
Long-Term Pain Characteristics and Management Following Minimally Invasive Spinal Decompression and Open Laminectomy and Fusion for Spinal Stenosis

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Surgical Technique
2.2. Statistical Analysis
3. Results
3.1. Back and Leg Pain Intensity and Frequency
3.2. Use of Pain Medication
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Disease, G.B.D.; Injury, I.; Prevalence, C. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Deyo, R.A.; Mirza, S.K.; Martin, B.I.; Kreuter, W.; Goodman, D.C.; Jarvik, J.G. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA 2010, 303, 1259–1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajaee, S.S.; Bae, H.W.; Kanim, L.E.; Delamarter, R.B. Spinal fusion in the United States: Analysis of trends from 1998 to 2008. Spine 2012, 37, 67–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herkowitz, H.N. Lumbar spinal stenosis: Indications for arthrodesis and spinal instrumentation. Instr. Course Lect. 1994, 43, 425–433. [Google Scholar] [PubMed]
- Lad, S.P.; Babu, R.; Ugiliweneza, B.; Patil, C.G.; Boakye, M. Surgery for spinal stenosis: Long-term reoperation rates, health care cost, and impact of instrumentation. Spine 2014, 39, 978–987. [Google Scholar] [CrossRef] [PubMed]
- Forsth, P.; Olafsson, G.; Carlsson, T.; Frost, A.; Borgstrom, F.; Fritzell, P.; Ohagen, P.; Michaelsson, K.; Sanden, B. A Randomized, Controlled Trial of Fusion Surgery for Lumbar Spinal Stenosis. N. Engl. J. Med. 2016, 374, 1413–1423. [Google Scholar] [CrossRef] [PubMed]
- Thomas, K.; Faris, P.; McIntosh, G.; Manners, S.; Abraham, E.; Bailey, C.S.; Paquet, J.; Cadotte, D.; Jacobs, W.B.; Rampersaud, Y.R.; et al. Decompression alone vs. decompression plus fusion for claudication secondary to lumbar spinal stenosis. Spine J. 2019, 19, 1633–1639. [Google Scholar] [CrossRef]
- Zigler, J.E.; Delamarter, R.B. Does 360 degrees lumbar spinal fusion improve long-term clinical outcomes after failure of conservative treatment in patients with functionally disabling single-level degenerative lumbar disc disease? Results of 5-year follow-up in 75 postoperative patients. Int. J. Spine Surg. 2013, 7, e1–e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alimi, M.; Hofstetter, C.P.; Pyo, S.Y.; Paulo, D.; Hartl, R. Minimally invasive laminectomy for lumbar spinal stenosis in patients with and without preoperative spondylolisthesis: Clinical outcome and reoperation rates. J. Neurosurg. Spine 2015, 22, 339–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, W.S.; Oh, C.H.; Ji, G.Y.; Shin, S.C.; Lee, J.B.; Park, D.H.; Cho, T.H. Spinal canal morphology and clinical outcomes of microsurgical bilateral decompression via a unilateral approach for lumbar spinal canal stenosis. Eur. Spine J. 2014, 23, 991–998. [Google Scholar] [CrossRef] [PubMed]
- Sasai, K.; Umeda, M.; Maruyama, T.; Wakabayashi, E.; Iida, H. Microsurgical bilateral decompression via a unilateral approach for lumbar spinal canal stenosis including degenerative spondylolisthesis. J. Neurosurg. Spine 2008, 9, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Khoo, L.T.; Fessler, R.G. Microendoscopic decompressive laminotomy for the treatment of lumbar stenosis. Neurosurgery 2002, 51, S146–S154. [Google Scholar] [CrossRef] [PubMed]
- Musluman, A.M.; Cansever, T.; Yilmaz, A.; Cavusoglu, H.; Yuce, I.; Aydin, Y. Midterm outcome after a microsurgical unilateral approach for bilateral decompression of lumbar degenerative spondylolisthesis. J. Neurosurg. Spine 2012, 16, 68–76. [Google Scholar] [CrossRef]
- Rahman, M.; Summers, L.E.; Richter, B.; Mimran, R.I.; Jacob, R.P. Comparison of techniques for decompressive lumbar laminectomy: The minimally invasive versus the “classic” open approach. Minim. Invasive Neurosurg. 2008, 51, 100–105. [Google Scholar] [CrossRef]
- Edelen, M.O.; Saliba, D. Correspondence of verbal descriptor and numeric rating scales for pain intensity: An item response theory calibration. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 778–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teno, J.M.; Weitzen, S.; Wetle, T.; Mor, V. Persistent pain in nursing home residents. JAMA 2001, 285, 2081. [Google Scholar] [CrossRef]
- Won, A.; Lapane, K.L.; Vallow, S.; Schein, J.; Morris, J.N.; Lipsitz, L.A. Long-term effects of analgesics in a population of elderly nursing home residents with persistent nonmalignant pain. J. Gerontol. A. Biol. Sci. Med. Sci. 2006, 61, 165–169. [Google Scholar] [CrossRef] [Green Version]
- Garfin, S.R.; Herkowitz, H.N.; Mirkovic, S. Spinal stenosis. Instr. Course Lect. 2000, 49, 361–374. [Google Scholar] [PubMed]
- Theodoridis, T.; Kramer, J.; Kleinert, H. Conservative treatment of lumbar spinal stenosis—A review. Z. Orthop. Unfall. 2008, 146, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.N.; Lipson, S.J.; Larson, M.G.; McInnes, J.M.; Fossel, A.H.; Liang, M.H. The outcome of decompressive laminectomy for degenerative lumbar stenosis. J. Bone Joint Surg. Am. 1991, 73, 809–816. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.N.; Jacquot, F.; Hall, H. Long-term follow-up of functional outcomes and radiographic changes at adjacent levels following lumbar spine fusion for degenerative disc disease. Eur. Spine J. 2001, 10, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Mobbs, R.J.; Li, J.; Sivabalan, P.; Raley, D.; Rao, P.J. Outcomes after decompressive laminectomy for lumbar spinal stenosis: Comparison between minimally invasive unilateral laminectomy for bilateral decompression and open laminectomy: Clinical article. J. Neurosurg. Spine 2014, 21, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Kelleher, M.O.; Timlin, M.; Persaud, O.; Rampersaud, Y.R. Success and failure of minimally invasive decompression for focal lumbar spinal stenosis in patients with and without deformity. Spine 2010, 35, E981–E987. [Google Scholar] [CrossRef]
- Toyoda, H.; Nakamura, H.; Konishi, S.; Dohzono, S.; Kato, M.; Matsuda, H. Clinical outcome of microsurgical bilateral decompression via unilateral approach for lumbar canal stenosis: Minimum five-year follow-up. Spine 2011, 36, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, K.; Ohzono, K.; Hiroshima, K. Five-year outcomes of surgical treatment for degenerative lumbar spinal stenosis: A prospective observational study of symptom severity at standard intervals after surgery. Spine 2006, 31, 1484–1490. [Google Scholar] [CrossRef]
- Chaudhary, M.A.; Bhulani, N.; de Jager, E.C.; Lipsitz, S.; Kwon, N.K.; Sturgeon, D.J.; Trinh, Q.D.; Koehlmoos, T.; Haider, A.H.; Schoenfeld, A.J. Development and Validation of a Bedside Risk Assessment for Sustained Prescription Opioid Use After Surgery. JAMA Netw. Open 2019, 2, e196673. [Google Scholar] [CrossRef] [PubMed]
- Karhade, A.V.; Cha, T.D.; Fogel, H.A.; Hershman, S.H.; Tobert, D.G.; Schoenfeld, A.J.; Bono, C.M.; Schwab, J.H. Predicting prolonged opioid prescriptions in opioid-naive lumbar spine surgery patients. Spine J. 2019. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, A.J.; Belmont, P.J., Jr.; Blucher, J.A.; Jiang, W.; Chaudhary, M.A.; Koehlmoos, T.; Kang, J.D.; Haider, A.H. Sustained Preoperative Opioid Use Is a Predictor of Continued Use Following Spine Surgery. J. Bone Joint Surg. Am. 2018, 100, 914–921. [Google Scholar] [CrossRef]
- Schoenfeld, A.J.; Nwosu, K.; Jiang, W.; Yau, A.L.; Chaudhary, M.A.; Scully, R.E.; Koehlmoos, T.; Kang, J.D.; Haider, A.H. Risk Factors for Prolonged Opioid Use Following Spine Surgery, and the Association with Surgical Intensity, Among Opioid-Naive Patients. J. Bone Joint Surg. Am. 2017, 99, 1247–1252. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MIS Decompression Group | Fusion Group | p-Value | |
|---|---|---|---|
| Age (years) * | 69.88 ± 11.7 | 63.6 ± 13 | 0.0092 |
| Male/female | 22/28 | 15/30 | 0.4 |
| Follow-up (years) | 7.82 ± 0.25 | 5.89 ± 0.09 | >0.001 |
| L2-3 | 3 (6%) | 0 | 0.05 |
| L3-4 | 15 (30%) | 10 (21.7%) | 0.5 |
| L4-5 | 34 (68%) | 30 (65.2%) | 0.8 |
| L5-S1 | 3 (6%) | 18 (39.1%) | 0.2 |
| Degenerative spondylolisthesis | 9 (18%) | 8 (17.8%) | 0.8 |
| One-level surgery | 47 (90.4%) | 33 (71.7%) | 0.7 |
| Two-level surgery | 5 (9.6%) | 13 (28.3%) | 0.3 |
| Reoperation and other lumbar spine surgeries | 11 (22%) | 13 (29%) | 0.65 |
| Surgery Type | p-Value | |||
|---|---|---|---|---|
| MIS Decompression Group (n = 46) | Fusion Group (n = 50) | |||
| Back pain | None | 19 (41.3%) | 9 (18%) | 0.0029 |
| Mild | 17 (37%) | 17 (34%) | ||
| Moderate | 9 (19.6%) | 12 (24%) | ||
| Severe | 1 (2.2%) | 12 (24%) | ||
| Leg pain | None | 13 (28.3%) | 12 (24%) | 0.3116 |
| Mild | 13 (28.3%) | 12 (24%) | ||
| Moderate | 15 (32.6%) | 13 (26%) | ||
| Severe | 5 (10.9%) | 13 (26%) | ||
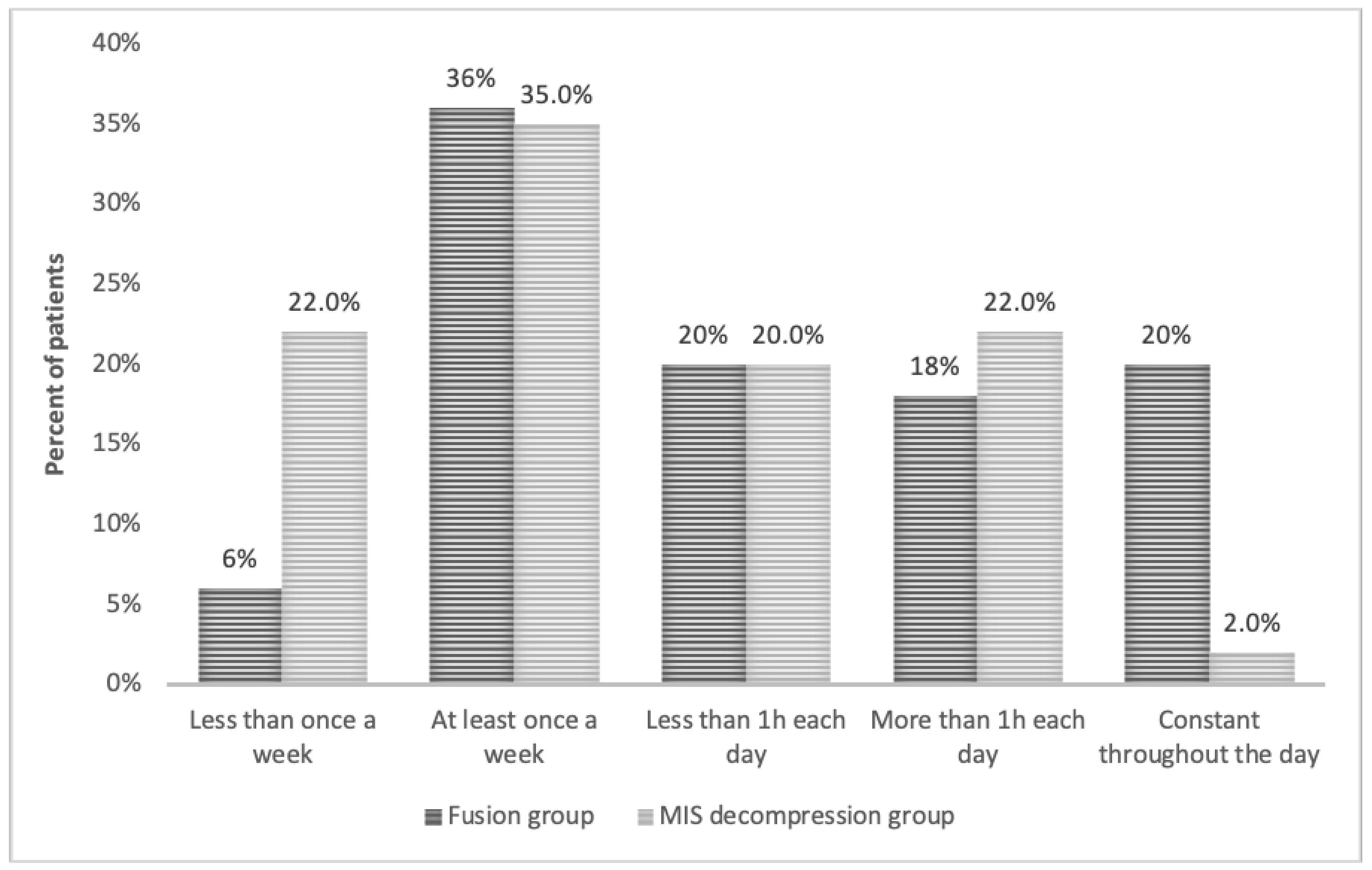
| Pain frequency | Less than once a week | 10 (21.7%) | 3 (6%) | 0.0203 |
| At least once a week | 16 (34.8%) | 18 (36%) | ||
| Less than 1 h each day | 9 (19.6%) | 10 (20%) | ||
| More than 1 h each day | 10 (21.7%) | 9 (18%) | ||
| Constant | 1 (2.2%) | 10 (20%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Regev, G.J.; Leor, G.; Ankori, R.; Hochberg, U.; Ofir, D.; Khashan, M.; Kedem, R.; Lidar, Z.; Salame, K. Long-Term Pain Characteristics and Management Following Minimally Invasive Spinal Decompression and Open Laminectomy and Fusion for Spinal Stenosis. Medicina 2021, 57, 1125. https://doi.org/10.3390/medicina57101125
Regev GJ, Leor G, Ankori R, Hochberg U, Ofir D, Khashan M, Kedem R, Lidar Z, Salame K. Long-Term Pain Characteristics and Management Following Minimally Invasive Spinal Decompression and Open Laminectomy and Fusion for Spinal Stenosis. Medicina. 2021; 57(10):1125. https://doi.org/10.3390/medicina57101125
Chicago/Turabian StyleRegev, Gilad J., Gil Leor, Ran Ankori, Uri Hochberg, Dror Ofir, Morsi Khashan, Ron Kedem, Zvi Lidar, and Khalil Salame. 2021. "Long-Term Pain Characteristics and Management Following Minimally Invasive Spinal Decompression and Open Laminectomy and Fusion for Spinal Stenosis" Medicina 57, no. 10: 1125. https://doi.org/10.3390/medicina57101125