Glycemia, Beta-Cell Function and Sensitivity to Insulin in Mildly to Critically Ill Covid-19 Patients


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
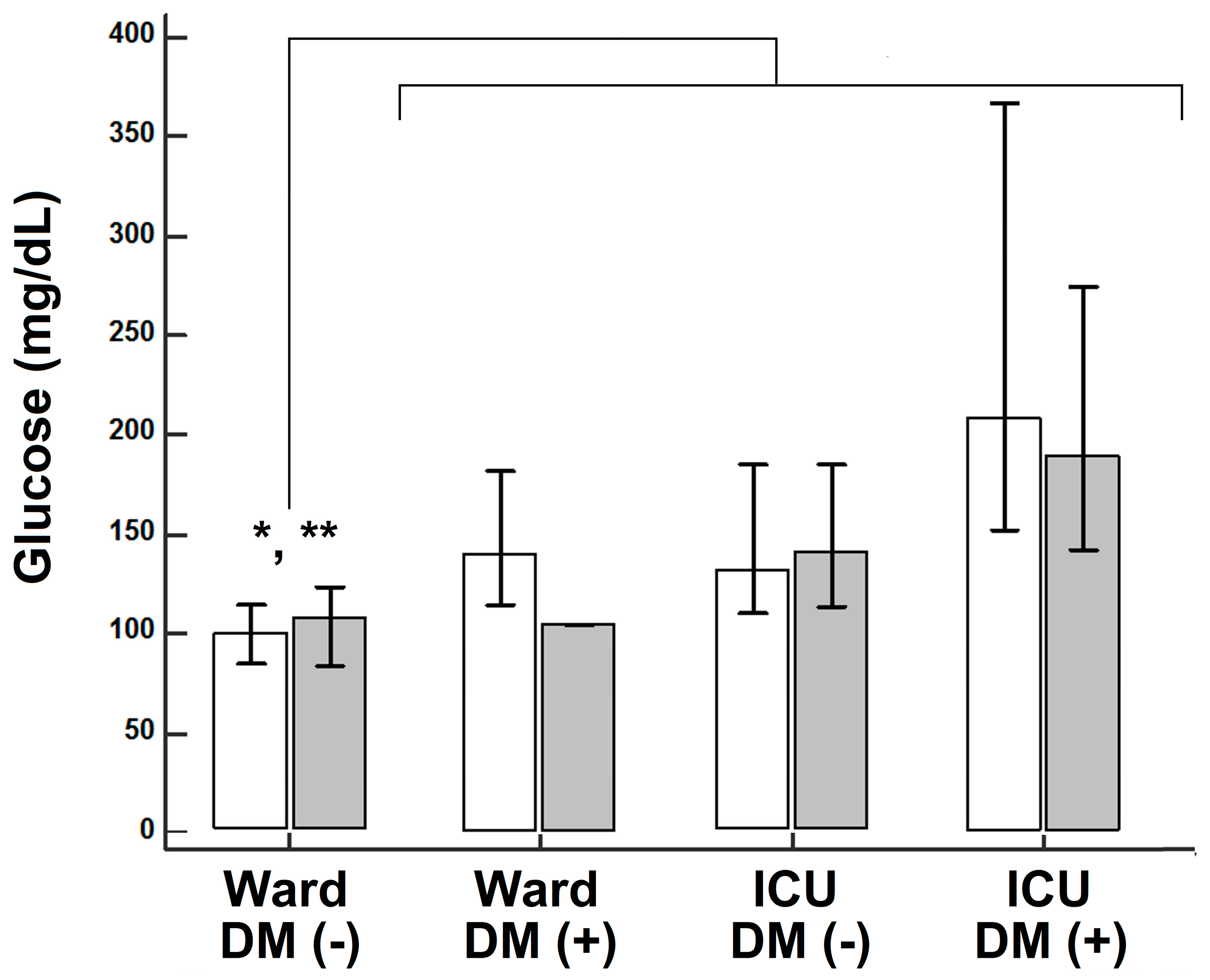
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ilias, I.; Zabuliene, L. Hyperglycemia and the novel Covid-19 infection: Possible pathophysiologic mechanisms. Med. Hypotheses 2020, 139, 109699. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Iacobellis, G.; Penaherrera, C.A.; Bermudez, L.E.; Bernal Mizrachi, E. Admission hyperglycemia and radiological findings of SARS-CoV2 in patients with and without diabetes. Diabetes Res. Clin. Pract. 2020, 164, 108185. [Google Scholar] [CrossRef] [PubMed]
- Ilias, I.; Jahaj, E.; Kokkoris, S.; Zervakis, D.; Temperikidis, P.; Magira, E.; Pratikaki, M.; Vassiliou, A.G.; Routsi, C.; Kotanidou, A.; et al. Clinical Study of Hyperglycemia and SARS-CoV-2 Infection in Intensive Care Unit Patients. In Vivo 2020, 34, 3029–3032. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Du, C.; Zhang, Y.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, e200994. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Wu, C.; Wang, X.; Yu, J.; Sun, Z. The Impact of COVID-19 on Blood Glucose: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2020, 11, 574541. [Google Scholar] [CrossRef]
- Carrasco-Sánchez, F.J.; López-Carmona, M.D.; Martínez-Marcos, F.J.; Pérez-Belmonte, L.M.; Hidalgo-Jiménez, A.; Buonaiuto, V.; Suárez Fernández, C.; Freire Castro, S.J.; Luordo, D.; Pesqueira Fontan, P.M.; et al. Admission hyperglycaemia as a predictor of mortality in patients hospitalized with COVID-19 regardless of diabetes status: Data from the Spanish SEMI-COVID-19 Registry. Ann. Med. 2021, 53, 103–116. [Google Scholar] [CrossRef]
- Ali Abdelhamid, Y.; Kar, P.; Finnis, M.E.; Phillips, L.K.; Plummer, M.P.; Shaw, J.E.; Horowitz, M.; Deane, A.M. Stress hyperglycaemia in critically ill patients and the subsequent risk of diabetes: A systematic review and meta-analysis. Crit. Care 2016, 20, 301. [Google Scholar] [CrossRef] [Green Version]
- Jensen, A.V.; Baunbæk Egelund, G.; Bang Andersen, S.; Petersen, P.T.; Benfield, T.; Witzenrath, M.; Rohde, G.; Ravn, P.; Faurholt-Jepsen, D. The Glycemic Gap and 90-Day Mortality in Community-acquired Pneumonia. A Prospective Cohort Study. Ann. Am. Thorac. Soc. 2019, 16, 1518–1526. [Google Scholar] [CrossRef]
- Liao, W.I.; Lin, C.S.; Lee, C.H.; Wu, Y.C.; Chang, W.C.; Hsu, C.W.; Wang, J.C.; Tsai, S.H. An Elevated Glycemic Gap is Associated with Adverse Outcomes in Diabetic Patients with Acute Myocardial Infarction. Sci. Rep. 2016, 6, 27770. [Google Scholar] [CrossRef]
- Donagaon, S.; Dharmalingam, M. Association between Glycemic Gap and Adverse Outcomes in Critically Ill Patients with Diabetes. Indian J. Endocrinol. Metab. 2018, 22, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.J.; Liao, W.I.; Tang, Z.C.; Wang, J.C.; Lee, C.H.; Chang, W.C.; Hsu, C.W.; Tang, S.E.; Tsai, S.H. Glycated hemoglobin A1c-based adjusted glycemic variables in patients with diabetes presenting with acute exacerbation of chronic obstructive pulmonary disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 1923–1932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, T.M.; Levy, J.C.; Matthews, D.R. Use and abuse of HOMA modeling. Diabetes Care 2004, 27, 1487–1495. [Google Scholar] [CrossRef] [Green Version]
- Muniangi-Muhitu, H.; Akalestou, E.; Salem, V.; Misra, S.; Oliver, N.S.; Rutter, G.A. Covid-19 and Diabetes: A Complex Bidirectional Relationship. Front. Endocrinol. 2020, 11, 582936. [Google Scholar] [CrossRef]
- Lim, S.; Bae, J.H.; Kwon, H.S.; Nauck, M.A. COVID-19 and diabetes mellitus: From pathophysiology to clinical management. Nat. Rev. Endocrinol. 2020, 17, 1–20. [Google Scholar] [CrossRef]
- Bode, B.; Garrett, V.; Messler, J.; McFarland, R.; Crowe, J.; Booth, R.; Klonoff, D.C. Glycemic Characteristics and Clinical Outcomes of COVID-19 Patients Hospitalized in the United States. J. Diabetes Sci. Technol. 2020, 14, 813–821. [Google Scholar] [CrossRef] [PubMed]
- Bellaver, P.; Schaeffer, A.F.; Dullius, D.P.; Viana, M.V.; Leitão, C.B.; Rech, T.H. Association of multiple glycemic parameters at intensive care unit admission with mortality and clinical outcomes in critically ill patients. Sci. Rep. 2019, 9, 18498. [Google Scholar] [CrossRef] [PubMed]
- Li, G. Inpatient use of glucocorticoids may mediate the detrimental effect of new-onset hyperglycemia on COVID-19 severity. Diabetes Res. Clin. Pract. 2020, 168, 108441. [Google Scholar] [CrossRef]
- Inagaki, N.; Harashima, S.; Maruyama, N.; Kawaguchi, Y.; Goda, M.; Iijima, H. Efficacy and safety of canagliflozin in combination with insulin: A double-blind, randomized, placebo-controlled study in Japanese patients with type 2 diabetes mellitus. Cardiovasc. Diabetol. 2016, 15, 89. [Google Scholar] [CrossRef] [Green Version]
- Yang, T.; Lu, M.; Ma, L.; Zhou, Y.; Cui, Y. Efficacy and tolerability of canagliflozin as add-on to metformin in the treatment of type 2 diabetes mellitus: A meta-analysis. Eur. J. Clin. Pharmacol. 2015, 71, 1325–1332. [Google Scholar] [CrossRef]
- Monnier, L.; Colette, C.; Thuan, J.F.; Lapinski, H. Insulin secretion and sensitivity as determinants of HbA1c in type 2 diabetes. Eur. J. Clin. Investig. 2006, 36, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Rubino, F.; Amiel, S.A.; Zimmet, P.; Alberti, G.; Bornstein, S.; Eckel, R.H.; Mingrone, G.; Boehm, B.; Cooper, M.E.; Chai, Z.; et al. New-Onset Diabetes in Covid-19. N. Engl. J. Med. 2020, 383, 789–790. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Group | Age (Years) | Gender (Men/Women) | BMI | APACHE II | SOFA | DEX (n) | Smoking | Comorbidities | Death |
|---|---|---|---|---|---|---|---|---|---|
| 1. Ward No Hx of diabetes (n = 75) | 56.3 ± 17.4 * | 50/25 | 25.7 ± 1.8 | N.A. | N.A. | 9 | 15 | Single: 23 More than one: 9 | 2 |
| 2. Ward Hx of diabetes (n = 10) | 59.3 ± 11.9 | 7/3 | 27.8 ± 5.3 | N.A. | N.A. | 1 | 2 | Single: 6 More than one: 4 | 0 |
| 3. ICU No Hx of diabetes (n = 60) | 62.9 ± 11.9 | 44/16 | 26.1 ± 2.4 | 13.7 ± 4.7 | 7.0 ± 2.8 | 36 | 17 | Single: 22 More than one: 12 | 17 |
| 4. ICU Hx of diabetes (n = 12) | 71.8 ± 10.8 | 11/1 | 27.1 ± 1.9 | 16.2 ± 6.1 | 7.4 ± 2.8 | 8 | 4 | Single: 5 More than one: 4 | 5 |
| Group | Glucose (mg/dL) | A1c (%) | GlyG (mg/dL) | Insulin (μU/mL) | C-Peptide (ng/mL) | HOMA2%Bins (%) | HOMA2%Bc-pept (%) | HOMA2%Sins (%) | HOMA2%Sc-pept (%) |
|---|---|---|---|---|---|---|---|---|---|
| 1. Ward No Hx of diabetes (n = 75) | 101 (84/116) * | 5.8 (5.3/6.2) | −14.1 (−38.0/+0.4) | 9.4 (5.9/23.8) | 2.5 (1.6/4.6) | 105.2 ± 63.2 | 128.4 ± 73.7 | 87.9 (47.6/122.4) | 54.0 (35.1/86.2) |
| 2. Ward Hx of diabetes (n = 10) | 136 (113/171) | 7.4 (6.1/11.0) | -5.6 (−29.9/+5.4) | 16.6 (14.9/18.4) | 3.7 (2.8/4.7) | 89.0 ± 84.5 | 100.4 ± 116.5 | 41.9 (39.3/46.9) | 25.5 (19.5/29.8) |
| 3. ICU No Hx of diabetes (n = 60) | 138 (110/184) | 5.8 (5.4/7.1) | +5.7 ** (−10.1/+22.0) | 8.4 (2.8/16.8) | 2.9 (1.5/5.9) | 76.9 ± 63.2+ | 109.9 ± 80.6 | 64.4 (37.8/99.8) | 40.9 (16.8/78.3) |
| 4. ICU Hx of diabetes (n = 12) | 192 (149/275) | 6.1 (5.4/6.5) | +30.2 (+5.5/+74.5) | 16.7 (13.6/19.8) | 3.4 (1.8/4.4) | 44.0 ± 19.0+ | 59.6 ± 65.3 | 37.0 (32.8/50.3) | 27.0 (24.1/124.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilias, I.; Diamantopoulos, A.; Pratikaki, M.; Botoula, E.; Jahaj, E.; Athanasiou, N.; Tsipilis, S.; Zacharis, A.; Vassiliou, A.G.; Vassiliadi, D.A.; et al. Glycemia, Beta-Cell Function and Sensitivity to Insulin in Mildly to Critically Ill Covid-19 Patients. Medicina 2021, 57, 68. https://doi.org/10.3390/medicina57010068
Ilias I, Diamantopoulos A, Pratikaki M, Botoula E, Jahaj E, Athanasiou N, Tsipilis S, Zacharis A, Vassiliou AG, Vassiliadi DA, et al. Glycemia, Beta-Cell Function and Sensitivity to Insulin in Mildly to Critically Ill Covid-19 Patients. Medicina. 2021; 57(1):68. https://doi.org/10.3390/medicina57010068
Chicago/Turabian StyleIlias, Ioannis, Aristidis Diamantopoulos, Maria Pratikaki, Efthymia Botoula, Edison Jahaj, Nikolaos Athanasiou, Stamatios Tsipilis, Alexandros Zacharis, Alice G. Vassiliou, Dimitra A. Vassiliadi, and et al. 2021. "Glycemia, Beta-Cell Function and Sensitivity to Insulin in Mildly to Critically Ill Covid-19 Patients" Medicina 57, no. 1: 68. https://doi.org/10.3390/medicina57010068