
The Role of New Technologies to Prevent Suicide in Adolescence: A Systematic Review of the Literature


Abstract
:1. Introduction
2. Materials and Methods
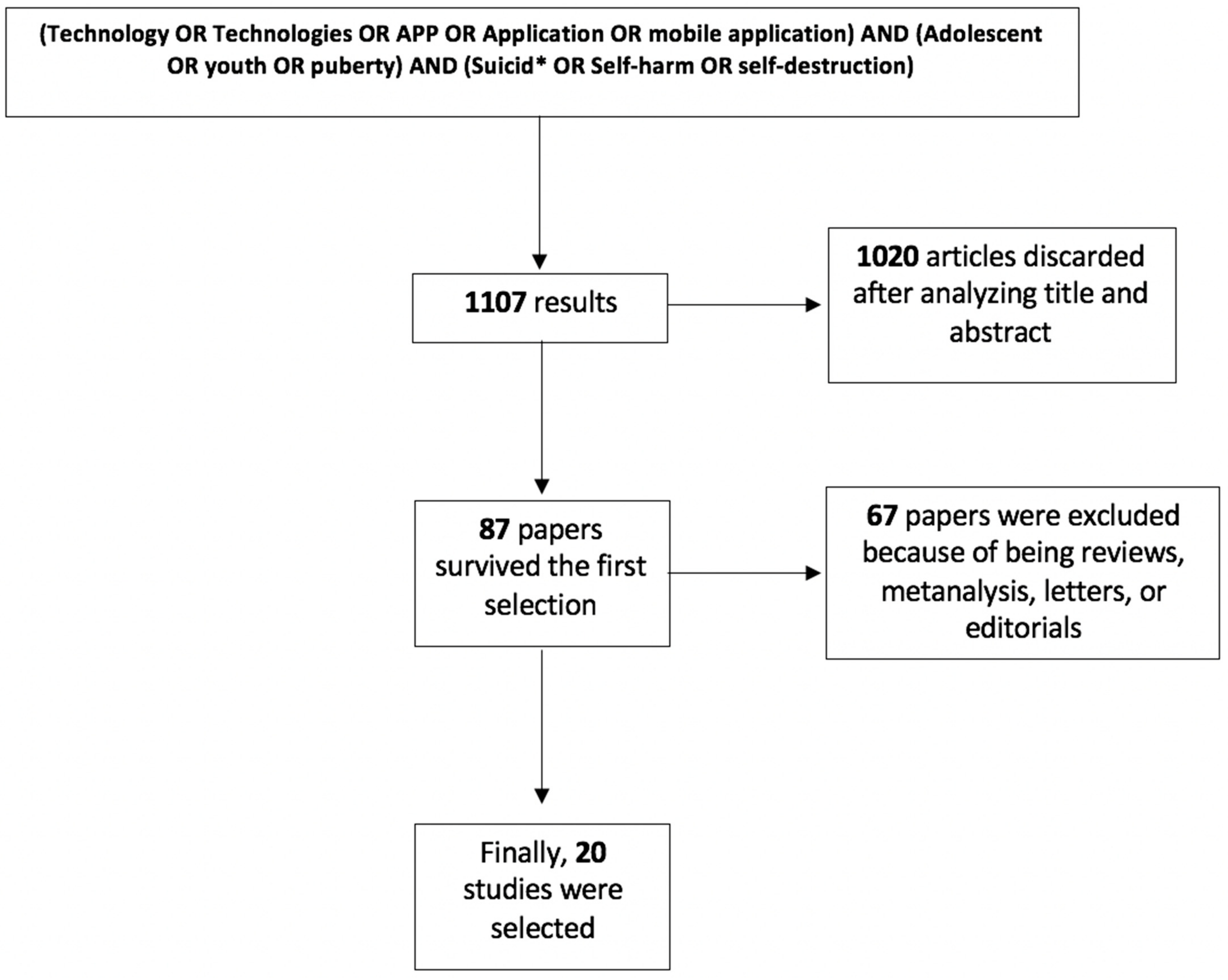
2.1. Search Strategy and Information Sources
2.2. Study Selection
2.3. Data Extraction
2.4. Risk of Bias within Studies
3. Results
3.1. Studies’ Selection, Characteristics and Limitations
3.2. Telepsychiatry
3.3. Mobile Health Interventions
3.4. Language Detection
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Hedegaard, H.; Curtin, S.C.; Warner, M. Suicide Mortality in the United States, 1999–2017; NCHS Data Brief; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2018; pp. 1–8. [Google Scholar]
- Hedegaard, H.; Curtin, S.C.; Warner, M. Suicide Rates in the United States Continue to Increase; NCHS Data Brief; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2018; pp. 1–8. [Google Scholar]
- Merikangas, K.R.; He, J.P.; Burstein, M.; Swanson, S.A.; Avenevoli, S.; Cui, L.; Swendsen, J. Lifetime prevalence of mental disorders in U.S. adolescents: Results from the national comorbidity survey replication-adolescent supplement (NCS-A). J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 980–989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gore, F.M.; Bloem, P.J.N.; Patton, G.C.; Ferguson, J.; Joseph, V.; Coffey, C.; Mathers, C.D. Global burden of disease in young people aged 10–24 years: A systematic analysis. Lancet 2011, 377, 2093–2102. [Google Scholar] [CrossRef]
- WHO. Causes of death among adolescents. In WHO Global Health Estimates; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- WHO. Preventing Suicide: A Global Imperative; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Geoffroy, M.C.; Orri, M.; Girard, A.; Perret, L.C.; Turecki, G. Trajectories of suicide attempts from early adolescence to emerging adulthood: Prospective 11-year follow-up of a Canadian cohort. Psychol Med. 2020. [Google Scholar] [CrossRef]
- Turecki, G.; Brent, D.A.; Gunnell, D.; O’Connor, R.C.; Oquendo, M.A.; Pirkis, J.; Stanley, B.H. Suicide and suicide risk. Nat. Rev. Dis. Prim. 2019, 5. [Google Scholar] [CrossRef]
- American Psychiatric Association. What is Telepsychiatry? American Psychiatric Association: Washington, DC, USA, 2020. [Google Scholar]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar]
- WHO. Coronavirus Disease 2019 (COVID-19) Situation Report—70. 2020; WHO: Geneva, Switzerland, 2020. [Google Scholar] [CrossRef]
- Pompili, M. Suicide Prevention at the Time of COVID-19. The BMJ Opinion, 10 September 2020. [Google Scholar]
- Faurholt-Jepsen, M.; Frost, M.; Christensen, E.M.; Bardram, J.E.; Vinberg, M.; Kessing, L.V. The effect of smartphone-based monitoring on illness activity in bipolar disorder: The MONARCA II randomized controlled single-blinded trial. Psychol. Med. 2020, 50, 838–848. [Google Scholar] [CrossRef]
- Faurholt-Jepsen, M.; Torri, E.; Cobo, J.; Yazdanyar, D.; Palao, D.; Cardoner, N.; Andreatta, O.; Mayora, O.; Kessing, L.V. Smartphone-based self-monitoring in bipolar disorder: Evaluation of usability and feasibility of two systems. Int. J. Bipolar. Disord. 2019, 7. [Google Scholar] [CrossRef] [PubMed]
- Svendsen, S.D.; Aggestrup, A.S.; Nørregaard, L.B.; Løventoft, P.; Præstegaard, A.; Danilenko, K.V.; Frost, M.; Knorr, U.; Hageman, I.; Kessing, L.V.; et al. Circadian reinforcement therapy in combination with electronic self-monitoring to facilitate a safe post-discharge period of patients with depression by stabilizing sleep: Protocol of a randomized controlled trial. BMC Psychiatry 2019, 19. [Google Scholar] [CrossRef] [Green Version]
- Ramalho, R.; Adiukwu, F.; Gashi Bytyçi, D.; El Hayek, S.; Gonzalez-Diaz, J.M.; Larnaout, A.; Grandinetti, P.; Nofal, M.; Pereira-Sanchez, V.; Pinto da Costa, M.; et al. Telepsychiatry During the COVID-19 Pandemic: Development of a Protocol for Telemental Health Care. Front. Psychiatry 2019, 11, 999. [Google Scholar]
- Roberts, L.W.; Chan, S.; Torous, J. New tests, new tools: Mobile and connected technologies in advancing psychiatric diagnosis. NPJ Digit. Med. 2018, 1, 1–4. [Google Scholar] [CrossRef]
- Lenhart, A. Teens, Social Media & Technology Overview; Pew Research Center: Washington, DC, USA, 2015. [Google Scholar]
- Witt, K.; Spittal, M.J.; Carter, G.; Pirkis, J.; Hetrick, S.; Currier, D.; Robinson, J.; Milner, A. Effectiveness of online and mobile telephone applications ('apps’) for the self-management of suicidal ideation and self-harm: A systematic review and meta-analysis. BMC Psychiatry 2017, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis JP, A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The age of adolescence. Lancet Child. Adolesc. Health 2018. [Google Scholar] [CrossRef]
- National Heart Lung and Blood Institute: National Institutes of Health. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies; National Institutes of Health: Bethesda, MA, USA, 2019. [Google Scholar]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 2016, 6. [Google Scholar] [CrossRef] [Green Version]
- Franklin, J.C.; Fox, K.R.; Franklin, C.R.; Kleiman, E.M.; Ribeiro, J.D.; Jaroszewski, A.C.; Hooley, J.M.; Nock, M.K. A brief mobile app reduces nonsuicidal and suicidal self-injury: Evidence from three randomized controlled trials. J. Consult. Clin. Psychol. 2016, 84, 544–557. [Google Scholar] [CrossRef] [PubMed]
- Hill, R.M.; Pettit, J.W. Pilot Randomized Controlled Trial of LEAP: A Selective Preventive Intervention to Reduce Adolescents’ Perceived Burdensomeness. J. Clin. Child Adolesc. Psychol. 2019, 48, S45–S56. [Google Scholar] [CrossRef]
- Bailey, E.; Alvarez-Jimenez, M.; Robinson, J.; D’Alfonso, S.; Nedeljkovic, M.; Davey, C.G.; Bendall, S.; Gilbertson, T.; Phillips, J.; Bloom, L. An enhanced social networking intervention for young people with active suicidal ideation: Safety, feasibility and acceptability outcomes. Int. J. Environ. Res. Public Health 2020, 17, 2435. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.Y.; Feltes, J.R.; Tzeng, W.S.; Lu, Z.Y.; Pan, M.; Zhao, N.; Talkin, R.; Javaherian, K.; Glowinski, A.; Ross, W. Phone-Based Interventions in Adolescent Psychiatry: A Perspective and Proof of Concept Pilot Study with a Focus on Depression and Autism. JMIR Res. Protoc. 2017, 6, e114. [Google Scholar] [CrossRef]
- Robinson, J.; Hetrick, S.; Cox, G.; Bendall, S.; Yuen, H.P.; Yung, A.; Pirkis, J. Can an Internet-based intervention reduce suicidal ideation, depression and hopelessness among secondary school students: Results from a pilot study. Early Interv. Psychiatry 2016, 10, 28–35. [Google Scholar] [CrossRef]
- Runkle, J.D.; Michael, K.D.; Stevens, S.E.; Sugg, M.M. Quasi-experimental evaluation of text-based crisis patterns in youth following Hurricane Florence in the Carolinas, 2018. Sci. Total Environ. 2021, 750. [Google Scholar] [CrossRef]
- Dickter, B.; Bunge, E.L.; Brown, L.M.; Leykin, Y.; Soares, E.E.; Van Voorhees, B.; Marko-Holguin, M.; Gladstone, T.R.G. Impact of an online depression prevention intervention on suicide risk factors for adolescents and young adults. mHealth 2019, 5, 11. [Google Scholar] [CrossRef] [PubMed]
- Grist, R.; Porter, J.; Stallard, P. Acceptability, Use, and Safety of a Mobile Phone App (BlueIce) for Young People Who Self-Harm: Qualitative Study of Service Users’ Experience. JMIR Ment. Health 2018, 5, e16. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Torok, M.; Gale, N.; Wong, Q.J.; Werner-Seidler, A.; Hetrick, S.E.; Christensen, H. Use of web conferencing technology for conducting online focus groups among young people with lived experience of suicidal thoughts: Mixed methods research. J. Med. Internet Res. 2019, 21, e14191. [Google Scholar] [CrossRef] [PubMed]
- Hetrick, S.E.; Robinson, J.; Burge, E.; Blandon, R.; Mobilio, B.; Rice, S.M.; Simmons, M.B.; Alvarez-Jimenez, M.; Goodrich, S.; Davey, C.G. Youth codesign of a mobile phone app to facilitate self-monitoring and management of mood symptoms in young eople with major depression, suicidal ideation, and self-harm. J. Med. Internet Res. 2018, 20. [Google Scholar] [CrossRef]
- McManama O’Brien, K.H.; LeCloux, M.; Ross, A.; Gironda, C.; Wharff, E.A. A Pilot Study of the Acceptability and Usability of a Smartphone Application Intervention for Suicidal Adolescents and Their Parents. Arch. Suicide Res. 2017, 21, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Milton, A.C.; Gill, B.A.; Davenport, T.A.; Dowling, M.; Burns, J.M.; Hickie, I.B. Sexting, web-based risks, and safety in two representative national samples of young Australians: Prevalence, perspectives, and predictors. J. Med Internet Res. 2019, 21, e13338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ospina-Pinillos, L.; Davenport, T.; Iorfino, F.; Tickell, A.; Cross, S.; Scott, E.M.; Hickie, I.B. Using new and innovative technologies to assess clinical stage in early intervention youth mental health services: Evaluation study. J. Med. Internet Res. 2018, 20, e259. [Google Scholar] [CrossRef]
- Owens, C.; Charles, N. Implementation of a text-messaging intervention for adolescents who self-harm (TeenTEXT): A feasibility study using normalisation process theory. Child Adolesc. Psychiatry Ment. Health 2016, 10, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennard, B.D.; Goldstein, T.; Foxwell, A.A.; McMakin, D.L.; Wolfe, K.; Biernesser, C.; Moorehead, A.; Douaihy, A.; Zullo, L.; Wentroble, E.; et al. As safe as possible (ASAP): A brief app-supported inpatient intervention to prevent postdischarge suicidal behavior in Hospitalized, Suicidal Adolescents. Am. J. Psychiatry 2018, 175, 864–872. [Google Scholar] [CrossRef]
- Thabrew, H.; D’Silva, S.; Darragh, M.; Goldfinch, M.; Meads, J.; Goodyear-Smith, F. Comparison of YouthCHAT, an electronic composite psychosocial screener, with a clinician interview assessment for young people: Randomized controlled trial. J. Med. Internet Res. 2019, 21, e13911. [Google Scholar] [CrossRef] [Green Version]
- Aladağ, A.E.; Muderrisoglu, S.; Akbas, N.B.; Zahmacioglu, O.; Bingol, H.O. Detecting suicidal ideation on forums: Proof-of-concept study. J. Med. Internet Res. 2018, 20. [Google Scholar] [CrossRef]
- Brown, R.C.; Bendig, E.; Fischer, T.; Goldwich, A.D.; Baumeister, H.; Plener, P.L. Can acute suicidality be predicted by Instagram data? Results from qualitative and quantitative language analyses. PLoS ONE 2019, 14. [Google Scholar] [CrossRef] [PubMed]
- Downs, J.; Velupillai, S.; George, G.; Holden, R.; Kikoler, M.; Dean, H.; Fernandes, A.; Dutta, R. Detection of Suicidality in Adolescents with Autism Spectrum Disorders: Developing a Natural Language Processing Approach for Use in Electronic Health Records. In Proceedings of the AMIA Annual Symposium Proceedings, Washington, DC, USA, 4–8 November 2017; pp. 641–649. [Google Scholar]
- Grant, R.N.; Kucher, D.; León, A.M.; Gemmell, J.F.; Raicu, D.S.; Fodeh, S.J. Automatic extraction of informal topics from online suicidal ideation. BMC Bioinform. 2018, 19, 57–66. [Google Scholar] [CrossRef]
- Pisani, A.R.; Murrie, D.C.; Silverman, M.M. Reformulating suicide risk formulation: From prediction to prevention. Acad. Psychiatry 2016, 40, 623–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lester, D.; Rogers, J.R. Crisis Intervention and Counseling by Telephone and the Internet, 3rd ed.; Charles C Thomas Publisher: Springfield, IL, USA, 2012. [Google Scholar]
- Muñoz, R.F.; Bunge, E.L.; Chen, K.; Schueller, S.M.; Bravin, J.I.; Shaughnessy, E.A.; Pérez-Stable, E.J. Massive Open Online Interventions. Clin. Psychol. Sci. 2016, 194–205. [Google Scholar]
- Kleiman, E.M.; Turner, B.J.; Fedor, S.; Beale, E.E.; Huffman, J.C.; Nock, M.K. Examination of real-time fluctuations in suicidal ideation and its risk factors: Results from two ecological momentary assessment studies. J. Abnorm. Psychol. 2017, 126, 726–738. [Google Scholar] [CrossRef]
- Forte, A.; Buscajoni, A.; Fiorillo, A.; Pompili, M.; Baldessarini, R.J. Suicidal Risk Following Hospital Discharge: A Review. Harv. Rev. Psychiatry 2019, 27, 209–216. [Google Scholar]
- Chung, D.T.; Ryan, C.J.; Hadzi-Pavlovic, D.; Singh, S.P.; Stanton, C.; Large, M.M. Suicide Rates After Discharge from Psychiatric Facilities. JAMA Psychiatry 2017, 74, 694. [Google Scholar] [CrossRef]
- Brent, D.A.; Greenhill, L.L.; Compton, S.; Emslie, G.; Wells, K.; Walkup, J.T.; Vitiello, B.; Bukstein, O.; Stanley, B.; Posner, K.; et al. The Treatment of Adolescent Suicide Attempters Study (TASA): Predictors of Suicidal Events in an Open Treatment Trial. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 987–996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, N.B.; Nelson, B.W.; Brent, D.; Auerbach, R.P. Short-term prediction of suicidal thoughts and behaviors in adolescents: Can recent developments in technology and computational science provide a breakthrough? J Affect Disord. 2019, 250, 163–169. [Google Scholar] [CrossRef]
- Coppersmith, G.; Leary, R.; Crutchley, P.; Fine, A. Natural Language Processing of Social Media as Screening for Suicide Risk. Biomed Inform. Insights 2018, 10, 117822261879286. [Google Scholar] [CrossRef] [PubMed]
- Trnka, R.; Lorencova, R. Fear, Anger, and Media-Induced Trauma During the Outbreak of COVID-19 in the Czech Republic. Psychol Trauma Theory. Res. Pract. Policy 2020, 12. [Google Scholar] [CrossRef]
- Robinson, J.; Bailey, E.; Witt, K.; Stefanac, N.; Milner, A.; Currier, D.; Pirkis, J.; Condron, P.; Hetrick, S. What Works in Youth Suicide Prevention? A Systematic Review and Meta-Analysis. EClinicalMedicine 2018, 4–5, 52–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pompili, M. The increase of suicide rates: The need for a paradigm shift. Lancet 2018, 392, 474–475. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Article | RCT | Method of Randomization | Treatment Allocation | Double Blinding | Power Calculation | Adherence | Continuous Exposure Variables | Times | Valid Outcome Measure | Drop-Out Rate |
|---|---|---|---|---|---|---|---|---|---|---|
| Aladag A.E. et al., 2018 | N | Y | NA | NA | NR | NA | Y | N | N | N |
| Bailey E. et al., 2020 | N | N | Y | N | Y | Y | Y | Y | Y | N |
| Brown R.C. et al., 2019 | N | N | NA | N | NR | Y | N | N | Y | N |
| Chen R.Y. et al., 2017 | N | N | Y | N | N | N | Y | N | Y | N |
| Dickter B. et al., 2019 | N | N | Y | N | N | Y | Y | Y | Y | N |
| Downs J. et al., 2017 | N | NA | NA | NA | N | NA | Y | N | Y | N |
| Franklin J. et al., 2016 | Y | Y | Y | N | N | Y | Y | N | Y | N |
| Grant R.N. et al., 2018 | N | N | N | N | NA | Y | Y | N | Y | NA |
| Grist R. et al., 2018 | N | N | NA | N | NR | Y | Y | Y | Y | Y |
| Han J. et al., 2019 | N | N | NA | N | N | Y | Y | N | Y | N |
| Hetrick S.E. et al., 2018 | N | N | NA | N | N | Y | Y | Y | Y | N |
| Hill R.M. et al., 2016 | Y | Y | Y | N | N | Y | Y | Y | Y | N |
| Kennard B.D. et al., 2018 | N | Y | Y | N | Y | Y | Y | Y | Y | Y |
| McManama O’Brien K.H. et al., 2016 | N | N | Y | N | N | N | N | N | N | N |
| Milton A.C. et al., 2019 | N | Y | NA | N | N | N | N | N | Y | N |
| Ospina-Pinillos et al., 2018 | N | Y | Y | NA | N | N | N | N | Y | NA |
| Owens C. et al., 2016 | N | N | NA | NA | N | NA | N | N | N | NA |
| Robinson J. et al., 2016 | N | N | N | N | N | Y | Y | Y | Y | Y |
| Runkle J.D. et al., 2020 | NA | NA | NA | NA | N | NA | N | Y | N | N |
| Thabrew H. et al., 2019 | Y | Y | Y | N | N | Y | Y | N | N | Y |
| Article | Technology | Type of Article | Gender (Female %) | N. Participants | Target Group | Age Range | Diagnosis | Outcome | Intervention |
|---|---|---|---|---|---|---|---|---|---|
| Aladag A.E. et al., 2018 | Language detection | Retrospective cohort study | / | 785 (posts) | General | / | / | Suicidality | Prevention (self-guided) |
| Bailey E. et al., 2020 | Telepsychiatry | Open-label single group trial | 55% | 20 | General | 16–25 (21.7 mean) | / | Feasibility, safety, acceptability and suicidal ideation | Prevention (self-guided/specialistic) |
| Brown R.C. et al., 2019 | Language detection | Retrospective cohort study | 87% | 52 | General | Mean age 16.6 | / | Suicidal thoughts, acute suicidality | Prevention (self-guided) |
| Chen R.Y. et al., 2017 | Telepsychiatry | Open-label single group trial | / | 9 | Clinical | adolescents | MDD,,break/>Autism Spectrum Disorders (ASD) | Response rate, suicidal behavior and ideation. | Prevention (self-guided) |
| Dickter B. et al., 2019 | Telepsychiatry | Open-label single group trial | 56.2 | 83 | Clinical | 14–21 | MDD | Suicidal ideation | Prevention (self-guided) |
| Downs J. et al., 2017 | Language detection | Retrospective cohort study | / | 1906 | Clinical | 14–18 | ASD | Suicidal ideation. | Postvention (self-guided) |
| Franklin J. et al., 2016 | APP | RCT | 80.7 | 114 | General | mean age 23.02 | / | Suicide plans and behavior. | Prevention (self-guided) |
| Grant R.N. et al., 2018 | Language detection | Retrospective cohort study | / | 63,252 (posts) | General | / | / | Latent topics related to suicide ideation. | Prevention (self-guided) |
| Grist R. et al., 2018 | APP | Open-label single group trial | 90 | 44 | Clinical | 12–17 | MDD, Anxiety disorder | Suicidal behavior | Prevention (self-guided) |
| Han J. et al., 2019 | Telepsychiatry | Open-label single group trial | 92.5 | 43 | General | 16–25 | / | Acceptability, suicidal ideation. | Postvention (specialist) |
| Hetrick S.E. et al., 2018 | APP | Open-label single group trial | 76.9 | 13 | Clinical | 18–25 | MDD | Mood monitoring, suicidal ideation. | Prevention (self-guided) |
| Hill R.M. et al., 2016 | Telepsychiatry | RCT | 68.8 | 80 | General | 13–19 | / | Perceived burdensomeness, thwarted belonginess, depressive symptoms | Prevention (specialist) |
| Kennard B.D. et al., 2018 | APP | Randomized study | 89.4 | 66 | Clinical | 12–18 | MDD, Anxiety disorder | Suicidal ideation, behavior, treatment utilization and satisfaction | Postvention (self-guided) |
| McManama O’Brien K.H. et al., 2016 | APP | Open-label single group trial | 80.7 | 20 | General | 13–18 | / | Acceptability, usability, suicidal ideation | Prevention (self-guided) |
| Milton A.C. et al., 2019 | Telepsychiatry | Open-label single group trial | 50 | 1400 | General | 16–25 | / | Sexting, suicidal thoughts and behavior. | Prevention (self-guided) |
| Ospina-Pinillos et al., 2018 | Telepsychiatry | Open-label single group trial | 71.6 | 204 | General | 16–25 | / | Online vs. face to face assessments | Postvention (specialist) |
| Owens C. et al., 2016 | Telepsychiatry | Open-label single group trial | / | 27 | General | 12–18 | / | Self-harming behaviors | Prevention (self-guided, specialist) |
| Robinson J. et al., 2016 | Telepsychiatry | Open-label single group trial | 87.5 | 32 | Clinical | 14–18 | MDD | Suicidal ideation, hopelessness and depression. | Prevention (self-guided, specialist) |
| Runkle J.D. et al., 2020 | Telepsychiatry | Open-label single group trial | / | 34.71 | General | 15–24 | / | Help-seeking patterns | Prevention (self-guided) |
| Thabrew H. et al., 2019 | Telepsychiatry | Randomized study | 49 | 110 | General | 13–14 | / | Completion times, detection rates, acceptability | Prevention (self-guided) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forte, A.; Sarli, G.; Polidori, L.; Lester, D.; Pompili, M. The Role of New Technologies to Prevent Suicide in Adolescence: A Systematic Review of the Literature. Medicina 2021, 57, 109. https://doi.org/10.3390/medicina57020109
Forte A, Sarli G, Polidori L, Lester D, Pompili M. The Role of New Technologies to Prevent Suicide in Adolescence: A Systematic Review of the Literature. Medicina. 2021; 57(2):109. https://doi.org/10.3390/medicina57020109
Chicago/Turabian StyleForte, Alberto, Giuseppe Sarli, Lorenzo Polidori, David Lester, and Maurizio Pompili. 2021. "The Role of New Technologies to Prevent Suicide in Adolescence: A Systematic Review of the Literature" Medicina 57, no. 2: 109. https://doi.org/10.3390/medicina57020109