong, I.G.; Ro, J.Y.; Kim, S.C.; You, D.; Song, C.; Hong, J.H.; Ahn, H.; Kim, C.-S. Extranodal extension in node-positive bladder cancer: The continuing controversy. BJU Int. 2010, 108, 38–43. [Google Scholar] [CrossRef]
- Kassouf, W.; Svatek, R.S.; Shariat, S.F.; Novara, G.; Lerner, S.P.; Fradet, Y.; Bastian, P.J.; Aprikian, A.; Karakiewicz, P.I.; Fritsche, H.M.; et al. Critical analysis and validation of lymph node density as prognostic variable in urothelial carcinoma of bladder. Urol. Oncol. Semin. Orig. Investig. 2013, 31, 480–486. [Google Scholar] [CrossRef]
- Seiler, R.; Von Gunten, M.; Thalmann, G.N.; Fleischmann, A. Extracapsular extension but not the tumour burden of lymph node metastases is an independent adverse risk factor in lymph node-positive bladder cancer. Histopathology 2011, 58, 571–578. [Google Scholar] [CrossRef]
- Mills, R.; Turner, W.; Fleischmann, A.; Markwalder, R.; Thalmann, G.; Studer, U. Pelvic Lymph Node Metastases from Bladder Cancer: Outcome in 83 Patients After Radical Cystectomy and Pelvic Lymphadenectomy. J. Urol. 2001, 166, 19–23. [Google Scholar] [CrossRef]
- Kassouf, W.; Agarwal, P.K.; Herr, H.W.; Munsell, M.F.; Spiess, P.E.; Brown, G.A.; Pisters, L.; Grossman, H.B.; Dinney, C.P.; Kamat, A.M. Lymph Node Density Is Superior to TNM Nodal Status in Predicting Disease-Specific Survival After Radical Cystectomy for Bladder Cancer: Analysis of Pooled Data From MDACC and MSKCC. J. Clin. Oncol. 2008, 26, 121–126. [Google Scholar] [CrossRef]
- Ahn, T.S.; Kim, H.S.; Jeong, C.W.; Kwak, C.; Kim, H.H.; Ku, J.H. Extracapsular Extension of Pelvic Lymph Node Metastasis is an Independent Prognostic Factor in Bladder Cancer: A Systematic Review and Meta-analysis. Ann. Surg. Oncol. 2015, 22, 3745–3750. [Google Scholar] [CrossRef] [PubMed]
- Frank, I.; Cheville, J.C.; Blute, M.L.; Lohse, C.M.; Nehra, A.; Weaver, A.L.; Karnes, R.J.; Zincke, H. Transitional cell carcinoma of the urinary bladder with regional lymph node involvement treated by cystectomy. Cancer 2003, 97, 2425–2431. [Google Scholar] [CrossRef]
- Stephenson, A.J.; Gong, M.C.; Campbell, S.C.; Fergany, A.F.; Hansel, D.E. Aggregate Lymph Node Metastasis Diameter and Survival After Radical Cystectomy for Invasive Bladder Cancer. Urology 2010, 75, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Kassouf, W.; Leibovici, D.; Munsell, M.F.; Dinney, C.P.; Grossman, H.B.; Kamat, A.M. Evaluation of the Relevance of Lymph Node Density in a Contemporary Series of Patients Undergoing Radical Cystectomy. J. Urol. 2006, 176, 53–57. [Google Scholar] [CrossRef]
- Koren, R.; Paz, A.; Konichezsky, M.; Sadikov, E.; Klein, B.; Livne, P.; Gal, R. Lymph Node Revealing Solution: A Rapid Method for the Fixation of Cystectomy Specimens. Pathol. Res. Pract. 1999, 195, 77–80. [Google Scholar] [CrossRef]
- Vieweg, J.; Gschwend, J.E.; Herr, H.W.; Fair, W.R. Pelvic Lymph Node Dissection Can Be Curative in Patients With Node Positive Bladder Cancer. J. Urol. 1999, 161, 449–454. [Google Scholar] [CrossRef]
- Ghoneim, M.A.; Abdel-Latif, M.; El-Mekresh, M.; Abol-Enein, H.; Mosbah, A.; Ashamallah, A.; El-Baz, M.A. Radical Cystectomy for Carcinoma of the Bladder: 2,720 Consecutive Cases 5 Years Later. J. Urol. 2008, 180, 121–127. [Google Scholar] [CrossRef]
- Meijer, R.; Nunnink, C.; Wassenaar, A.; Bex, A.; Van Der Poel, H.; Van Rhijn, B.; Meinhardt, W.; Horenblas, S. Standard Lymph Node Dissection for Bladder Cancer: Significant Variability in the Number of Reported Lymph Nodes. J. Urol. 2012, 187, 446–450. [Google Scholar] [CrossRef]
- Fang, A.C.; Ahmad, A.E.; Whitson, J.M.; Ferrell, L.D.; Carroll, P.R.; Konety, B.R. Effect of a minimum lymph node policy in radical cystectomy and pelvic lymphadenectomy on lymph node yields, lymph node positivity rates, lymph node density, and survivorship in patients with bladder cancer. Cancer 2010, 116, 1901–1908. [Google Scholar] [CrossRef]
- Shao, P.; Meng, X.; Li, J.; Lv, Q.; Zhang, W.; Xu, Z.; Yin, C. Laparoscopic extended pelvic lymph node dissection during radical cystectomy: Technique and clinical outcomes. BJU Int. 2011, 108, 124–128. [Google Scholar] [CrossRef]
- Leissner, J.; Hohenfellner, R.; Thüroff, J.; Wolf, H. Lymphadenectomy in patients with transitional cell carcinoma of the urinary bladder; significance for staging and prognosis. BJU Int. 2000, 85, 817–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, J.-B.; Zu, X.-B.; Miao, J.-G.; Wang, J.; Chen, M.-F.; Qi, L. Laparoscopic pelvic lymph node dissection system based on preoperative primary tumour stage (T stage) by computed tomography in urothelial bladder cancer: Results of a single-institution prospective study. BJU Int. 2013, 112, E87–E91. [Google Scholar] [CrossRef] [PubMed]
- Leow, J.J.; Bedke, J.; Chamie, K.; Collins, J.W.; Daneshmand, S.; Grivas, P.; Heidenreich, A.; Messing, E.M.; Royce, T.J.; Sankin, A.I.; et al. SIU–ICUD consultation on bladder cancer: Treatment of muscle-invasive bladder cancer. World J. Urol. 2019, 37, 61–83. [Google Scholar] [CrossRef] [PubMed]
- Spiess, P.E.; Agarwal, N.; Bangs, R.; Boorjian, S.A.; Buyyounouski, M.K.; Clark, P.E.; Downs, T.M.; Efstathiou, J.A.; Flaig, T.W.; Friedlander, T.; et al. Bladder Cancer, Version 5.2017, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2017, 15, 1240–1267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, S.S.; Bochner, B.H.; Chou, R.; Dreicer, R.; Kamat, A.M.; Lerner, S.P.; Lotan, Y.; Meeks, J.J.; Michalski, J.M.; Morgan, T.M.; et al. Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline. J. Urol. 2017, 198, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, G.S.; Black, P.C.; Sridhar, S.S.; Kapoor, A.; Zlotta, A.R.; Shayegan, B.; Rendon, R.A.; Chung, P.; Van Der Kwast, T.; Alimohamed, N.; et al. Canadian Urological Association guideline: Muscle-invasive bladder cancer. Can. Urol. Assoc. J. 2019, 13, 230–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parekh, D.J.; Reis, I.M.; Castle, E.P.; Gonzalgo, M.L.; Woods, M.E.; Svatek, R.S.; Weizer, A.Z.; Konety, B.R.; Tollefson, M.; Krupski, T.L.; et al. Robot-assisted radical cystectomy versus open radical cystectomy in patients with bladder cancer (RAZOR): An open-label, randomised, phase 3, non-inferiority trial. Lancet 2018, 391, 2525–2536. [Google Scholar] [CrossRef]
- Bochner, B.H.; Dalbagni, G.; Sjoberg, D.D.; Silberstein, J.; Paz, G.E.K.; Donat, S.M.; Coleman, J.A.; Mathew, S.; Vickers, A.; Schnorr, G.C.; et al. Comparing Open Radical Cystectomy and Robot-assisted Laparoscopic Radical Cystectomy: A Randomized Clinical Trial. Eur. Urol. 2015, 67, 1042–1050. [Google Scholar] [CrossRef] [Green Version]
- Bochner, B.H.; Dalbagni, G.; Marzouk, K.H.; Sjoberg, D.D.; Lee, J.; Donat, S.M.; Coleman, J.A.; Vickers, A.; Herr, H.W.; Laudone, V.P. Randomized Trial Comparing Open Radical Cystectomy and Robot-assisted Laparoscopic Radical Cystectomy: Oncologic Outcomes. Eur. Urol. 2018, 74, 465–471. [Google Scholar] [CrossRef]
- Khan, M.S.; Omar, K.; Ahmed, K.; Gan, C.; Van Hemelrijck, M.; Nair, R.; Thurairaja, R.; Rimington, P.; Dasgupta, P. Long-term Oncological Outcomes from an Early Phase Randomised Controlled Three-arm Trial of Open, Robotic, and Laparoscopic Radical Cystectomy (CORAL). Eur. Urol. 2020, 77, 110–118. [Google Scholar] [CrossRef]
- Khan, M.S.; Gan, C.; Ahmed, K.; Ismail, A.F.; Watkins, J.; Summers, J.A.; Peacock, J.L.; Rimington, P.; Dasgupta, P. A Single-centre Early Phase Randomised Controlled Three-arm Trial of Open, Robotic, and Laparoscopic Radical Cystectomy (CORAL). Eur. Urol. 2016, 69, 613–621. [Google Scholar] [CrossRef] [Green Version]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.; Zheng, J.; Li, Y.; Yu, H.; Shi, S.; Xie, W.; Liu, H.; Su, Y.; Huang, J.; Lin, T. A radiomics nomogram for the preoperative prediction of lymph node metastasis in bladder cancer. Clin. Cancer Res. 2017, 23, 6904–6911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, S.; Zheng, J.; Li, Y.; Wu, Z.; Shi, S.; Huang, M.; Yu, H.; Dong, W.; Huang, J.; Lin, T. Development and Validation of an MRI-Based Radiomics Signature for the Preoperative Prediction of Lymph Node Metastasis in Bladder Cancer. EBioMedicine 2018, 34, 76–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NCT01224665. S1011 Standard or Extended Pelvic Lymphadenectomy in Treating Patients Undergoing Surgery for Invasive Bladder Cancer. Available online: https://ClinicaltrialsGov/Show/NCT012246652010 (accessed on 12 March 2021).
- Rosenblatt, R.; Johansson, M.; Alamdari, F.; Sidiki, A.; Holmström, B.; Hansson, J.; Vasko, J.; Marits, P.; Gabrielsson, S.; Riklund, K.; et al. Sentinel node detection in muscle-invasive urothelial bladder cancer is feasible after neoadjuvant chemotherapy in all pT stages, a prospective multicenter report. World J. Urol. 2017, 35, 921–927. [Google Scholar] [CrossRef] [Green Version]
- Aljabery, F.; Shabo, I.; Olsson, H.; Gimm, O.; Jahnson, S. Radio-guided sentinel lymph node detection and lymph node mapping in invasive urinary bladder cancer: A prospective clinical study. BJU Int. 2016, 120, 329–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polom, W.; Markuszewski, M.; Cytawa, W.; Czapiewski, P.; Lass, P.; Matuszewski, M. Fluorescent Versus Radioguided Lymph Node Mapping in Bladder Cancer. Clin. Genitourin. Cancer 2017, 15, e405–e409. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.S.; Mellman, I. Oncology Meets Immunology: The Cancer-Immunity Cycle. Immunity 2013, 39, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Bellmunt, J.; Powles, T.; Vogelzang, N.J. A review on the evolution of PD-1/PD-L1 immunotherapy for bladder cancer: The future is now. Cancer Treat. Rev. 2017, 54, 58–67. [Google Scholar] [CrossRef] [Green Version]
- Wołącewicz, M.; Hrynkiewicz, R.; Grywalska, E.; Suchojad, T.; Leksowski, T.; Roliński, J.; Niedźwiedzka-Rystwej, P. Immunotherapy in Bladder Cancer: Current Methods and Future Perspectives. Cancers 2020, 12, 1181. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Małkiewicz, B.; Kiełb, P.; Gurwin, A.; Knecht, K.; Wilk, K.; Dobruch, J.; Zdrojowy, R. The Usefulness of Lymphadenectomy in Bladder Cancer—Current Status. Medicina 2021, 57, 415. https://doi.org/10.3390/medicina57050415
Małkiewicz B, Kiełb P, Gurwin A, Knecht K, Wilk K, Dobruch J, Zdrojowy R. The Usefulness of Lymphadenectomy in Bladder Cancer—Current Status. Medicina. 2021; 57(5):415. https://doi.org/10.3390/medicina57050415
Chicago/Turabian StyleMałkiewicz, Bartosz, Paweł Kiełb, Adam Gurwin, Klaudia Knecht, Karol Wilk, Jakub Dobruch, and Romuald Zdrojowy. 2021. "The Usefulness of Lymphadenectomy in Bladder Cancer—Current Status" Medicina 57, no. 5: 415. https://doi.org/10.3390/medicina57050415