
The Outcomes of Enamel Matrix Derivative on Periodontal Regeneration under Diabetic Conditions

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
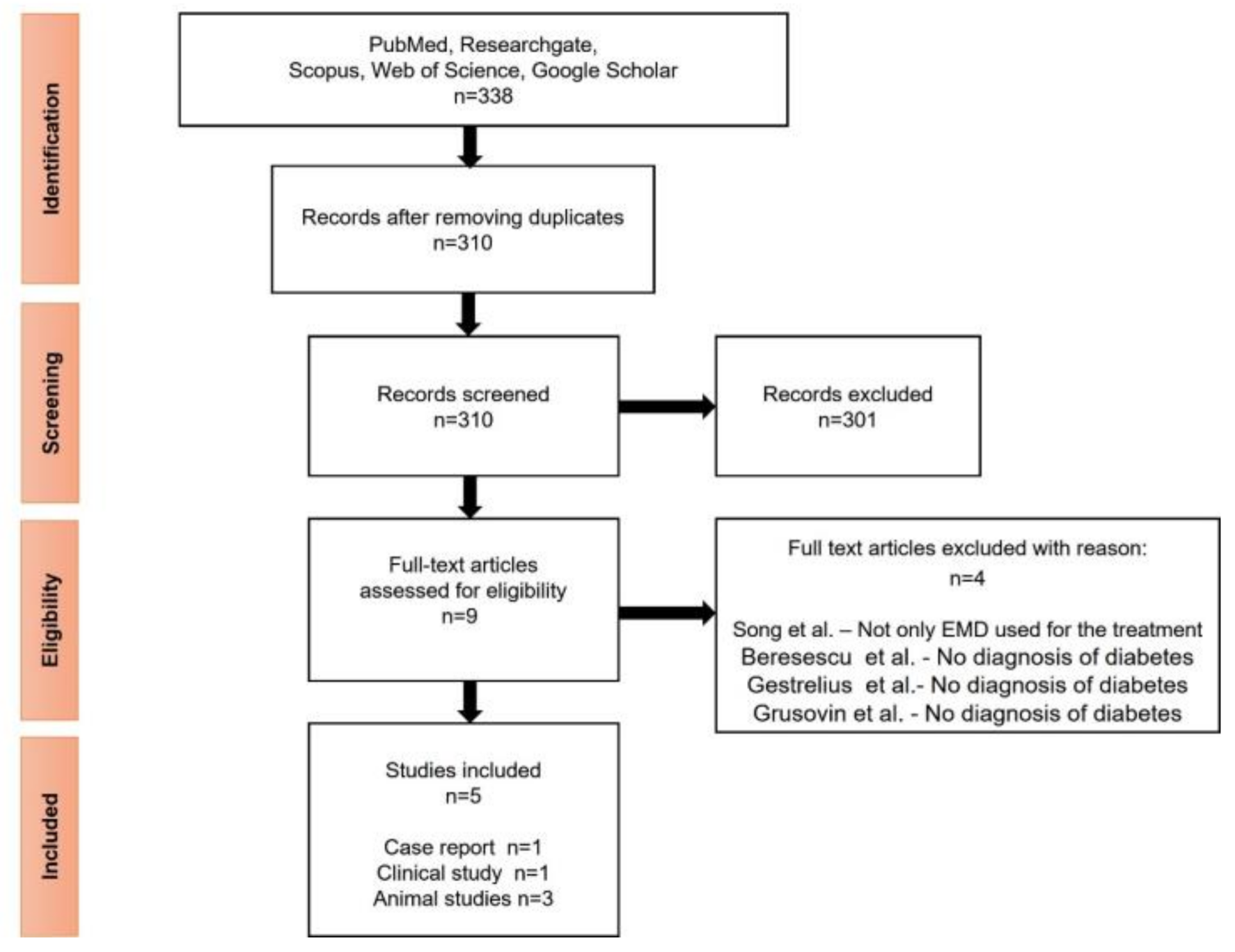
2.2. Literature Search
2.3. Data Extraction and Statistical Analysis
3. Results
3.1. Search Results and General Characteristics
3.2. Periodontal Disease Assessment and Surgical Intervention
3.3. The Outcome of EMD under Diabetic Condition
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Waqas, S.; Tahir, A.; Nadeem Shafique, B.; Hamid, M.R.A. Effect of Diet on Type 2 Diabetes Mellitus: A Review. Int. J. Health Sci. 2017, 11, 65–71. [Google Scholar]
- World Health Organization. WHO | Diabetes Factsheet; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Sanz, M.; Ceriello, A.; Buysschaert, M.; Chapple, I.; Demmer, R.T.; Graziani, F.; Herrera, D.; Jepsen, S.; Lione, L.; Madianos, P.; et al. Scientific Evidence on the Links between Periodontal Diseases and Diabetes: Consensus Report and Guidelines of the Joint Workshop on Periodontal Diseases and Diabetes by the International Diabetes Federation and the European Federation of Periodontology. J. Clin. Periodontol. 2018, 137, 231–241. [Google Scholar] [CrossRef]
- Preshaw, P.M.; Bissett, S.M. Periodontitis and Diabetes. Br. Dent. J. 2019, 227, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Polak, D.; Shapira, L. An Update on the Evidence for Pathogenic Mechanisms That May Link Periodontitis and Diabetes. J. Clin. Periodontol. 2018, 45. [Google Scholar] [CrossRef] [PubMed]
- Junior, R.L.; Santos, C.; Oliveira, B.; Fischer, R.G.; Santos, A.P.P. Effects on HbA1c in Diabetic Patients of Adjunctive Use of Systemic Antibiotics in Nonsurgical Periodontal Treatment: A Systematic Review. J. Dent. 2017, 66, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Mathew, J.E.; Jacob, J.J.; Kalra, S. Periodontitis Management in Diabetes Care. J. Pak. Med. Assoc. 2021, 71, 2097–2099. [Google Scholar] [PubMed]
- Zhang, X.; Wang, M.; Wang, X.; Qu, H.; Zhang, R.; Gu, J.; Wu, Y.; Ni, T.; Tang, W.; Li, Q. Relationship between Periodontitis and Microangiopathy in Type 2 Diabetes Mellitus: A Meta-analysis. J. Periodontal Res. 2021, 1–9. [Google Scholar] [CrossRef]
- Nitta, H.; Katagiri, S.; Nagasawa, T.; Izumi, Y.; Ishikawa, I.; Izumiyama, H.; Uchimura, I.; Kanazawa, M.; Chiba, H.; Matsuo, A.; et al. The Number of Microvascular Complications Is Associated with an Increased Risk for Severity of Periodontitis in Type 2 Diabetes Patients: Results of a Multicenter Hospital-Based Cross-Sectional Study. J. Diabetes Investig. 2017, 8, 677–686. [Google Scholar] [CrossRef] [PubMed]
- Lyngstadaas, S.P.; Wohlfahrt, J.C.; Brookes, S.J.; Paine, M.L.; Snead, M.L.; Reseland, J.E. Enamel Matrix Proteins; Old Molecules for New Applications. Orthod. Craniofacial Res. 2009, 12, 243–253. [Google Scholar] [CrossRef] [Green Version]
- Miron, R.J.; Dard, M.; Weinreb, M. Enamel Matrix Derivative, Inflammation and Soft Tissue Wound Healing. J. Periodontal Res. 2015, 50, 555–569. [Google Scholar] [CrossRef]
- Ivanovski, S.; Esposito, M.; Grusovin, M.G.; Papanikolaou, N.; Coulthard, P.; Worthington, H.V. Enamel Matrix Derivative (Emdogain®) for Periodontal Tissue Regeneration in Intrabony Defects. Aust. Dent. J. 2010, 55, 101–104. [Google Scholar] [CrossRef] [Green Version]
- Rathva, V.J. Enamel Matrix Protein Derivatives: Role in Periodontal Regeneration. Clin. Cosmet. Investig. Dent. 2011, 3, 79–92. [Google Scholar] [CrossRef] [Green Version]
- Kuramitsu-Fujimoto, S.; Ariyoshi, W.; Saito, N.; Okinaga, T.; Kamo, M.; Ishisaki, A.; Takata, T.; Yamaguchi, K.; Nishihara, T. Novel Biological Activity of Ameloblastin in Enamel Matrix Derivative. J. Appl. Oral Sci. 2015, 23, 49–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spahr, A.; Lyngstadaas, S.P.; Boeckh, C.; Andersson, C.; Podbielski, A.; Haller, B. Effect of the Enamel Matrix Derivative Emdogain® on the Growth of Periodontal Pathogens in Vitro. J. Clin. Periodontol. 2002, 29, 62–72. [Google Scholar] [CrossRef]
- Grandin, H.M.; Gemperli, A.C.; Dard, M. Enamel Matrix Derivative: A Review of Cellular Effects in Vitro and a Model of Molecular Arrangement and Functioning. Tissue Eng. -Part B Rev. 2012, 18, 181–202. [Google Scholar] [CrossRef] [PubMed]
- Mancini, L.; Fratini, A.; Marchetti, E. Periodontal Regeneration. Encyclopedia 2021, 1, 11. [Google Scholar] [CrossRef]
- Mancini, L.; Romandini, M.; Fratini, A.; Americo, L.M.; Panda, S.; Marchetti, E. Biomaterials for Periodontal and Peri-Implant Regeneration. Materials 2021, 14, 3319. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Estarli, M.; Barrera, E.S.A.; et al. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeda, K.; Mizutani, K.; Matsuura, T.; Kido, D.; Mikami, R.; Noda, M.; Buranasin, P.; Sasaki, Y.; Izumi, Y. Periodontal Regenerative Effect of Enamel Matrix Derivative in Diabetes. PLoS ONE 2018, 13, e0207201. [Google Scholar] [CrossRef]
- Shirakata, Y.; Eliezer, M.; Nemcovsky, C.E.; Weinreb, M.; Dard, M.; Sculean, A.; Bosshardt, D.D.; Moses, O. Periodontal Healing after Application of Enamel Matrix Derivative in Surgical Supra/Infrabony Periodontal Defects in Rats with Streptozotocin-Induced Diabetes. J. Periodontal Res. 2014, 49, 93–101. [Google Scholar] [CrossRef]
- Mizutani, K.; Shioyama, H.; Matsuura, T.; Mikami, R.; Takeda, K.; Izumi, Y.; Aoki, A.; Iwata, T. Periodontal Regenerative Therapy in Patients with Type 2 Diabetes Using Minimally Invasive Surgical Technique with Enamel Matrix Derivative under 3-Year Observation: A Prospective Cohort Study. J. Periodontol. 2020, 92, 1262–1273. [Google Scholar] [CrossRef]
- Corrêa, M.G.; Gomes Campos, M.L.; Marques, M.R.; Casati, M.Z.; Nociti, F.H.; Sallum, E.A. Histometric Analysis of the Effect of Enamel Matrix Derivative on the Healing of Periodontal Defects in Rats With Diabetes. J. Periodontol. 2013, 84, 1309–1318. [Google Scholar] [CrossRef]
- Seshima, F.; Nishina, M.; Namba, T.; Saito, A. Periodontal Regenerative Therapy in Patient with Chronic Periodontitis and Type 2 Diabetes Mellitus: A Case Report. Bull. Tokyo Dent. Coll. 2016, 57, 97–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, W.; Cai, W.; Li, J.; Jiang, F.; He, S. Predicting Blood Glucose Levels with EMD and LSTM Based CGM Data. In Proceedings of the 2019 6th International Conference on Systems and Informatics, ICSAI 2019, Shanghai, China, 2–4 November 2019. [Google Scholar] [CrossRef]
- Beresescu, G.F.; Ormenisan, A.; Szekely, M.; Monea, M.; Monea, A. Clinical Outcomes after Regenerative Periodontal Therapy with Emdogain. Acta Med. Marisiensis 2017, 63, 136–139. [Google Scholar] [CrossRef] [Green Version]
- Gestrelius, S.; Lyngstadaas, S.P.; Hammarström, L. Emdogain--Periodontal Regeneration Based on Biomimicry. Clin. Oral Investig. 2000, 4, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Grusovin, M.G.; Esposito, M. The Efficacy of Enamel Matrix Derivative (Emdogain) for the Treatment of Deep Infrabony Periodontal Defects: A Placebo-Controlled Randomised Clinical Trial. Eur. J. Oral Implantol. 2009, 2, 43–54. [Google Scholar]
- Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2010, 33, S62–S69. [CrossRef] [PubMed] [Green Version]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Clin. Periodontol. 2018, 45, S149–S161. [Google Scholar] [CrossRef] [Green Version]
- Miron, R.J.; Sculean, A.; Cochran, D.L.; Froum, S.; Zucchelli, G.; Nemcovsky, C.; Donos, N.; Lyngstadaas, S.P.; Deschner, J.; Dard, M.; et al. Twenty years of enamel matrix derivative: The past, the present and the future. J. Clin. Periodontol. 2016, 43, 668–683. [Google Scholar] [CrossRef]
- Rexhepi, I.; Paolantonio, M.; Romano, L.; Serroni, M.; Santamaria, P.; Secondi, L.; Paolantonio, G.; Sinjari, B.; De Ninis, P.; Femminella, B. The efficacy of inorganic bovine bone combined with leukocyte and platelet-rich fibrin or collagen membranes for treating unfavorable periodontal infrabony defects: Randomized non-inferiority trial. J. Periodontol. 2021, 1–12. [Google Scholar] [CrossRef]
- Cassetta, M.; Perrotti, V.; Calasso, S.; Piattelli, A.; Sinjari, B.; Iezzi, G. Bone formation in sinus augmentation procedures using autologous bone, porcine bone, and a 50:50 mixture: A human clinical and histological evaluation at 2 months. Clin. Oral Implant. Res. 2015, 26, 1180–1184. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Studies Characteristics | Periodontal Disease Assessments | ||||||
|---|---|---|---|---|---|---|---|
| Author. Year. Country. | Study Type | Sample Size | Characteristics | Measurements | Results | Conclusions | |
| Mizutani, 2020, Japan [22] | Prospective cohort study | DM group: n = 10 Non-DM group: n = 18 | DM group: (a) Mean age: 67.5 ± 7.6 (b) Sex: male (n = 4) female (n = 6) (c) BMI: 23.9 ± 3.1 d) HbA1c: 6.82 ± 0.72% Non-DM group: (a) Mean age: 63.1 ± 9.7 (b) Sex: male (n = 5) female (n = 13) (c) BMI: 22.8 ± 2.7 (d) HbA1c: NA | PPD CAL PCR REC BOP Periapical radiographs Tooth mobility | Intrabony Defects | The combination of minimally invasive surgical technique and EMD for the regenerative periodontal surgery showed successful results for both DM and non-DM groups. | |
| Pre-operative PPD (mm) (a) DM group 7.1 ± 1.6 (b) Non-DM group 7.0 ± 1.3 CAL (mm) (a) DM group 7.6 ± 1.5 (b) Non-DM group 7.8 ± 1.5 Radiographical defect (mm) (a) DM group 4.6 ± 0.9 (b) Non-DM group 4.8 ± 1.5 | Post-operative (1 year and 3 years) PPD (mm) (a) DM group 4.8 ± 1.5; 4.5 ± 1.4 b) Non-DM group 4.8 ± 1.5; 4.7 ± 1.4 CAL (a) DM group 4.1 ± 1.2; 3.8 ± 1.1 (b) Non-DM group 4.3 ± 1.1; 4.1 ± 1.1 Radiographical defect (mm) (a) DM group 2.5 ± 0.7; 2.6 ± 0.6 (b) Non-DM group 3.1 ± 1.4; 3.2 ± 1.3 | ||||||
| Seshima, 2016, Japan [24] | Case report | n = 1 | Age: 66 years Gender: male HbA1c: 7.8% | CAL PPD Furcation Tooth mobility OHRQL | Intrabony Defects | The use of EMD in intrabony defects had favorable outcomes. | |
| Pre-operative PPD (mm) Tooth 1.6: 10 Tooth 2.6: 7 Tooth 2.7: 9 CAL (mm) Tooth 1.6: 10 Tooth 2.6: 7 Tooth 2.7: 9 | Post-operative (7 months) PPD (mm) Tooth 1.6: 5 Tooth 2.6: 3 Tooth 2.7: 4 CAL (mm) Tooth 1.6: 6 Tooth 2.6: 4 Tooth 2.7: 8 | ||||||
| Author. Year. Country. | Sample Size, Type of Animal | Measurements | Results | Conclusions |
|---|---|---|---|---|
| Takeda, 2018, Japan [20] | DM group: n = 18 Control group: n = 18 Male Wistar rats | Histomorphometrically analysis: cement–enamel junction to the bottom of the bone defect, length of the junctional epithelium, newly formed cementum, new bone, area of new bone, and area of new cementum. Micro-CT analysis: bone volume, cancellous bone volume, bone mineral density, cancellous mineral content | Defects were filled with new connective tissue, new cementum, and new bone after 28 days in both groups. In the DM group, sparse and oblique collagen fibers were detected; in the control group, dense and vertical collagen fibers were present. Newly formed connective tissue attachment and bone were increased at EMD-treated sites. | Bone regeneration was noticed when EMD was used, but it was diminished in DM rats. |
| Shirakata, 2014, Switzerland [21] | DM group: n = 15 Control group: n = 15 Male Wistar rats | Histomorphometrically analysis: root length, defect depth, sulcus depth, gingival recession, length of junctional epithelium, supracrestal connective tissue, new bone, new cementum, ankylosis | Root length and defect depth values were comparable in all groups and there were no statistical difference. Gingival recession was greater in diabetic rats. The length of junctional epithelium was smaller in the EMD-treated sites of both DM and control animals. Sulcus depth and length supracrestal connective tissue differences were not seen between the groups. New bone formation was mostly situated on the apical site of the defect. New cementum has been seen in none of the groups. | EMD had no benefits in the formation of new bone and cementum. |
| Corrêa, 2012, Brazil [23] | DM: n = 10 Non-DM: n = 10 Male Wistar rats | Defect fill The density of newly formed bone New cementum formation Number of osteoclasts | Defect fill: DM showed less defect fill than control, for the EMD-treated defects and non-treated controls. Bone density: Statistically significant differences were noticed in bone density between DM and non-DM, in the EMD-treated sites and the non-treated controls. New cementum formation: No statistically significant difference in new cementum formation between DM and non-DM, for EMD-treated sites and non-treated control. | EMD determined an increased defect fill in both groups and enhanced bone density and new cementum formation only in non-diabetic animals. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Narita, L.E.; Mester, A.; Onisor, F.; Bran, S.; Onicas, M.I.; Voina-Tonea, A. The Outcomes of Enamel Matrix Derivative on Periodontal Regeneration under Diabetic Conditions. Medicina 2021, 57, 1071. https://doi.org/10.3390/medicina57101071
Narita LE, Mester A, Onisor F, Bran S, Onicas MI, Voina-Tonea A. The Outcomes of Enamel Matrix Derivative on Periodontal Regeneration under Diabetic Conditions. Medicina. 2021; 57(10):1071. https://doi.org/10.3390/medicina57101071
Chicago/Turabian StyleNarita, Laura Elena, Alexandru Mester, Florin Onisor, Simion Bran, Maria Ioana Onicas, and Andrada Voina-Tonea. 2021. "The Outcomes of Enamel Matrix Derivative on Periodontal Regeneration under Diabetic Conditions" Medicina 57, no. 10: 1071. https://doi.org/10.3390/medicina57101071