
Association of Colonic Diverticula with Colorectal Adenomas and Cancer

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Colonoscopy and Histopathology
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rondagh, E.J.A.; Sanduleanu, S.; Leclercq, C.M.C.; Winkens, B.; Masclee, A.A.M. Diverticulosis and colorectal polyps at a younger age: A possible link? Eur. J. Gastroenterol. Hepatol. 2011, 23, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Strate, L.L.; Modi, R.; Cohen, E.; Spiehel, B.M.R. Diverticular disease as a chronic illness: Evolving epidemiologic and clinical insights. Am. J. Gastroenterol. 2012, 107, 1486–1493. [Google Scholar] [CrossRef] [PubMed]
- Boynton, W.; Floch, M. New strategies for the management of diverticular disease: Insights for the clinician. Therap. Adv. Gastroenterol. 2013, 6, 205–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matrana, M.R.; Margolin, D.A. Epidemiology and pathophysiology of diverticular disease. Clin. Colon Rectal. Surg. 2009, 22, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Cuomo, R.; Barbara, G.; Pace, F.; Annese, V.; Bassotti, G.; Binda, G.A.; Casetti, T.; Colecchia, A.; Festi, D.; Fiocca, R.; et al. Italian consensus conference for colonic diverticulosis and diverticular disease. United Eur. Gastroenterol. J. 2014, 2, 413–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.; Jung, C.W.; Kim, K.; Kim, S.J.; Kim, W.S.; Jang, J.H. Iron deficient erythropoiesis might play key role in development of anemia in cancer patients. Oncotarget 2015, 40, 42803–42812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.H.; Hinshaw, J.L.; Kim, D.H.; Pickhardt, P.J. Symptomatic versus asymptomatic colorectal cancer: Predictive features at CT colonography. Acad. Radiol. 2016, 23, 712–717. [Google Scholar] [CrossRef]
- Lin, J.S.; Piper, M.A.; Perdue, L.A.; Rutter, C.M.; Webber, E.M.; O′Connor, E.; Smith, N.; Whitlock, E.P. Screening for colorectal cancer: Updated evidence report and systematic review for the US preventive services task force. JAMA 2016, 315, 2576–2594. [Google Scholar] [CrossRef] [Green Version]
- Paimela, H.; Malila, N.; Palva, T.; Hakulinen, T.; Vertio, H.; Järvinen, H. Early detection of colorectal cancer with faecal occult blood test screening. Br. J. Surg. 2010, 97, 1567–1571. [Google Scholar] [CrossRef]
- Hreinsson, J.P.; Jonasson, J.G.; Bjornsson, E.S. Bleeding-related symptoms in colorectal cancer: A 4-year nationwide population-based study. Aliment. Pharm. Ther. 2014, 39, 77–84. [Google Scholar] [CrossRef]
- Comparato, G.; Pilotto, A.; Franzè, A.; Franceschi, M.; Di Mario, F. Diverticular disease in the elderly. Dig. Dis. 2007, 25, 2151–2159. [Google Scholar] [CrossRef] [PubMed]
- Altobelli, E.; Lattanzi, A.; Paduano, R.; Varassi, G.; di Orio, F. Colorectal cancer prevention in Europe: Burden of disease and status of screening programs. Prev. Med. 2014, 62, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Altobelli, E.; D’Aloisio, F.; Angeletti, P.M. Colorectal cancer screening in countries of European Council outside of the EU-28. World J. Gastroenterol. 2016, 22, 4946–4957. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Eser, S.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, 359–386. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, J.H.; Enns, R.; Heidelbaugh, J.; Barkun, A. Clinical guidelines committee. American gastroenterological association institute guideline on the diagnosis and management of Lynch syndrome. Gastroenterology 2015, 149, 777–782. [Google Scholar] [CrossRef] [Green Version]
- Samadder, N.J.; Jasperson, K.; Burt, R.W. Hereditary and common familial colorectal cancer: Evidence for colorectal screening. Dig. Dis. Sci. 2015, 60, 734–747. [Google Scholar] [CrossRef]
- Sebastian, S.; Hernández, V.; Myrelid, P.; Kariv, R.; Tsianos, E.; Tsianos, E.; Marti-Gallostra, M.; Spinelli, A.; van der Meulen-de Jong, A.E.; Yuksel, E.S.; et al. Colorectal cancer in inflammatory bowel disease: Results of the 3rd ECCO pathogenesis scientific workshop (I). J. Crohns Colitis 2014, 8, 5–18. [Google Scholar] [CrossRef]
- Cannon, J. Colorectal neoplasia and inflammatory bowel disease. Surg. Clin. N. Am. 2015, 95, 1261–1269. [Google Scholar] [CrossRef]
- Parian, A.; Lazarev, M. Who and how to screen for cancer in at-risk inflammatory bowel disease patients. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 731–746. [Google Scholar] [CrossRef]
- Breynaert, C.; Vermeire, S.; Rutgeerts, P.; Van Assche, G. Dysplasia and colorectal cancer in inflammatory bowel disease: A result of inflammation or an intrinsic risk? Acta Gastroenterol. Belg. 2008, 71, 367–372. [Google Scholar]
- Brenner, H.; Hoffmeister, M.; Stegmaier, C.; Brenner, G.; Altenhofen, L.; Altenhofen, L. Risk of progression of advanced adenomas to colorectal cancer by age and sex: Estimates based on 840,149 screening colonoscopies. Gut 2007, 56, 1585–1589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chacko, L.; Macaron, C.; Burke, C.A. Colorectal cancer screening and prevention in women. Dig Dis Sci. 2015, 60, 698–710. [Google Scholar] [CrossRef] [PubMed]
- Erlinger, T.P.; Platz, E.A.; Rifai, N.; Helzlsouer, K.J. C-reactive protein and the risk of incident colorectal cancer. JAMA 2004, 291, 585–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, K.; Karin, M. Tumor-elicited inflammation and colorectal cancer. Adv. Cancer Res. 2015, 128, 173–196. [Google Scholar]
- Tursi, A.; Brandimarte, G.; Elisei, W.; Giorgetti, G.M.; Inchingolo, C.D.; Danese, S.; Aiello, F. Assessment and grading of mucosal inflammation in colonic diverticular disease. J. Clin. Gastroenterol. 2008, 42, 699–703. [Google Scholar] [CrossRef]
- Morini, S.; Hassan, C.; Zullo, A.; De Francesco, V.; Festa, V.; Barberani, F.; Faleo, D.; Stroffolini, T. Diverticular disease as a risk factor for sigmoid colon adenomas. Dig. Liv. Dis. 2002, 34, 635–639. [Google Scholar] [CrossRef]
- Ashktorab, H.; Panchal, H.; Shokrani, B.; Paydar, M.; Sanderson, A.; Lee, E.L.; Begum, R.; Haidary, T.; Laiyemo, A.O.; McDonald-Pinkett, S.; et al. Association between diverticular disease and pre-neoplastic colorectal lesions in an urban African-American population. Digestion 2015, 92, 60–65. [Google Scholar] [CrossRef] [Green Version]
- Gohil, V.B.; Patrie, J.T.; Shami, V.M.; Sauer, B.G.; Argo, C.K.; Crowe, S.E.; Wang, A.Y. Colonic diverticulosis is associated with an increased adenoma detection rate in patients undergoing first-time screening colonoscopy. J. Interv. Gastroenterol. 2012, 2, 70–75. [Google Scholar] [CrossRef]
- Muhammad, A.; Lamendola, O.; Daas, A.; Kumar, A.; Kumar, A. Association between colonic diverticulosis and prevalence of colorectal polyps. Int. J. Colorectal Dis. 2014, 29, 947–951. [Google Scholar] [CrossRef]
- Meurs-Szojda, M.M.; Terhaar sive Droste, J.S.; Kuik, D.J.; Mulder, C.J.; Felt-Bersma, R.J. Diverticulosis and diverticulitis form no risk for polyps and colorectal neoplasia in 4241 colonoscopies. Int. J. Colorectal Dis. 2008, 23, 979–984. [Google Scholar] [CrossRef] [Green Version]
- Granlund, J.; Svensson, T.; Granath, F.; Hjern, F.; Ekbom, A.; Blomqvist, P.; Schmidt, P.T. Diverticular disease and the risk of colon cancer-a populationbased case-control study. Aliment. Pharmacol. Ther. 2011, 34, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Peery, A.F.; Martin, C.F.; Levinson, S.E.; Sandler, R.S. Colonic diverticula are not associated with an increased risk of colorectal adenomas. Am. J. Gastroenterol. 2015, 110, 1694–1697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calderwood, A.H.; Schroy, P.C., 3rd; Lieberman, D.A.; Logan, J.R.; Zurfluh, M.; Jacobson, B.C. Boston Bowel Preparation Scale scores provide a standardized definition of adequate for describing bowel cleanliness. Gastrointest. Endosc. 2014, 80, 269–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tursi, A.; Papa, A.; Danese, S. Review article: The pathophysiology and medical management of diverticulosis and diverticular disease of the colon. Aliment. Pharmacol. Ther. 2015, 42, 664–684. [Google Scholar] [CrossRef]
- McCallum, A.; Eastwood, M.A.; Smith, A.N.; Fulton, P.M. Colonic diverticulosis in patients with colorectal cancer and in controls. Scand. J. Gastroenterol. 1988, 23, 284–286. [Google Scholar] [CrossRef]
- Morini, S.; de Angelis, P.; Manurita, L.; Colavolpe, V. Association of colonic diverticula with adenomas and carcinomas. A colonoscopic experience. Dis. Colon Rectum. 1988, 31, 793–796. [Google Scholar] [CrossRef]
- Stefánsson, T.; Ekbom, A.; Sparèn, P.; Påhlman, L. Increased risk of left sided colon cancer in patients with diverticular disease. Gut 1993, 34, 499–502. [Google Scholar] [CrossRef] [Green Version]
- Yusuf, M.A.; Rafique, N.; Kausar, R.; Saeed, K. Absence of diverticular disease in a group of patients with colorectal carcinoma. Gastrointest Endosc. 2000, 51, AB235. [Google Scholar]
- Loffeld, R.J.; Van Der Putten, A.B. Diverticular disease of the colon and concomitant abnormalities in patients undergoing endoscopic evaluation of the large bowel. Colorectal Dis. 2002, 4, 189–192. [Google Scholar] [CrossRef]
- Stefánsson, T.; Ekbom, A.; Sparèn, P.; Påhlman, L. Association between sigmoid diverticulitis and left-sided colon cancer: A nested, population-based, case control study. Scand. J. Gastroenterol. 2004, 39, 743–747. [Google Scholar] [CrossRef]
- Kieff, B.J.; Eckert, G.J.; Imperiale, T.F. Is diverticulosis associated with colorectal neoplasia? A cross-sectional colonoscopic study. Am. J. Gastroenterol. 2004, 99, 2007–2011. [Google Scholar] [CrossRef] [PubMed]
- Rajendra, S.; Ho, J.J. Colonic diverticular disease in a multiracial Asian patient population has an ethnic predilection. Eur. J. Gastroenterol. Hepatol. 2005, 17, 871–875. [Google Scholar] [CrossRef] [PubMed]
- Soran, A.; Harlak, A.; Wilson, J.W.; Nesbitt, L.; Lembersky, B.C.; Wienad, H.S.; O′Connell, M.J. Diverticular disease in patients with colon cancer: Subgroup analysis of national surgical adjuvant breast and bowel project protocol C-06. Clin. Colorectal Cancer 2006, 6, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Krones, C.J.; Klinge, U.; Butz, N.; Junge, K.; Stumpf, M.; Rosch, R.; Hermanns, B.; Hermanns, B.; Hermanns, B. The rare epidemiologic coincidence of diverticular disease and advanced colonic neoplasia. Int. J. Colorectal Dis. 2006, 21, 18–24. [Google Scholar] [CrossRef]
- Choi, C.S.; Choi, S.C.; Seo, G.S.; Cho, E.Y.; Cho, H.J.; Kim, Y.S.; Kim, K.H.; Kim, T.H.; Nah, Y.H. Association between diverticulosis and colonic Neoplasm in Koreans. Korean J. Gastroenterol. 2007, 49, 364–368. [Google Scholar] [PubMed]
- Rangnekar, A.S.; Tokayer, A.Z. Low frequency of colon polyps in association with diverticulosis. Am. J. Gastroenterol. 2007, 102, S562–S563. [Google Scholar] [CrossRef]
- Hirata, T.; Kawakami, Y.; Kinjo, N.; Arakaki, S.; Arakaki, T.; Hokama, A.; Kinjo, F.; Fujita, J. Association between colonic polyps and diverticular disease. World J. Gastroenterol. 2008, 14, 2411–2413. [Google Scholar] [CrossRef]
- Hammoud, I.; Sharif, O.; Hannat, N.A.L.; Nawras, A. Co-incidence of diverticulosis and polyps in the colon. Am. J. Gastroenterol. 2009, 104, S165–S166. [Google Scholar] [CrossRef]
- Lee, K.M.; Paik, C.N.; Chung, W.C.; Jung, S.H.; Chang, U.; Yang, J.M. Clinical significance of colonic diverticulosis associated with bowel symptoms and colon polyp. J. Korean Med. Sci. 2010, 25, 1323–1329. [Google Scholar] [CrossRef] [Green Version]
- Mazumder, M.K.; Atluri, S.; Changela, K.; Anand, S.; Nigar, S. Diverticulosis and colonic polyps: Direct link versus common etiology? A look at a minority population. Gastroenterology 2011, 140, S567–S568. [Google Scholar] [CrossRef]
- Neubauer, K.; Dudkowiak, R.; Kempinski, R.; Bak, A.; Paradowski, L. Colonic diverticulosis and risk of large bowel adenomas. Adv. Clin. Exp. Med. 2011, 20, 623–626. [Google Scholar]
- Szura, M.; Zajac, A.; Kulig, J. Colonic diverticula coexisting with other lesions in the colon visualized by colonoscopy. Surg. Endosc. 2011, 25, S103. [Google Scholar]
- Lee, S.J.; Kim, S.; Ku, B.H.; Kim, H.Y.; Kim, J.Y.; Chang, D.K.; Son, H.J.; Shim, S.G.; Rhee, P.L.; Kim, J.J. Association between colorectal cancer and colonic diverticulosis: Case–control study based on computed tomographic colonography. Abdom. Imaging 2012, 37, 70–73. [Google Scholar] [CrossRef]
- Azzam, N.; Aljebreen, A.M.; Alharbi, O.; Almadi., M.A. Prevalence and clinical features of colonic diverticulosis in a Middle Eastern population. World J. Gastrointest Endosc. 2013, 5, 391–397. [Google Scholar] [CrossRef]
- Parava, P.; Azizi, S.; Singh, M.; Richter, S. Diverticular disease and its association with colorectal polyps. Am. J. Gastroenterol. 2013, 108, S181–S182. [Google Scholar] [CrossRef]
- Lecleire, S.; Nahon, S.; Alatawi, A.; Antonietti, M.; Chaput, U.; Di-Fiore, A.; Alhameedi, R.; Marteau, P.; Ducrott, P.; Dray, X. Diagnostic impact of routine colonoscopy following acute diverticulitis: A multicenter study in 808 patients and controls. United Eur. Gastroenterol. J. 2014, 2, 301–306. [Google Scholar] [CrossRef] [Green Version]
- Meda, S.; Parcha, S.; Talla, H.; Vemulapalli, V.; Vemuru, T.; Vemuru, R. Impact of diverticulosis on adenoma/ polyp detection. Am. J. Gastroenterol. 2014, 109, S619. [Google Scholar] [CrossRef]
- Shen, H.; Lipka, S.; Silpe, J.; White, A.; Satler, S.; Luebbers, D.; Statler, J.; Zheng, A.; Elder, J.; Abraham, A. Association Between Diverticulosis and Colorectal Adenomas: A Cross-Sectional Study. Am. J. Gastroenterol. 2014, 109, S209. [Google Scholar] [CrossRef]
- Huang, W.Y.; Lin, C.C.; Jen, Y.M.; Chang, Y.J.; Hsiao, C.W.; Yang, M.H.; Lin, C.S.; Sung, F.C.; Liang, J.A.; Kao, C.H. Association between colonic diverticular disease and colorectal cancer: A nationwide population-based study. Clin. Gastroenterol. Hepatol. 2014, 12, 1288–1294. [Google Scholar] [CrossRef]
- Wang, F.W.; Chuang, H.Y.; Tu, M.S.; King, T.M.; Wang, J.H.; Hsu, C.W.; Hsu, P.I.; Chen, W.C. Prevalence and risk factors of asymptomatic colorectal diverticulosis in Taiwan. BMC Gastroenterol. 2015, 15, 40. [Google Scholar] [CrossRef] [Green Version]
- Wong, E.R.; Idris, F.; Chong, C.F.; Telisinghe, P.U.; Tan, J.; Chong, V.H. Diverticular disease and colorectal neoplasms: Association between left sided diverticular disease with colorectal cancers and right sided with colonic polyps. Asian Pac. J. Cancer Prev. 2016, 17, 2401–2405. [Google Scholar] [PubMed]
- Levine, I.; Rangnekar, A.S.; Tokayer, A.Z. Low frequency of polyps in colonic regions with diverticulosis. Int. J. Colorectal Dis. 2017, 32, 1597–1602. [Google Scholar] [CrossRef]
- Shah, R.; Mann, A.; Kung, J.; Prajapati, D. Colonic diverticulosis associated with an increased risk of adenomas. Am. J. Gastroenterol. 2017, 112, S152. [Google Scholar] [CrossRef]
- Teixeira, C.; Trabulo, D.; Ribeiro, S.; Martins, C.R.; Alves, A.L.; Cremers, I.; Oliveira, A.P. Colonic diverticulosis and the metabolic syndrome: An association? Rev. Esp. Enferm. Dig. 2017, 109, 768–771. [Google Scholar] [CrossRef] [PubMed]
- Hong, W.; Dong, L.; Zippi, M.; Stock, S.; Geng, W.; Xu, C.; Zhou, M. Colonic diverticulosis is not a risk factor for colonic adenoma. Ther. Clin. Risk. Manag. 2018, 14, 531–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavão Borges, V.; Mendez Santos, S.; Vale Rodrigues, R.; Capela, T.; Silva, M.J.; Vasconcelos Loureiro, R.; Bernardes, C.; Russo, P.; Saiote, J. Colonic diverticula: Risk factor for colorectal adenomas? United Eur. Gastroenterol. J. 2018, 6, A690. [Google Scholar]
- Rodriguez-Castro, K.; Baldassarre, G.; Ferronato, A.; Miraglia, C.; Cambiè, G.; Violi, A.; Cuoco, L.; Tursi, A.; Cerofolini, A.; Di Mario, F.; et al. Diverticular disease: Real-life prevalence and associated risk factors in a high-volume endoscopic unit. United Eur. Gastroenterol. J. 2018, 6, A691. [Google Scholar]
- Schramm, C.; Kütting, F.; Lang, S.; Kasper, P.; Chon, S.H.; Steffen, H.M. Hyperplastic polyps and nonadvanced adenomas, but not advanced polypoid lesions, are detected more frequently in the presence of colonic diverticula during screening colonoscopies. Z. Gastroenterol. 2018, 56, 1475–1480. [Google Scholar] [CrossRef]
- Wang, S.F.; Li, C.Y.; Dai, Z.M.; Wang, Z.K.; Peng, L.H.; Zhang, X.L.; Li, J.F.; Yang, Y.S.; Hu, B.; Ning, S.B. Gender, age, and concomitant diseases of colorectal diverticulum in china: A study of 7964 cases. Dig Dis. 2019, 37, 116–122. [Google Scholar] [CrossRef]
- Tomaoglu, K. Association between colonic diverticulosis and colorectal polyps, advanced neoplastic lesions, and colorectal carcinomas: A cross-sectional, retrospective study. Surg. Laparosc. Endosc. Percutan. Tech. 2019. [Google Scholar] [CrossRef]
- Lee, H.J.; Park, S.J.; Cheon, J.H.; Kim, T.I.; Kim, W.H.; Kim, H.J. The relationship between diverticulosis and colorectal neoplasia: A meta-analysis. PLoS ONE 2019, 14, e0216380. [Google Scholar] [CrossRef] [PubMed]
- Tursi, A. Biomarkers in diverticular diseases of the colon. Dig. Dis. 2012, 30, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Arévalo, F.; Aguilar, R.; Ramos, C.; Arias, J.; Castillo, S.; Monge, E. Inflamatory polyps of the colon an evaluation. Rev. Gastroenterol. Peru. 2009, 29, 40–43. [Google Scholar] [PubMed]
- Tony, J.; Harish, K.; Ramachandran, T.M.; Sunilkumar, K.; Thomas, V. Profile of colonic polyps in a southern Indian population. Indian J. Gastroenterol. 2007, 26, 127–129. [Google Scholar]
- Sussman, D.A.; Barkin, J.A.; Martin, A.M.; Arias, J.; Castillo, S.; Monge, E. Development of advanced imaging criteria for the endoscopic identification of inflammatory polyps. Clin. Transl. Gastroenterol. 2015, 6, e128. [Google Scholar] [CrossRef]
- Tursi, A.; Brandimarte, G.; Elisei, W.; Inchingolo, C.D.; Aiello, F. Epithelial cell proliferation of the colonic mucosa in different degrees of colonic diverticular disease. J. Clin. Gastroenterol. 2006, 40, 306–311. [Google Scholar] [CrossRef]
- Simpson, J.; Scholefield, J.H.; Spiller, R.C. Pathogenesis of colonic diverticula. Br. J. Surg. 2002, 89, 546–554. [Google Scholar] [CrossRef]
- Tursi, A. Diverticulosis today: Unfashionable and still under-researched. Therap. Adv. Gastroenterol. 2016, 9, 213–228. [Google Scholar] [CrossRef] [Green Version]
- Bultman, S.J. Interplay between diet, gut microbiota, epigenetic events, and colorectal cancer. Mol. Nutr. Food Res. 2017, 61. [Google Scholar] [CrossRef] [Green Version]
- Gagnière, J.; Raisch, J.; Veziant, J.; Barnich, N.; Bonnet, R.; Buc, E.; Bringer, M.A.; Pezet, D.; Bonnet, M. Gut microbiota imbalance and colorectal cancer. World J. Gastroenterol. 2016, 22, 501–518. [Google Scholar] [CrossRef] [PubMed]
- Ullman, T.A.; Itzkowitz, S.H. Intestinal inflammation and cancer. Gastroenterology 2011, 140, 1807–1816. [Google Scholar] [CrossRef] [PubMed]
- Eaden, J.A.; Abrams, K.R.; Mayberry, J.F. The risk of colorectal cancer in ulcerative colitis: A meta-analysis. Gut 2001, 48, 526–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francescone, R.; Hou, V.; Grivennikov, S.I. Cytokines, IBD, and colitis-associated cancer. Inflamm. Bowel. Dis. 2015, 21, 409–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dyson, J.K.; Rutter, M.D. Colorectal cancer in inflammatory bowel disease: What is the real magnitude of the risk? World J. Gastroenterol. 2012, 18, 3839–3848. [Google Scholar] [CrossRef]
- Morini, S.; Hassan, C.; Zullo, A.; De Francesco, V.; Burattini, O.; Margiotta, M.; Panella, C.; Ierardi, E. Epithelial cell proliferation of the colonic mucosa in diverticular disease: A case-control study. Aliment. Pharmacol. Ther. 2005, 21, 1385–1390. [Google Scholar] [CrossRef]
- Tontini, G.E.; Pastorelli, L.; Spina, L.; Fabris, F.; Bruni, B.; Clemente, C.; de Nucci, G.; Cavallaro, F.; Marconi, S.; Neurath, M.F. Microscopic colitis and colorectal neoplastic lesion rate in chronic nonbloody diarrhea: A prospective, multicenter study. Inflamm. Bowel Dis. 2014, 20, 882–891. [Google Scholar] [CrossRef]
- Sonnenberg, A.; Genta, R.M. Low prevalence of colon polyps in chronic inflammatory conditions of the colon. Am. J. Gastroenterol. 2015, 110, 1056–1061. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| GROUP A | GROUP B | GROUP C | GROUP D | |
|---|---|---|---|---|
| Diverticula | Polyps or Cancer | Polyps or Cancer and Diverticula | No Diverticula, Polyps, or Cancer | |
| (N.183) | (N.204) | (N.168) | (N.935) | |
| Age (Years) | ||||
| Median (Range) | 68 (27–92) | 63 (21–93) | 68 (47–92) | 65 (29–90) |
| Sex | ||||
| Female N (%) | 88 (48%) | 95 (47%) | 64 (38%) | 410 (44%) |
| Male N (%) | 95 (52%) | 109 (53%) | 104 (62%) | 525 (56%) |
| Family history of CRC | ||||
| Negative N (%) | 166 (90.71%) | 152 (74.51%) | 143 (85.12%) | 783 (83.74%) |
| Positive N (%) | 17 (9.29%) | 52 (25.49%) | 25 (14.88%) | 152 (16.26%) |
| Family history of DD | ||||
| Negative N (%) | 178 (97.27%) | 202 (99.02) | 160 (95.24%) | 910 (97.33%) |
| Positive N (%) | 5 (2.73%) | 2 (0.98) | 8 (4.76%) | 25 (2.67%) |
| Localization of Diverticula in the Colon Tracts | Histology | |||
|---|---|---|---|---|
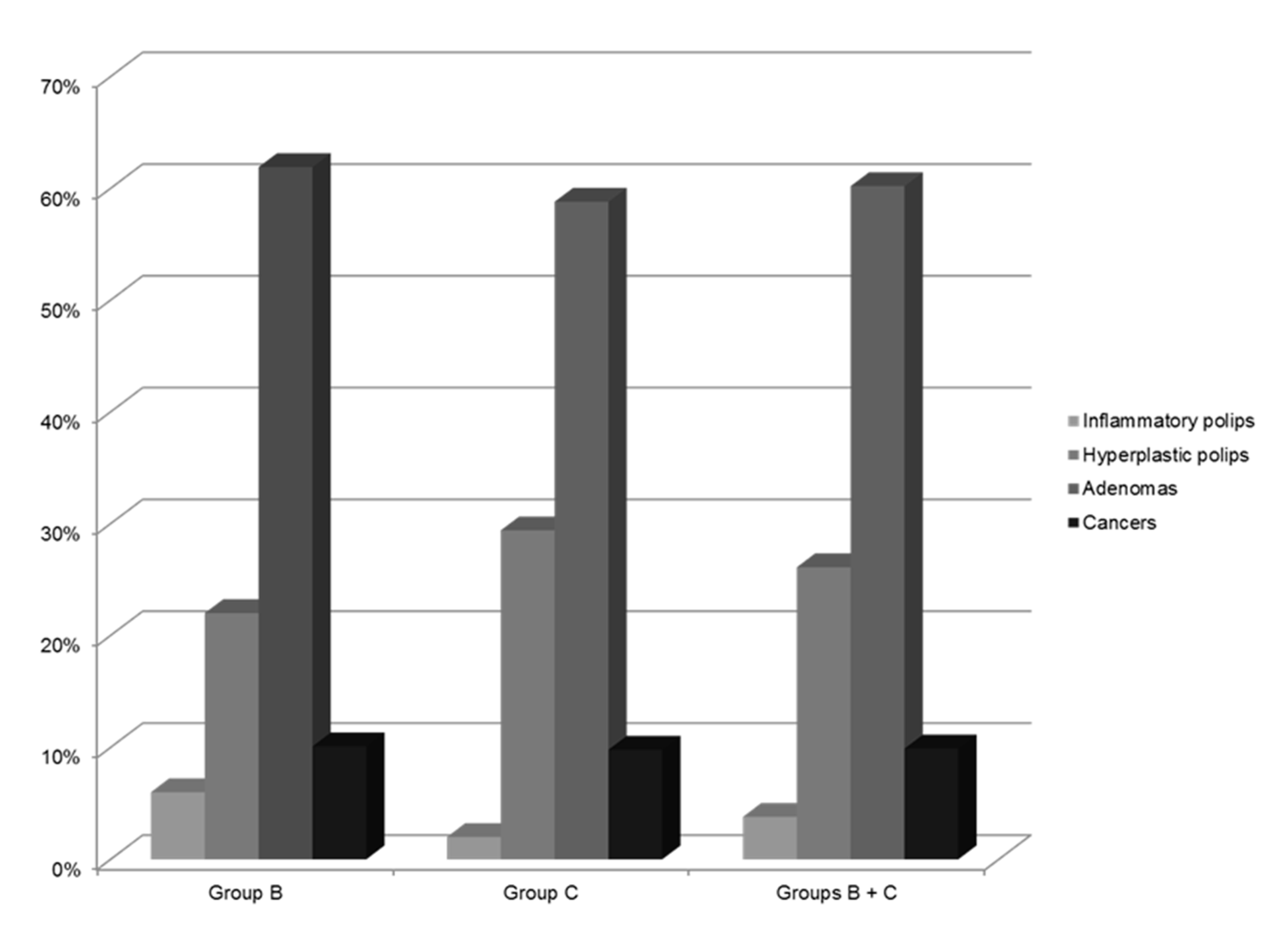
| Inflammatory Polyps N (%) 10 (6.0%) | Hyperplastic Polyps N (%) 37 (22.0%) | Adenomas N (%) 104 (61.9%) | Cancer N (%) 17 (10.1%) | |
| Proximal colon | 0 | 2 (5.4%) | 2 (1.9%) | 2 (11.8%) |
| Distal colon | 10 (100%) | 29 (78.4%) | 70 (67.3%) | 15 (88.2%) |
| Proximal and distal colon | 0 | 6 (16.2%) | 32 (30.8%) | 0 |
| Polyps and Cancers | Diverticula | Total | |
|---|---|---|---|
| Absent | Present | ||
| Absent | 935 | 183 | 1118 (75.0%) |
| Present | 204 | 168 | 372 (25.0%) |
| Total | 1139 | 351 | 1490 |
| Relative risk 2.67 | |||
| 95% CI 2.27 to 3.15 | |||
| Significance level p < 0.0001 | |||
| Adenoma and Cancers | Diverticula | Total | |
|---|---|---|---|
| Absent | Present | ||
| Absent | 999 | 230 | 1229 (82.5%) |
| Present | 140 | 121 | 261 (17.5%) |
| Total | 1139 | 351 | 1490 |
| Relative risk 2.81 | |||
| 95% CI 2.27 to 3.47 | |||
| Significance level p < 0.0001 | |||
| Variables | Odds Ratio | p Value |
|---|---|---|
| (95% CI) | ||
| Age | ||
| per year | 1.00 (0.99–1.01) | 0.753 |
| Sex | ||
| female | 1 (reference) | 0.836 |
| male | 0.97 (0.74–1.28) | |
| Family history of CRC | ||
| No | 1 (reference) | 0.162 |
| Yes | 1.32 (0.90–1.94) | |
| Family history of DD | ||
| No | 1 (reference) | 0.467 |
| Yes | 0.71 (0.28–1.78) | |
| Diverticula | ||
| No | 1 (reference) | <0.0001 |
| Yes | 3.86 (2.90–5.14) |
| Study | Study Design | N. Patients | Mean Age | Outcomes Assessed | Diagnosis | Association |
|---|---|---|---|---|---|---|
| McCallum A 1988 [35] | Retrospective | 119 | -- | Association between diverticulosis and CRC | Barium enema | no |
| Morini S 1988 [36] | Case-control study | 150 | 57.0 | Association between diverticular disease, adenomas, and CRC | Colonoscopy | Yes for adenomas No for CRC |
| Stefansson T 1993 [37] | Retrospective | 7159 | -- | Association between diverticulosis or diverticulitis and CRC | Nationwide register | Two-fold increase in the RR of left-sided CRC in patients with diverticulosis or diverticulitis. |
| Yusuf MA 2000 [38] a | Retrospective | 311 | 45.3 | Association between diverticular disease and CRC | Colonoscopy | no |
| Loffeld R.J 2002 [39] | Retrospective | 9086 | 52.0 without DD 69.0 with DD | Association between diverticulosis and CRC or polyps (histological type unspecified) | Colonoscopy | No for CRC yes for polyps |
| Morini S 2002 [26] | Prospective | 630 | 66.8 with DD 61.5 without DD | Association between diverticular disease, adenomas, and CRC | Colonoscopy | Yes for adenomas No for CRC |
| Stefansson T 2004 [40] | Retrospective | 7159 | -- | Association between sigmoid diverticulitis and increased risk of left-side CRC | Barium enema | yes |
| Kieff BJ 2004 [41] | Prospective | 502 | 58.6 | Association between diverticulosis and CRC | Colonoscopy CT scan surgery barium enema | Yes, only for women with extensive distal diverticulosis |
| Rajendra S 2005 [42] | Prospective | 410 | 51.7 | Association between diverticular disease and adenomas | Colonoscopy | yes |
| Soran A 2006 [43] | Retrospective | 1561 | 67.0 with DD and CRC 61.0 only with DD | Association between diverticulosis and CRC | Surgery | no |
| Krones CJ 2006 [44] | Retrospective | 1326 | 64.0 | Association between diverticulosis or diverticulitis and CRC | Surgery | no |
| Choi CS 2007 [45] | Retrospective | 2377 | 50.8 | Association between diverticulosis and CRC | Colonoscopy | yes |
| Rangnekar AS 2007 [46] a | Prospective | 308 | -- | Association of diverticulosis and polyps | Colonoscopy | yes |
| Hirata T 2008 [47] | Retrospective | 672 | 58.0 | Association between diverticular disease and colonic polyps | Colonoscopy | yes |
| Meurs-Szojda MM 2008 [30] | Retrospective | 4241 | 59.0 | Association of diverticulosis, diverticulitis, polyps, and CRC | Colonoscopy | no |
| Hammoud I 2009 [48] a | Retrospective | 1668 | -- | Association of diverticulosis and polyps | Colonoscopy | no |
| Lee KM 2010 [49] | Prospective | 1030 | 52.2 | Association of diverticulosis and polyps | Colonoscopy | yes |
| Mazumder MK 2011 [50] a | Retrospective | 1000 | 57.3 | Association of diverticulosis and polyps | Colonoscopy | yes |
| Neubauer K 2011 [51] a | Retrospective | 1776 | 52.5 | Association between diverticulosis and colorectal adenomas and CRC | Colonoscopy | Yes for adenomas No for CRC |
| Rondagh EJ 2011 [1] | Prospective | 2310 | 58.4 | Association between diverticulosis and colorectal polyps (adenoma, serrated polyp, advanced CRC) | Colonoscopy | yes |
| Grandlund J 2011 [31] | Retrospective | 41,037 | 75.0 F 73.0 M | Association between diverticular disease and CRC | CT-scan Colonoscopy | no |
| Szura M 2011 [52] a | Retrospective | 22,441 | 55.1 | Association of diverticulosis and polyps | Colonoscopy | yes |
| Gohil VB 2012 [28] | Retrospective | 300 | 57.0 | Association between diverticulosis and adenoma detection rate | Colonoscopy | yes |
| Lee SJ 2012 [53] | Prospective | 604 | 56.9 | Association of diverticulosis and CRC | CT-colonography | no |
| Azzam N 2013 [54] | Retrospective | 270 | 60.82 | Association among colonic polyps, comorbidities, and diverticular disease | Colonoscopy | Yes for diverticulosis and adenomas |
| Parava P 2013 [55] a | Retrospective | 1077 | 57.0 | Association of diverticulosis and polyps | Colonoscopy | yes |
| Muhammad A 2014 [29] | Retrospective | 2223 | 63.0 with DD 59.0 without DD | Association between diverticulosis and colorectal polyps (adenomas and advanced adenomas) | Colonoscopy | Yes for adenomas |
| Lecleire S 2014 [56] | Retrospective | 404 | 60.9 with DD 60.7 without DD | Association between acute diverticulitis and colorectal polyps | Colonoscopy | no |
| Meda S 2014 [57] a | Retrospective | 890 | -- | Association of diverticulosis and polyps | Colonoscopy | no |
| Shen H 2014 [58] a | Prospective | 1363 | 59.3 | Association of diverticulosis and adenomas | Colonoscopy | no |
| Huang WY 2014 [59] | Retrospective | 41,359 | 56.0 | Association between diverticulosis or diverticulitis and CRC | Colonoscopy | no |
| Ashktorab H 2015 [27] | Retrospective | 1986 | 57.0 | Association between diverticulosis and pre-neoplastic colonic lesions (hyperplastic polyps and adenomas) | Colonoscopy | yes |
| Peery AF 2015 [32] | Prospective | 624 | 56.0 with adenoma 53.0 without | Association between colonic diverticula and adenomas or advanced adenomas | Colonoscopy | no |
| Wang FW 2015 [60] | Prospective | 1899 | 52.8 | Association of diverticulosis and adenomas | Colonoscopy | yes |
| Wong ER 2016 [61] | Retrospective | 2766 | 53.2 | Association between colonic diverticula and CRC or polyps (not specified the histological type) | Colonoscopy | yes |
| Levine I 2017 [62] | Retrospective | 589 | 63 with D 58 without D | Association between colonic diverticula and CRC or polyps | Colonoscopy | no |
| Shah R 2017 [63] a | Retrospective | 896 | -- | Association of diverticulosis and polyps | Colonoscopy | yes |
| Teixeira C 2017 [64] | Prospective | 203 | 65.5 | Association of diverticulosis and adenomas | Colonoscopy | no |
| Hong W 2018 [65] | Prospective | 17,456 | 53.5 with D 49 without D | Association of diverticulosis or location of diverticulosis and adenoma or advanced adenoma | Colonoscopy | no |
| Pavão Borges V 2018 [66] a | Retrospective | 414 | 67.2 | Association of diverticulosis and adenomas | Colonoscopy | no |
| Rodriguez-Castro K 2018 [67] a | Prospective | 25,962 | 67.2 with D 58.1 without D | Association between colonic diverticula and CRC or polyps | Colonoscopy | Yes for adenomas No for CRC |
| Schramm C 2018 [68] | Retrospective | 4196 | 65.6 with D 62.0 without D | Association between colonic diverticula and CRC or polyps | Colonoscopy | Yes for adenomas No for CRC |
| Wang SF 2019 [69] | Retrospective | 346,118 | 56 | Association between colonic diverticula and CRC or polyps | Colonoscopy | yes |
| Tomaoglu K 2020 [70] | Retrospective | 3496 | 51.3 M 53.3 F | Association between diverticulosis and CRC or polyps | Colonoscopy | Yes for adenomas No for CRC |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viscido, A.; Ciccone, F.; Vernia, F.; Gabrieli, D.; Capannolo, A.; Stefanelli, G.; Necozione, S.; Valerii, G.; Ashktorab, H.; Latella, G. Association of Colonic Diverticula with Colorectal Adenomas and Cancer. Medicina 2021, 57, 108. https://doi.org/10.3390/medicina57020108
Viscido A, Ciccone F, Vernia F, Gabrieli D, Capannolo A, Stefanelli G, Necozione S, Valerii G, Ashktorab H, Latella G. Association of Colonic Diverticula with Colorectal Adenomas and Cancer. Medicina. 2021; 57(2):108. https://doi.org/10.3390/medicina57020108
Chicago/Turabian StyleViscido, Angelo, Fabiana Ciccone, Filippo Vernia, Dolores Gabrieli, Annalisa Capannolo, Gianpiero Stefanelli, Stefano Necozione, Giorgio Valerii, Hassan Ashktorab, and Giovanni Latella. 2021. "Association of Colonic Diverticula with Colorectal Adenomas and Cancer" Medicina 57, no. 2: 108. https://doi.org/10.3390/medicina57020108