
Patients’ Perception of Recovery after Dental Implant Placement

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
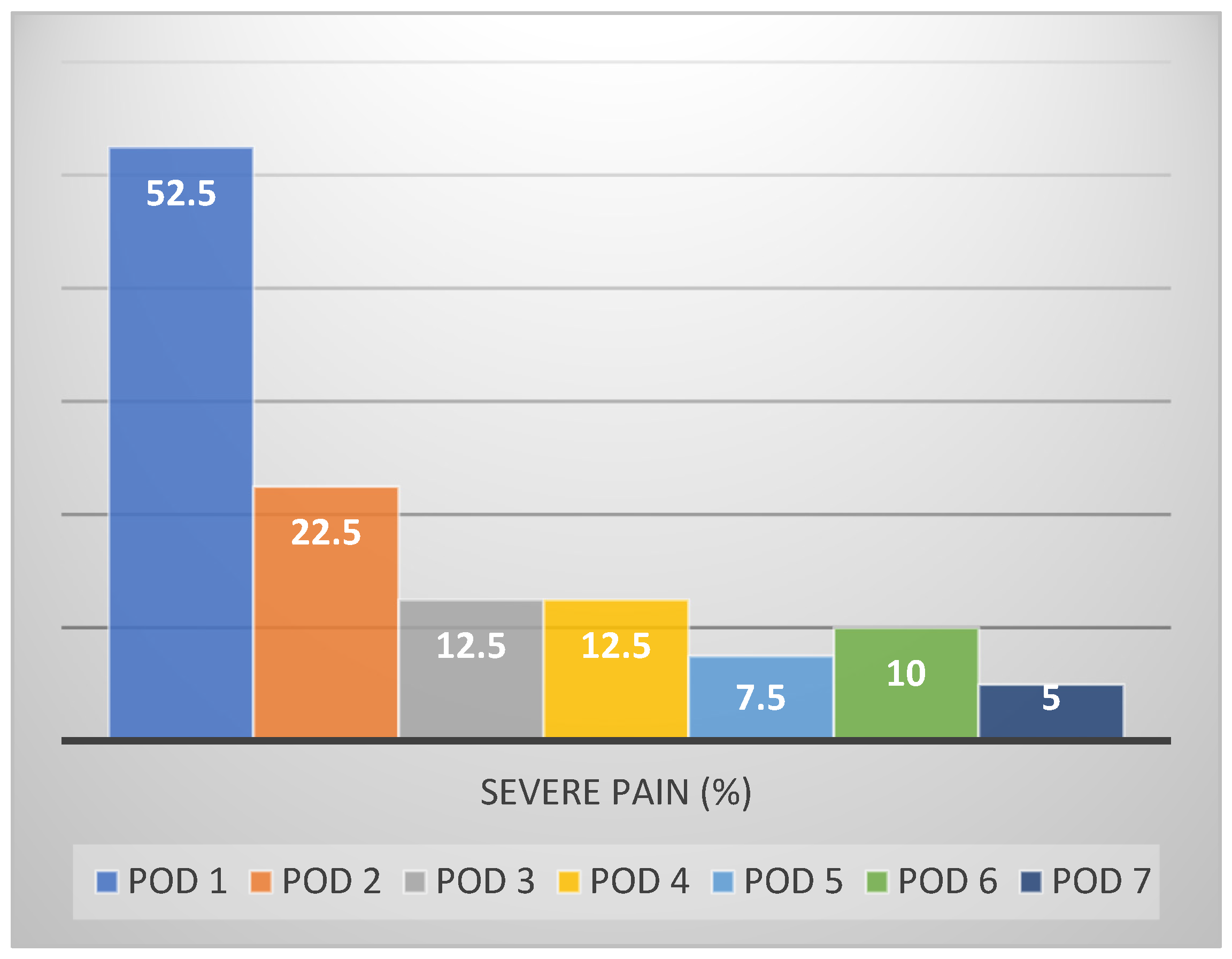
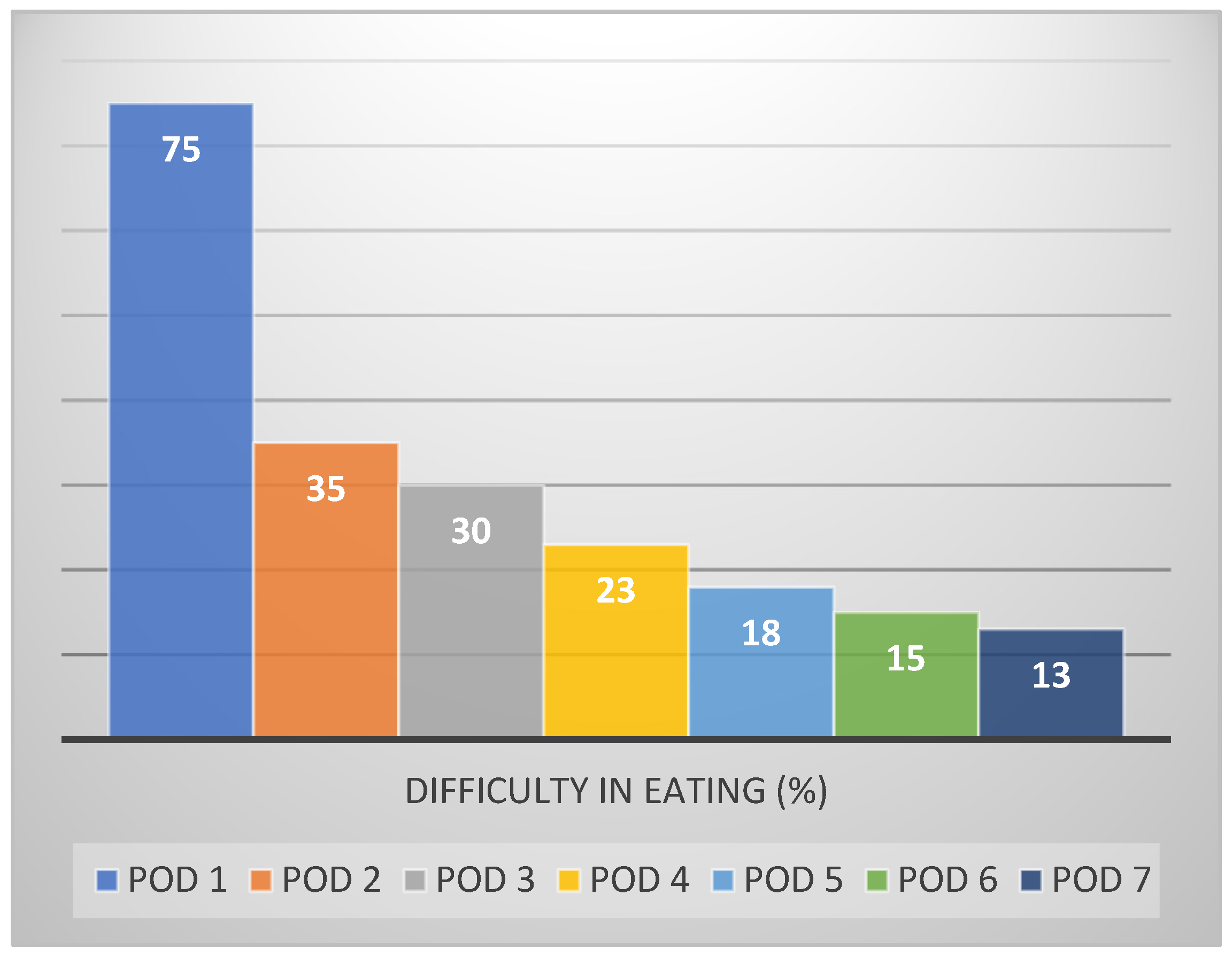
3. Results
4. Discussion
5. Conclusions
- Patients should expect, in general, recovery within 4 days after dental implant placement.
- Women will experience a delayed recovery.
- Implants placed in the intercanine area will result in postoperative eating difficulties for nearly one week.
- The number of implants placed during the same appointment has no effect on post treatment recovery.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Messias, A.; Nicolau, P.; Guerra, F. Different interventions for rehabilitation of the edentulous maxilla with implant-supported prostheses: An overview of systematic reviews. Int. J. Prosthodont. 2021, 34, s63–s84. [Google Scholar] [CrossRef]
- Karasan, D.; Fehmer, V.; Ligoutsikou, M.; Srinivasan, M.; Sailer, I. The influence of patient-related factors and material selection on the clinical outcomes of fixed and removable complete implant prostheses: An overview on systematic reviews. Int. J. Prosthodont. 2021, 34, s46–s62. [Google Scholar] [CrossRef]
- Fretwurst, T.; Nelson, K. Influence of medical and geriatric factors on implant success: An overview of systematic reviews. Int. J. Prosthodont. 2021, 34, s21–s26. [Google Scholar] [CrossRef]
- Albrektsson, T.; Wennerberg, A. On osseointegration in relation to implant surfaces. Clin. Implant Dent. Relat. Res. 2019, 21, 4–7. [Google Scholar] [CrossRef] [Green Version]
- Albrektsson, T.; Zarb, G.A. Current interpretations of the osseointegrated response: Clinical significance. Int. J. Prosthodont. 1993, 2, 95–105. [Google Scholar]
- Adell, R.; Lekholm, U.; Rockler, B.; Brånemark, P.I. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int. J. Oral Surg. 1981, 6, 387–416. [Google Scholar] [CrossRef]
- Al-Khabbaz, A.K.; Griffin, T.J.; Al-Shammari, K.F. Assessment of pain associated with the surgical placement of dental implants. J. Periodontol. 2007, 78, 239–246. [Google Scholar] [CrossRef] [PubMed]
- González-Santana, H.; Peñarrocha-Diago, M.; Guarinos-Carbó, J.; Balaguer-Martínez, J. Pain and inflammation in 41 patients following the placement of 131 dental implants. Med. Oral Patol. Oral Cir. Bucal 2005, 10, 258–263. [Google Scholar] [PubMed]
- Hashem, A.A.; Claffey, N.M.; O’Connell, B. Pain and anxiety following the placement of dental implants. Int. J. Oral Maxillofac. Implant. 2006, 21, 943–950. [Google Scholar]
- Urban, T.; Wenzel, A. Discomfort experienced after immediate implant placement associated with three different regenerative techniques. Clin. Oral Implants Res. 2010, 21, 1271–1277. [Google Scholar] [CrossRef]
- Eli, I.; Schwartz-Arad, D.; Baht, R.; Ben-Tuvim, H. Effect of anxiety on the experience of pain in implant insertion. Clin. Oral Implant. Res. 2003, 14, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Lee, Y.J.; Lee, S.; Moon, H.S.; Chung, M.K. Assessment of pain and anxiety following surgical placement of dental implants. Int. J. Oral Maxillofac. Implant. 2013, 28, 531–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabrizi, R.; Mohajerani, H.; Nabtieh, A.; Shafiei, S. Do patients have the same experience of pain following tooth extraction and dental implants? Ann. Maxillofac. Surg. 2020, 10, 88–90. [Google Scholar] [PubMed]
- Mardinger, O.; Poliakov, H.; Beitlitum, I.; Nissan, J.; Chaushu, G. The patient’s perception of recovery after maxillary sinus augmentation: A prospective study. J. Periodontol. 2009, 80, 572–576. [Google Scholar] [CrossRef] [PubMed]
- Klages, U.; Ulusoy, O.; Kianifard, S.; Wehrbein, H. Dental trait anxiety and pain sensitivity as predictors of expected and experienced pain in stressful dental procedures. Eur. J. Oral Sci. 2004, 112, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Conrad, S.M.; Blakey, G.H.; Shugars, D.A.; Marciani, R.D.; Philips, C.; White, R.P., Jr. Patient’s perception of recovery after third molar surgery. J. Oral Maxillofac. Surg. 1999, 57, 1288–1294. [Google Scholar] [CrossRef]
- Morton, R.P. Quality of life assessment: Integral to clinical practice. Clin. Otolaryngol. 1996, 21, 1–2. [Google Scholar] [CrossRef]
- Troidl, H.; Kusche, J.; Vestweber, K.H.; Eypasc, E.; Koeppen, L.; Bouillon, B. Quality of life: An important endpoint both in surgical practice and research. J. Chron. Dis. 1987, 40, 523–528. [Google Scholar] [CrossRef]
- Fraser, S.C.A. Quality of life measurement in surgical practice. Brit. J. Surg. 1993, 80, 163–169. [Google Scholar] [CrossRef]
- Shugars, D.A.; Benson, K.; White, R.P., Jr.; Simpson, K.N.; Bader, J.D. Developing a measure of patient perception of short-term outcomes of third molar surgery. J. Oral Maxillofac. Surg. 1996, 54, 1402–1408. [Google Scholar] [CrossRef]
- Savin, J.; Ogden, G.R. Third molar surgery—A preliminary report on aspects affecting quality of life in the early postoperative period. Brit. J. Oral Maxillofac. Surg. 1997, 35, 246–253. [Google Scholar] [CrossRef]
- Reisine, S.T.; Weber, J. The effects of temporomandibular joint disorders on patient’s quality of life. Community Dent. Health 1989, 6, 257–270. [Google Scholar]
- Chaushu, G.; Becker, A.; Zeltser, R.; Branski, S.; Chaushu, S. Patients’ perceptions of recovery after exposure of impacted teeth with a closed-eruption technique. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 690–696. [Google Scholar] [CrossRef]
- Rantavuori, K.; Lahti, S.; Hausen, H.; Seppa, L.; Karkkainen, S. Dental fear and oral health and family characteristics of Finnish children. Acta Odont. Scan. 2004, 62, 207–213. [Google Scholar] [CrossRef] [PubMed]
- AlQutub, A.W. Pain experience after dental implant placement compared to tooth extraction. Int. J. Dent. 2021, 2021, 4134932. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro-Rotta, R.F.; Lindh, C.; Pereira, A.C.; Rohlin, M. Ambiguity in bone tissue characteristics as presented in studies on dental implant planning and placement: A systematic review. Clin. Oral Implant. Res. 2011, 22, 789–801. [Google Scholar] [CrossRef] [PubMed]
- Berggren, U.; Meynert, G. Dental fear and avoidance: Causes, symptoms, and consequences. J. Am. Dent. Assoc. 1984, 109, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Kvale, G.; Berggren, U.; Milgrom, P. Dental fear in adults: A meta-analysis of behavioral interventions. Comm. Dent. Oral Epidemiol. 2004, 32, 250–264. [Google Scholar] [CrossRef]
- Valieri, M.M.; de Freitas, K.M.; Valarelli, F.P.; Cançado, R.H. Comparison of topical and infiltration anesthesia for orthodontic mini-implant placement. Dent. Press J. Orthod. 2014, 19, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Fardal, Ø.; McCulloch, C.A. Impact of anxiety on pain perception associated with periodontal and implant surgery in a private practice. J. Periodontol. 2012, 83, 1079–1085. [Google Scholar] [CrossRef] [PubMed]
- Sarapultseva, M.; Sarapultsev, A.; Medvedeva, S.; Danilova, I. Structural damage to periodontal tissues at varying rate of anesthetic injection. J. Dent. Anesth. Pain Med. 2018, 18, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Prabhat, K.C.; Maheshwari, S.; Verma, S.K.; Gupta, N.D.; Balamani, A.; Khan, M.T.; Singh, R.K. Dental anxiety and pain perception associated with the use of miniscrew implants for orthodontic anchorage. J. Ind. Orthod. Soc. 2014, 48, 163–167. [Google Scholar] [CrossRef]
- Atalay, B.; Ramazanoglu, M.; Tozan, E.N.; Ozyuvaci, H. Pain intensity and its objective determinants following implant surgery and sinus lifting: A 1-year prospective study. Niger. J. Clin. Pract. 2017, 20, 1139–1144. [Google Scholar] [CrossRef] [PubMed]
- Croog, S.H.; Baume, R.M.; Nalbandian, J. Pre-surgery psychological characteristics, pain response, and activities impairment in female patients with repeated periodontal surgery. J. Psychosom. Res. 1995, 39, 39–51. [Google Scholar] [CrossRef]
- Silveira, E.R.; Cademartori, M.G.; Schuch, H.S.; Corrêa, M.B.; Ardenghi, T.M.; Armfield, J.; Horta, B.L.; Demarco, F.F. The vicious cycle of dental fear at age 31 in a birth cohort in Southern Brazil. Community Dent. Oral Epidemiol. 2021, 49, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Li, Y.; Li, J.; Fan, L.; Yu, H. The risk of moderate-to-severe post-operative pain following the placement of dental implants. J. Oral Rehabil. 2019, 46, 836–844. [Google Scholar] [CrossRef]
- Kovačić, I.; Peršić, S.; Kranjčić, J.; Disha, V.; Rener-Sitar, K.; Čelebić, A. Short-term postoperative pain and swelling associated with mini and standard-size implants in the same patients. Int. J. Prosthodont. 2018, 31, 117–119. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, A.B.; Della Vecchia, M.P.; Cunha, T.R.; Sorgini, D.B.; Dos Reis, A.C.; Muglia, V.A.; de Albuquerque, R.F., Jr.; de Souza, R.F. Short-term post-operative pain and discomfort following insertion of mini-implants for retaining mandibular overdentures: A randomized controlled trial. J. Oral Rehabil. 2015, 42, 605–614. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Question | Median Score | ||||||
|---|---|---|---|---|---|---|---|
| POD1 | POD2 | POD3 | POD4 | POD5 | POD6 | POD7 | |
| Has it been difficult to swallow today? | 2 | 2 | 1 | 1 | 1 | 1 | 1 |
| Has it been difficult to open your mouth today? | 2 | 2 | 2 | 1.5 | 1 | 1 | 1 |
| Were there any foods you could not eat today? | 4 | 3 | 2 | 2 | 2 | 1.5 | 1 |
| Have you enjoyed your food today? | 3.5 | 3 | 2 | 2 | 2 | 1 | 1 |
| Has speech been difficult today? | 2.5 | 2 | 1 | 1 | 1 | 1 | 1 |
| Was it difficult to sleep last night? | 2 | 1 | 1 | 1 | 1 | 1 | 1 |
| Have you missed school/work? | 1.5 | 1 | 1 | 1 | 1 | 1 | 1 |
| Has it been difficult to continue your daily activities today? | 2 | 2 | 1 | 1 | 1 | 1 | 1 |
| Has there been any swelling today? | 3 | 3 | 3 | 2 | 2 | 1 | 1 |
| Has there been bruising today? | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Has there been bleeding today? | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Have you felt unwell today? | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Have you had a bad taste or bad smell in your mouth today? | 2 | 2 | 1 | 2 | 1 | 1 | 1 |
| Has there been any food debris in the operation area today? | 2 | 1 | 2 | 1 | 1 | 1 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kahn, A.; Masri, D.; Shalev, T.; Meir, H.; Sebaoun, A.; Chaushu, L. Patients’ Perception of Recovery after Dental Implant Placement. Medicina 2021, 57, 1111. https://doi.org/10.3390/medicina57101111
Kahn A, Masri D, Shalev T, Meir H, Sebaoun A, Chaushu L. Patients’ Perception of Recovery after Dental Implant Placement. Medicina. 2021; 57(10):1111. https://doi.org/10.3390/medicina57101111
Chicago/Turabian StyleKahn, Adrian, Daya Masri, Tamir Shalev, Haya Meir, Alon Sebaoun, and Liat Chaushu. 2021. "Patients’ Perception of Recovery after Dental Implant Placement" Medicina 57, no. 10: 1111. https://doi.org/10.3390/medicina57101111