It’s Not All about Echocardiography. Open the Lung Window for the Cardiac Emergencies


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Clinical Utility in Common Cardiac-Related Emergencies
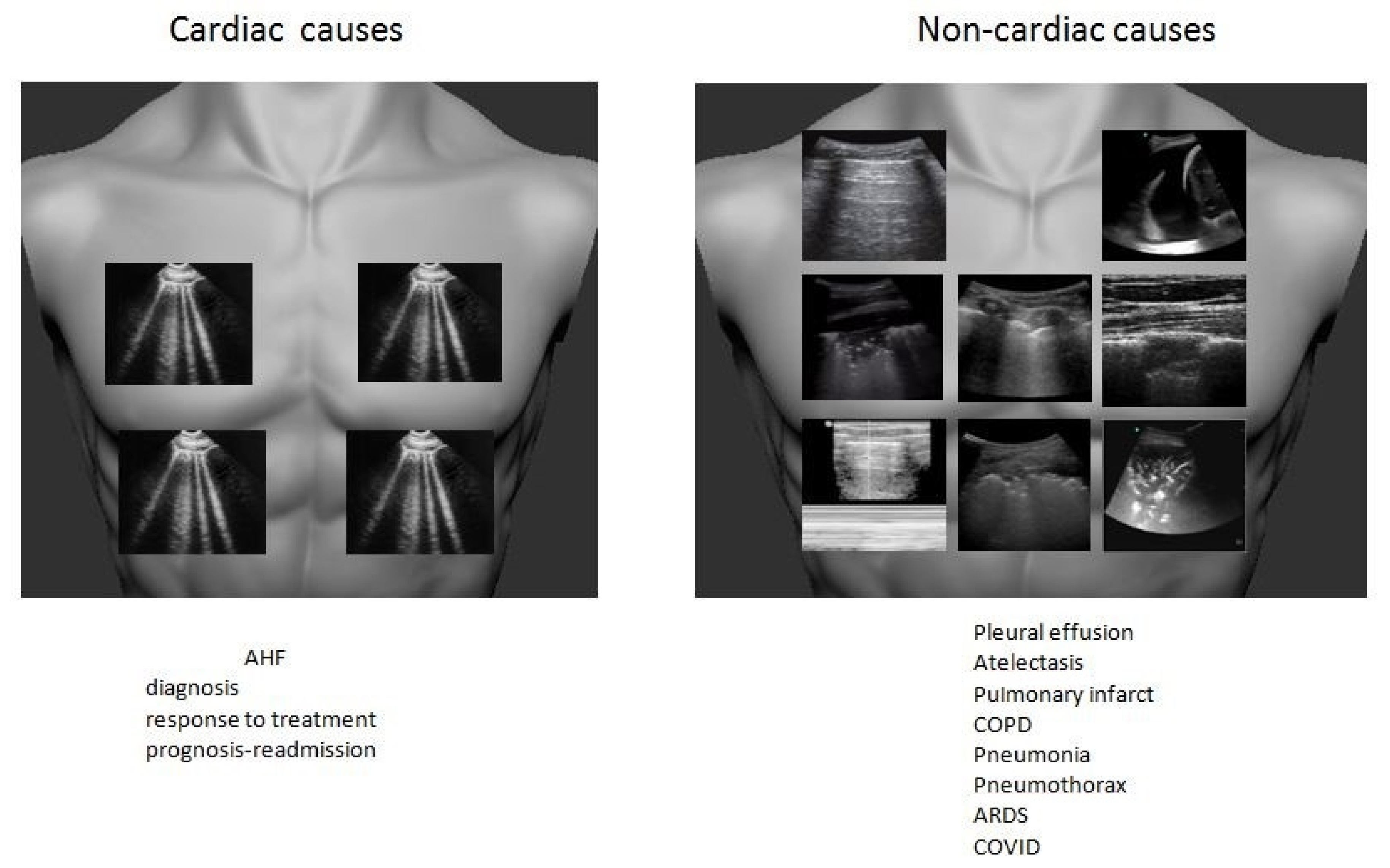
2.1. Undifferentiated Dyspnea
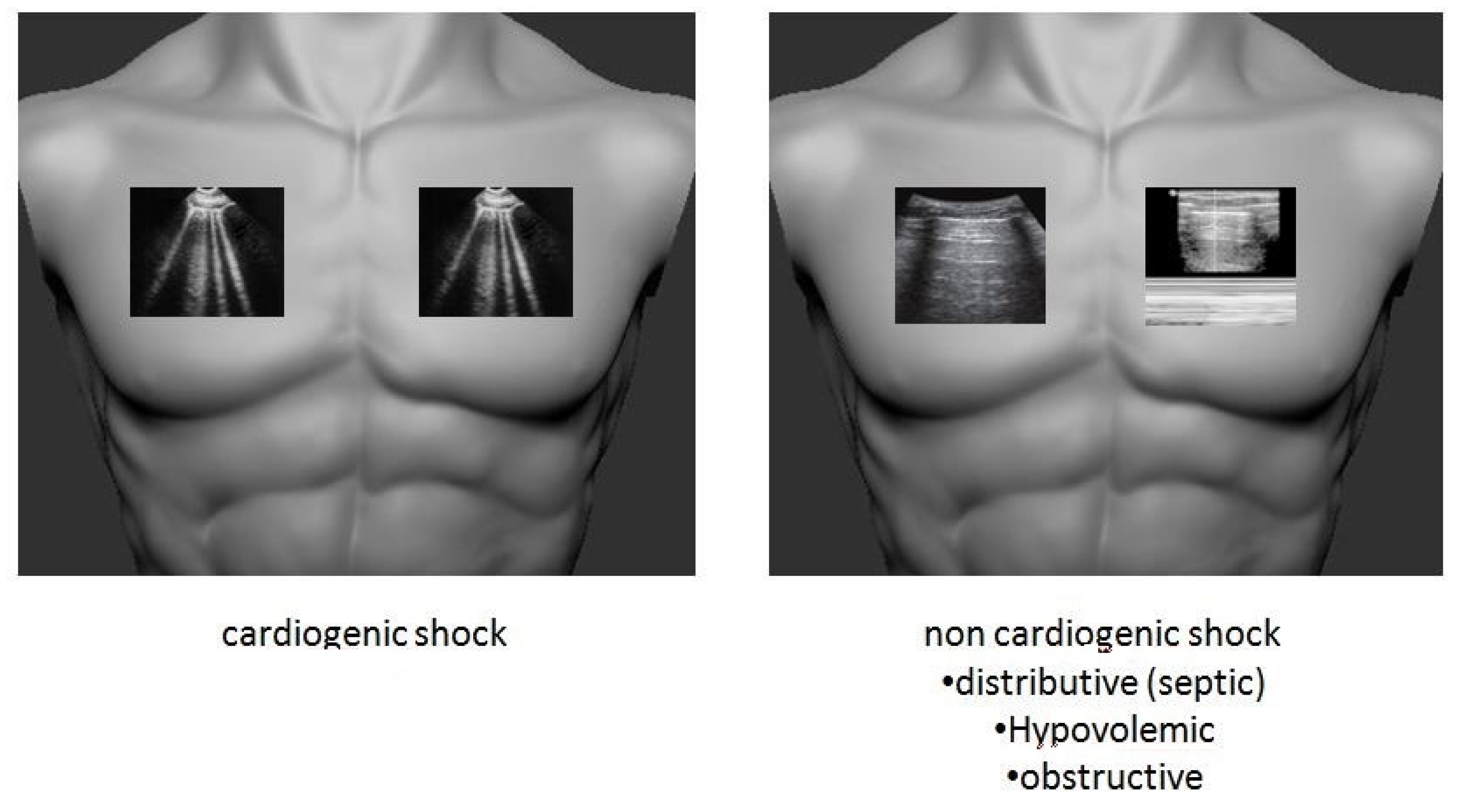
2.2. Undifferentiated Shock
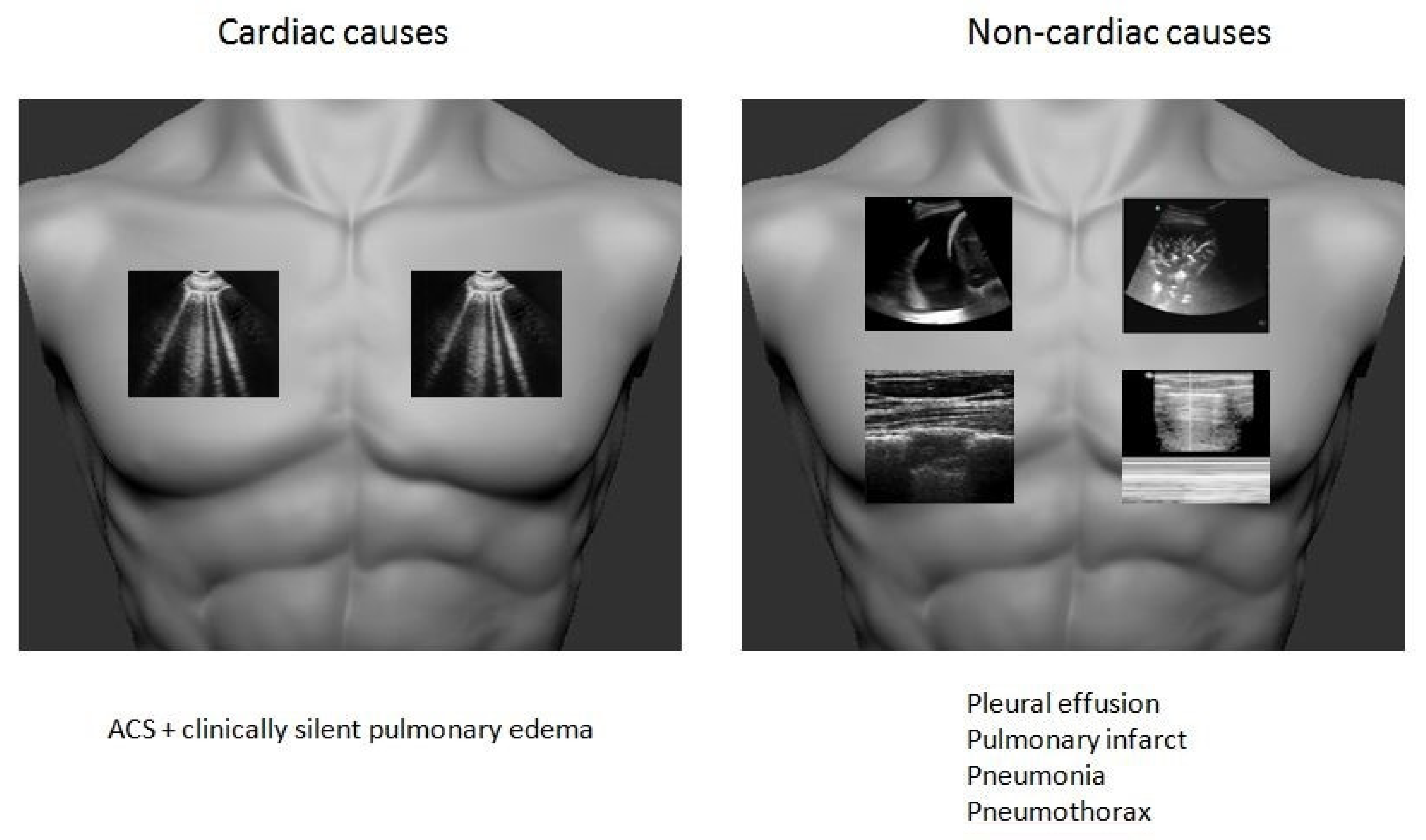
2.3. Chest Pain
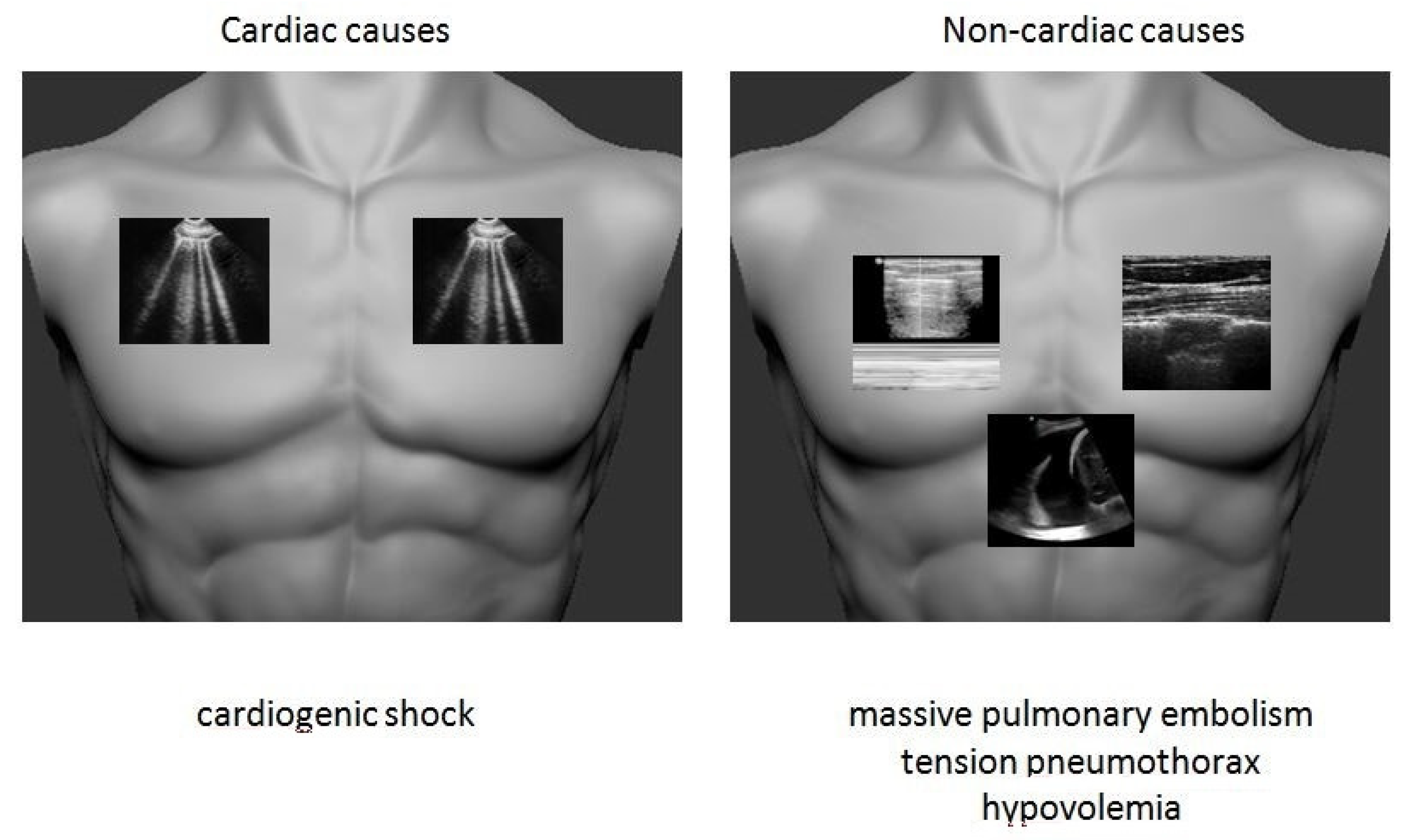
2.4. Cardiac Arrest
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ponikowski, P. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [PubMed]
- Lichtenstein, D.; Goldstein, I.; Mourgeon, E.; Cluzel, P.; Grenier, P.; Rouby, J. Comparative diagnostic performances of auscultation, chest radiography, and lung ultrasonography in acute respiratory distress syndrome. Anesthesiology 2004, 100, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Pivetta, E.; Goffi, A.; Nazerian, P.; Castagno, D.; Tozzetti, C.; Tizzani, P.; Tizzani, M.; Porrino, G.; Ferreri, E.; Busso, V.; et al. Lung ultrasound integrated with clinical assessment for the diagnosis of acute decompensated heart failure in the emergency department: A randomized controlled trial. Eur. J. Heart Fail. 2019, 21, 754–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiemstra, B.; Eck, R.J.; Keus, F.; van der Horst, I.C.C. Clinical examination for diagnosing circulatory shock. Curr. Opin. Crit. Care 2017, 23, 293–301. [Google Scholar] [CrossRef]
- Goodacre, S.; Locker, T.; Morris, F.; Campbell, S. How useful are clinical features in the diagnosis of acute, undifferentiated chest pain? Acad. Emerg. Med. 2002, 9, 203–208. [Google Scholar] [CrossRef]
- Lichtenstein, D.; Meziere, G.; Biderman, P.; Gepner, A.; Barre, O. The comet-tail artifact. An ultrasound sign of alveolar-interstitial syndrome. Am. J. Respir. Crit. Care Med. 1997, 156, 1640–1646. [Google Scholar] [CrossRef] [PubMed]
- Barillari, A. Lung ultrasound: A new tool for the emergency physician. Intern. Emerg. Med. 2010, 5, 335–340. [Google Scholar] [CrossRef]
- Reissig, A.; Copetti, R.; Mathis, G.; Mempel, C.; Schuler, A.; Zechner, P.; Aliberti, S.; Neumann, R.; Kroegel, C.; Hoyer, H. Lung ultrasound in the diagnosis and follow-up of community-acquired pneumonia: A prospective, multicenter, diagnostic accuracy study. Chest 2012, 142, 965–972. [Google Scholar] [CrossRef] [Green Version]
- Miglioranza, M.H.; Sousa, A.C.S.; Araujo, C.d.C.; Almeida-Santos, M.A.; Gargani, L. Lung Ultrasound: The Cardiologists’ New Friend. Arq. Bras. Cardiol. 2017, 109, 606–608. [Google Scholar] [CrossRef]
- Ha, Y.R. Clinically integrated multi-organ point-of-care ultrasound for undifferentiated respiratory difficulty, chest pain, or shock: A critical analytic review. J. Intensive Care 2016, 4, 54. [Google Scholar] [CrossRef] [Green Version]
- Hew, M. The efficacy of bedside chest ultrasound: From accuracy to outcomes. Eur. Respir. Rev. 2016, 25, 230–246. [Google Scholar] [CrossRef] [Green Version]
- Picano, E.; Scali, M.C.; Ciampi, Q.; Lichtenstein, D. Lung Ultrasound for the Cardiologist. JACC Cardiovasc. Imaging 2018, 11, 1692–1705. [Google Scholar] [CrossRef] [PubMed]
- Neskovic, A.N.; Hagendorff, A.; Lancellotti, P.; Guarracino, F.; Varga, A.; Cosyns, B.; Flachskampf, F.A.; Popescu, B.A.; Gargani, L.; Zamorano, J.L.; et al. Emergency echocardiography: The European Association of Cardiovascular Imaging recommendations. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lichtenstein, D.A.; Meziere, G.A. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: The BLUE protocol. Chest 2008, 134, 117–125. [Google Scholar] [CrossRef] [Green Version]
- Maw, A.M.; Hassanin, A.; Ho, P.M.; McInnes, M.D.F.; Moss, A.; Juarez-Colunga, E.; Soni, N.J.; Miglioranza, M.H.; Platz, E.; DeSanto, K.; et al. Diagnostic Accuracy of Point-of-Care Lung Ultrasonography and Chest Radiography in Adults With Symptoms Suggestive of Acute Decompensated Heart Failure: A Systematic Review and Meta-analysis. JAMA Netw. Open 2019, 2, e190703. [Google Scholar] [CrossRef] [PubMed]
- Platz, E.; Jhund, P.S.; Girerd, N.; Pivetta, E.; McMurray, J.J.V.; Peacock, W.F.; Masip, J.; Martin-Sanchez, F.J.; Miro, O.; Price, S.; et al. Expert consensus document: Reporting checklist for quantification of pulmonary congestion by lung ultrasound in heart failure. Eur. J. Heart Fail. 2019, 21, 844–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Deeb, M.; Barbic, S.; Featherstone, R.; Dankoff, J.; Barbic, D. Point-of-care ultrasonography for the diagnosis of acute cardiogenic pulmonary edema in patients presenting with acute dyspnea: A systematic review and meta-analysis. Acad. Emerg. Med. 2014, 21, 843–852. [Google Scholar] [CrossRef]
- Pivetta, E.; Goffi, A.; Lupia, E.; Tizzani, M.; Porrino, G.; Ferreri, E.; Volpicelli, G.; Balzaretti, P.; Banderali, A.; Iacobucci, A.; et al. Lung Ultrasound-Implemented Diagnosis of Acute Decompensated Heart Failure in the ED: A SIMEU Multicenter Study. Chest 2015, 148, 202–210. [Google Scholar] [CrossRef] [Green Version]
- Martindale, J.L.; Wakai, A.; Collins, S.P.; Levy, P.D.; Diercks, D.; Hiestand, B.C.; Fermann, G.J.; Desouza, I.; Sinert, R. Diagnosing Acute Heart Failure in the Emergency Department: A Systematic Review and Meta-analysis. Acad. Emerg. Med. 2016, 23, 223–242. [Google Scholar] [CrossRef] [Green Version]
- Bistola, V.; Polyzogopoulou, E.; Ikonomidis, I.; Parissis, J. Lung ultrasound for the diagnosis of acute heart failure: Time to upgrade current indication? Eur. J. Heart Fail. 2019, 21, 767–769. [Google Scholar] [CrossRef]
- Gargani, L. Ultrasound of the Lungs: More than a Room with a View. Heart Fail. Clin. 2019, 15, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Martindale, J.L. Resolution of sonographic B-lines as a measure of pulmonary decongestion in acute heart failure. Am. J. Emerg. Med. 2016, 34, 1129–1132. [Google Scholar] [CrossRef] [PubMed]
- Martindale, J.L.; Secko, M.; Kilpatrick, J.F.; deSouza, I.S.; Paladino, L.; Aherne, A.; Mehta, N.; Conigiliaro, A.; Sinert, R. Serial Sonographic Assessment of Pulmonary Edema in Patients with Hypertensive Acute Heart Failure. J. Ultrasound Med. 2018, 37, 337–345. [Google Scholar] [CrossRef]
- Miglioranza, M.H.; Picano, E.; Badano, L.P.; Sant’Anna, R.; Rover, M.; Zaffaroni, F.; Sicari, R.; Kalil, R.K.; Leiria, T.L.; Gargani, L. Pulmonary congestion evaluated by lung ultrasound predicts decompensation in heart failure outpatients. Int. J. Cardiol. 2017, 240, 271–278. [Google Scholar] [PubMed] [Green Version]
- Lichtenstein, D.A. Lung ultrasound for the cardiologist-a basic application: The B-profile of the Bedside Lung Ultrasound in Emergencies protocol for diagnosing haemodynamic pulmonary oedema. Arch. Cardiovasc. Dis. 2020, 113, 489–491. [Google Scholar] [CrossRef] [PubMed]
- Schor, E.H.; Delgado Mosquera, C.J. Lung Ultrasound in Cardiology: A Window to Pulmonary Edema. Rev. Argentina Cardiol. 2019, 87, 463–468. [Google Scholar] [CrossRef]
- Lee, F.C. Lung ultrasound-a primary survey of the acutely dyspneic patient. J. Intensive Care 2016, 4, 57. [Google Scholar] [CrossRef] [Green Version]
- Kiamanesh, O.; Harper, L.; Wiskar, K.; Luksun, W.; McDonald, M.; Ross, H.; Woo, A.; Granton, J. Lung Ultrasound for Cardiologists in the Time of COVID-19. Can. J. Cardiol. 2020, 36, 1144–1147. [Google Scholar] [CrossRef]
- Lichtenstein, D. FALLS-protocol: Lung ultrasound in hemodynamic assessment of shock. Heart Lung Vessel 2013, 5, 142–147. [Google Scholar]
- Perera, P.; Mailhot, T.; Riley, D.; Mandavia, D. The RUSH exam: Rapid Ultrasound in SHock in the evaluation of the critically lll. Emerg. Med. Clin. North. Am. 2010, 28, 29–56. [Google Scholar] [CrossRef]
- Atkinson, P.; Bowra, J.; Milne, J.; Lewis, D.; Lambert, M.; Jarman, B.; Noble, V.E.; Lamprecht, H.; Harris, T.; Connolly, J.; et al. International Federation for Emergency Medicine Consensus Statement: Sonography in hypotension and cardiac arrest (SHoC): An international consensus on the use of point of care ultrasound for undifferentiated hypotension and during cardiac arrest. CJEM 2017, 19, 459–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lichtenstein, D.A. Integrating lung ultrasound in the hemodynamic evaluation of acute circulatory failure (the fluid administration limited by lung sonography protocol). J. Crit. Care 2012, 27, 533.e11–533.e19. [Google Scholar] [CrossRef] [PubMed]
- Pandompatam, G.; Sweeney, D.A.; Diaz-Gomez, J.L.; Wiley, B.M. Integrated Cardiac and Lung Ultrasound (ICLUS) in the Cardiac Intensive Care Unit. Curr. Cardiovasc. Imaging Rep. 2018, 11, 23. [Google Scholar] [CrossRef]
- Bedetti, G. Comparison of prognostic value of echographic [corrected] risk score with the Thrombolysis in Myocardial Infarction (TIMI) and Global Registry in Acute Coronary Events (GRACE) risk scores in acute coronary syndrome. Am. J. Cardiol. 2010, 106, 1709–1716. [Google Scholar] [CrossRef] [PubMed]
- Araujo, G.N.; Silveira, A.D.; Scolari, F.L.; Custodio, J.L.; Marques, F.P.; Beltrame, R.; Menegazzo, W.; Machado, G.P.; Fuchs, F.C.; Goncalves, S.C.; et al. Admission Bedside Lung Ultrasound Reclassifies Mortality Prediction in Patients with ST-Segment-Elevation Myocardial Infarction. Circ. Cardiovasc. Imaging 2020, 13, e010269. [Google Scholar] [CrossRef]
- Lichtenstein, D.A. Critical care ultrasound in cardiac arrest. Technological requirements for performing the SESAME-protocol—A holistic approach. Anaesthesiol. Intensive Ther. 2015, 47, 471–481. [Google Scholar] [CrossRef] [Green Version]
- Hernandez, C.; Shuler, K.; Hannan, H.; Sonyika, C.; Likourezos, A.; Marshall, J. C.A.U.S.E.: Cardiac arrest ultra-sound exam—A better approach to managing patients in primary non-arrhythmogenic cardiac arrest. Resuscitation 2008, 76, 198–206. [Google Scholar] [CrossRef]
- Knudtson, J.L.; Shuler, K.; Hannan, H.; Sonyika, C.; Likourezos, A.; Marshall, J. Surgeon-performed ultrasound for pneumothorax in the trauma suite. J. Trauma 2004, 56, 527–530. [Google Scholar] [CrossRef]
- Lichtenstein, D.A.; Van Hooland, S.; Elbers, P.; Malbrain, M.L.N.G. Ten good reasons to practice ultrasound in critical care. Anaesthesiol. Intensive Ther. 2014, 46, 323–335. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polyzogopoulou, E.; Boultadakis, A.; Ikonomidis, I.; Parissis, J. It’s Not All about Echocardiography. Open the Lung Window for the Cardiac Emergencies. Medicina 2021, 57, 69. https://doi.org/10.3390/medicina57010069
Polyzogopoulou E, Boultadakis A, Ikonomidis I, Parissis J. It’s Not All about Echocardiography. Open the Lung Window for the Cardiac Emergencies. Medicina. 2021; 57(1):69. https://doi.org/10.3390/medicina57010069
Chicago/Turabian StylePolyzogopoulou, Eftihia, Antonios Boultadakis, Ignatios Ikonomidis, and John Parissis. 2021. "It’s Not All about Echocardiography. Open the Lung Window for the Cardiac Emergencies" Medicina 57, no. 1: 69. https://doi.org/10.3390/medicina57010069