
Ventricular Fibrillation Recurrences in Successfully Shocked Out-of-Hospital Cardiac Arrests

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. General Characteristics
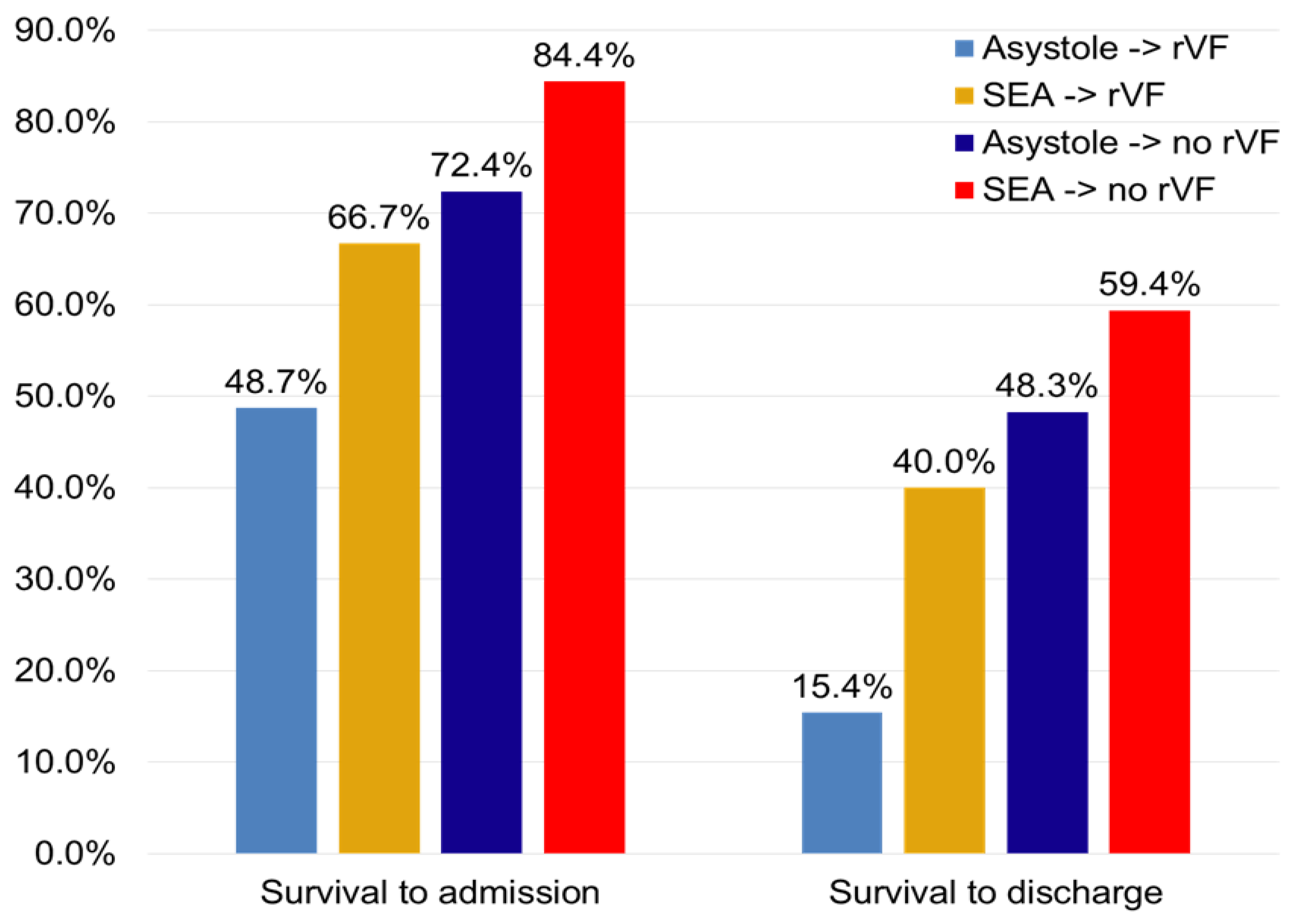
3.2. VF Recurrence and Survival
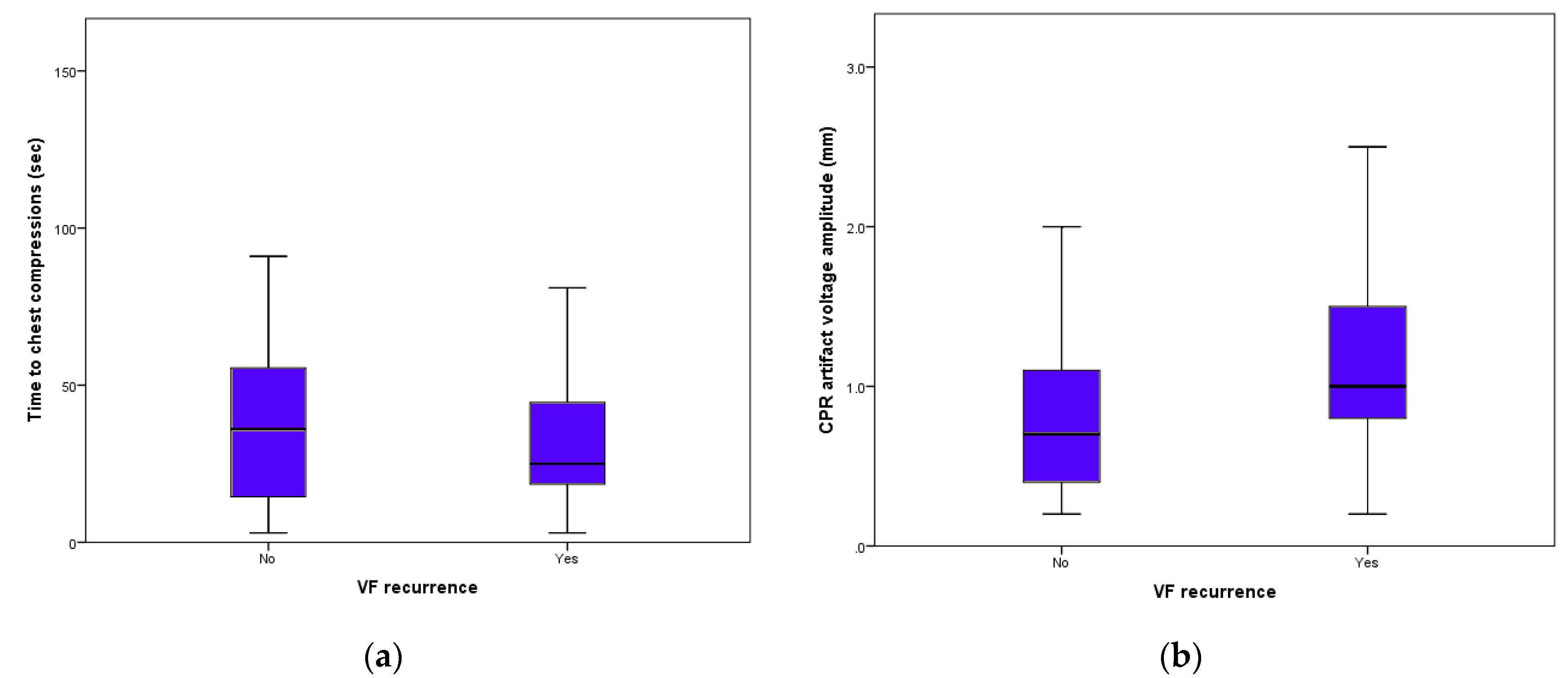
3.3. After-Shock Chest Compressions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neumar, R.W.; Shuster, M.; Callaway, C.W.; Gent, L.M.; Atkins, D.L.; Bhanji, F.; Brooks, S.C.; de Caen, A.R.; Donnino, M.W.; Hazinski, M.F.; et al. Part 1: Executive summary: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2015, 132 (Suppl. 2), S315–S367. [Google Scholar] [CrossRef] [Green Version]
- Maron, B.J.; Estes, I.I.I. NM Commotio cordis. N. Engl. J. Med. 2010, 362, 917–927. [Google Scholar] [CrossRef] [PubMed]
- Kleinman, M.E.; Brennan, E.E.; Goldberger, Z.D.; Swor, R.A.; Terry, M.; Bobrow, B.J.; Gazmuri, R.J.; Travers, A.H.; Rea, T. Part 5: Adult basic life support and cardiopulmonary resuscitation quality: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2015, 132 (Suppl. 2), S414–S435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atwood, C.; Eisenberg, M.S.; Herlitz, J.; Rea, T.D. Incidence of EMS-treated out-of-hospital cardiac arrest in Europe. Resuscitation 2005, 67, 75–80. [Google Scholar] [CrossRef]
- Berdowski, J.; Tijssen, J.G.P.; Koster, R.W. Chest Compressions Cause Recurrence of Ventricular Fibrillation After the First Successful Conversion by Defibrillation in Out-of-Hospital Cardiac Arrest. Circ. Arrhythm. Electrophysiol. 2010, 3, 72–78. [Google Scholar] [CrossRef] [Green Version]
- Capucci, A.; Aschieri, D.; Guerra, F.; Pelizzoni, V.; Nani, S.; Villani, G.Q.; Bardy, G.H. Community-based automated external defibrillator only resuscitation for out-of-hospital cardiac arrest patients. Am. Heart J. 2016, 172, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Aschieri, D.; Penela, D.; Pelizzoni, V.; Guerra, F.; Vermi, A.C.; Rossi, L.; Torretta, L.; Losi, G.; Villani, G.Q.; Capucci, A. Outcomes after sudden cardiac arrest in sports centres with and without on-site external defibrillators. Heart 2018, 104, 1344–1349. [Google Scholar] [CrossRef]
- Krischer, J.P.; Fine, E.G.; Davis, J.H.; Nagel, E.L. Complications of Cardiac Resuscitation. Chest 1987, 92, 287–291. [Google Scholar] [CrossRef]
- Bardy, G.H. A Critic’s Assessment of Our Approach to Cardiac Arrest. N. Engl. J. Med. 2011, 364, 374–375. [Google Scholar] [CrossRef] [Green Version]
- Conover, Z.; Kern, K.B.; Silver, A.E.; Bobrow, B.J.; Spaite, D.W.; Indik, J.H. Resumption of chest compressions after successful defibrillation and risk for recurrence of ventricular fibrillation in out-of-hospital cardiac arrest. Circ. Arrhythm. Electrophysiol. 2014, 7, 633–639. [Google Scholar] [CrossRef] [Green Version]
- Osorio, J.; Dosdall, D.J.; Robichaux, J.R.P.; Tabereaux, P.B.; Ideker, R.E. In a Swine Model, Chest Compressions Cause Ventricular Capture and, By Means of a Long-Short Sequence, Ventricular Fibrillation. Circ. Arrhythm. Electrophysiol. 2008, 1, 282–289. [Google Scholar] [CrossRef] [Green Version]
- Kohl, P.; Bollensdorff, C.; Garny, A. Effects of mechanosensitive ion channels on ventricular electrophysiology: Experimental and theoretical models. Exp. Physiol. 2006, 91, 307–321. [Google Scholar] [CrossRef] [PubMed]
- Osorio, J.; Dosdall, D.J.; Tabereaux, P.B.; Robichaux, R.P.; Stephens, S.; Kerby, J.D.; Stickney, R.E.; Pogwizd, S.; Ideker, R.E. Effect of Chest Compressions on Ventricular Activation. Am. J. Cardiol. 2012, 109, 670–674. [Google Scholar] [CrossRef] [PubMed]
- Skogvoll, E.; Nordseth, T. The early minutes of in-hospital cardiac arrest: Shock or CPR? A population based prospective study. Scand. J. Trauma Resusc. Emerg. Med. 2008, 16, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stiell, I.G.; Walker, R.G.; Chapman, F.W.; Lank, P.; Nesbitt, L.P.; Cousineau, D.; Christenson, J.; Bradford, P.; Sookram, S.; Berringer, R.; et al. Response to Letter Regarding Article, BIPHASIC Trial: A Randomized Comparison of Fixed Lower Versus Escalating Higher Energy Levels for Defibrillation in Out-of-Hospital Cardiac Arrest. Circulation 2007, 116, e523. [Google Scholar] [CrossRef] [Green Version]
- Miller, F.C.; Krucoff, M.W.; Satler, L.F.; E Green, C.; Fletcher, R.D.; A Del Negro, A.; Pearle, D.L.; Kent, K.M.; E Rackley, C. Ventricular arrhythmias during reperfusion. Am. Heart J. 1986, 112, 928–932. [Google Scholar] [CrossRef]
- Henriques, J.P.; Gheeraert, P.J.; Ottervanger, J.P.; De Boer, M.-J.; Dambrink, J.-H.E.; Gosselink, A.M.; Hof, A.W.V.T.; Hoorntje, J.C.; Suryapranata, H.; Zijlstra, F. Ventricular fibrillation in acute myocardial infarction before and during primary PCI. Int. J. Cardiol. 2005, 105, 262–266. [Google Scholar] [CrossRef]
- Berg, R.A.; Sanders, A.B.; Kern, K.B.; Hilwig, R.W.; Heidenreich, J.W.; Porter, M.E.; Ewy, G.A. Adverse hemodynamic effects of interrupting chest compressions for rescue breathing during cardiopulmonary resuscitation for ventricular fibrillation cardiac arrest. Circulation 2001, 104, 2465–2470. [Google Scholar] [CrossRef] [Green Version]
- Cascio, W.E.; Yang, H.; Johnson, T.A.; Muller-Borer, B.J.; Lemasters, J.J. Electrical properties and conduction in reperfused papillary muscle. Circ. Res. 2001, 89, 807–814. [Google Scholar] [CrossRef] [Green Version]
- Berdowski, J.; Haaf, M.T.; Tijssen, J.G.; Chapman, F.W.; Koster, R.W. Time in Recurrent Ventricular Fibrillation and Survival After Out-of-Hospital Cardiac Arrest. Circulation 2010, 122, 1101–1108. [Google Scholar] [CrossRef] [Green Version]
- Telesz, B.J.; Hess, E.P.; Atkinson, E.; White, R.D. Recurrent ventricular fibrillation: Experience with first responders prior to advanced life support interventions. Resuscitation 2015, 88, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Guerra, F.; Flori, M.; Bonelli, P.; Patani, F.; Capucci, A. Electrical storm and heart failure worsening in implantable cardiac defibrillator patients. Europace 2014, 17, 247–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerra, F.; Palmisano, P.; Dell’Era, G.; Ziacchi, M.; Ammendola, E.; Pongetti, G.; Bonelli, P.; Patani, F.; Devecchi, C.; Accogli, M.; et al. Cardiac resynchronization therapy and electrical storm: Results of the OBSERVational registry on long-term outcome of ICD patients (OBSERVO-ICD). Europace 2017, 20, 979–985. [Google Scholar] [CrossRef] [PubMed]
- Straznitskas, A.D.; Wong, S.; Kupchik, N.; Carlbom, D. Secondary ventricular fibrillation or pulseless ventricular tachycardia during cardiac arrest and epinephrine dosing. Am. J. Crit. Care 2015, 24, e22–e27. [Google Scholar] [CrossRef] [PubMed]
- Guerra, F.; Malagoli, A.; Contadini, D.; Baiocco, E.; Menditto, A.; Bonelli, P.; Rossi, L.; Sticozzi, C.; Zanni, A.; Cai, J.; et al. Global Longitudinal Strain as a Predictor of First and Subsequent Arrhythmic Events in Remotely Monitored ICD Patients with Structural Heart Disease. Jacc Cardiovasc. Imaging 2020, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Matsuura, T.R.; Bartos, J.A.; Tsangaris, A.; Shekar, K.C.; Olson, M.D.; Riess, M.L.; Bienengraeber, M.; Aufderheide, T.P.; Neumar, R.W.; Rees, J.N.; et al. Early Effects of Prolonged Cardiac Arrest and Ischemic Postconditioning during Cardiopulmonary Resuscitation on Cardiac and Brain Mitochondrial Function in Pigs. Resuscitation 2017, 116, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Bjørshol, C.A.; Myklebust, H.; Nilsen, K.L.; Hoff, T.; Bjørkli, C.; Illguth, E.; Søreide, E.; Sunde, K. Effect of socioemotional stress on the quality of cardiopulmonary resuscitation during advanced life support in a randomized manikin study. Crit. Care Med. 2011, 39, 300–304. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Shockable Rhythms | Excluded Patients | Included Patients | |
|---|---|---|---|
| 461 | 298 | 163 | |
| Age (years) | 63.3 ± 15.4 | 62.6 ± 16.3 | 64.4 ± 16.9 |
| male gender | 325 (70.5%) | 214 (71.8%) | 111 (68.1%) |
| mean time to arrival (min) | 5.8 ± 3.7 | 5.7 ± 4.2 | 5.9 ± 4.5 |
| Location of cardiac arrest | |||
| Home | 360 (78.1%) | 234 (78.5%) | 126 (77.3%) |
| Public places | 101 (21.9%) | 64 (21.5%) | 37 (22.7%) |
| Initial responder | |||
| Progetto Vita | 65 (14.1%) | 40 (13.4%) | 25 (15.3%) |
| BLS EMS | 219 (47.5%) | 133 (44.6%) | 86 (52.8%) |
| ACLS EMS | 177 (38.4%) | 125 (41.9%) | 52 (31.9%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aschieri, D.; Guerra, F.; Pelizzoni, V.; Paolini, E.; Stronati, G.; Moderato, L.; Losi, G.; Compagnucci, P.; Coccia, M.; Casella, M.; et al. Ventricular Fibrillation Recurrences in Successfully Shocked Out-of-Hospital Cardiac Arrests. Medicina 2021, 57, 358. https://doi.org/10.3390/medicina57040358
Aschieri D, Guerra F, Pelizzoni V, Paolini E, Stronati G, Moderato L, Losi G, Compagnucci P, Coccia M, Casella M, et al. Ventricular Fibrillation Recurrences in Successfully Shocked Out-of-Hospital Cardiac Arrests. Medicina. 2021; 57(4):358. https://doi.org/10.3390/medicina57040358
Chicago/Turabian StyleAschieri, Daniela, Federico Guerra, Valentina Pelizzoni, Enrico Paolini, Giulia Stronati, Luca Moderato, Giulia Losi, Paolo Compagnucci, Michela Coccia, Michela Casella, and et al. 2021. "Ventricular Fibrillation Recurrences in Successfully Shocked Out-of-Hospital Cardiac Arrests" Medicina 57, no. 4: 358. https://doi.org/10.3390/medicina57040358