Association between Osteoporosis and Cognitive Impairment during the Acute and Recovery Phases of Ischemic Stroke

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
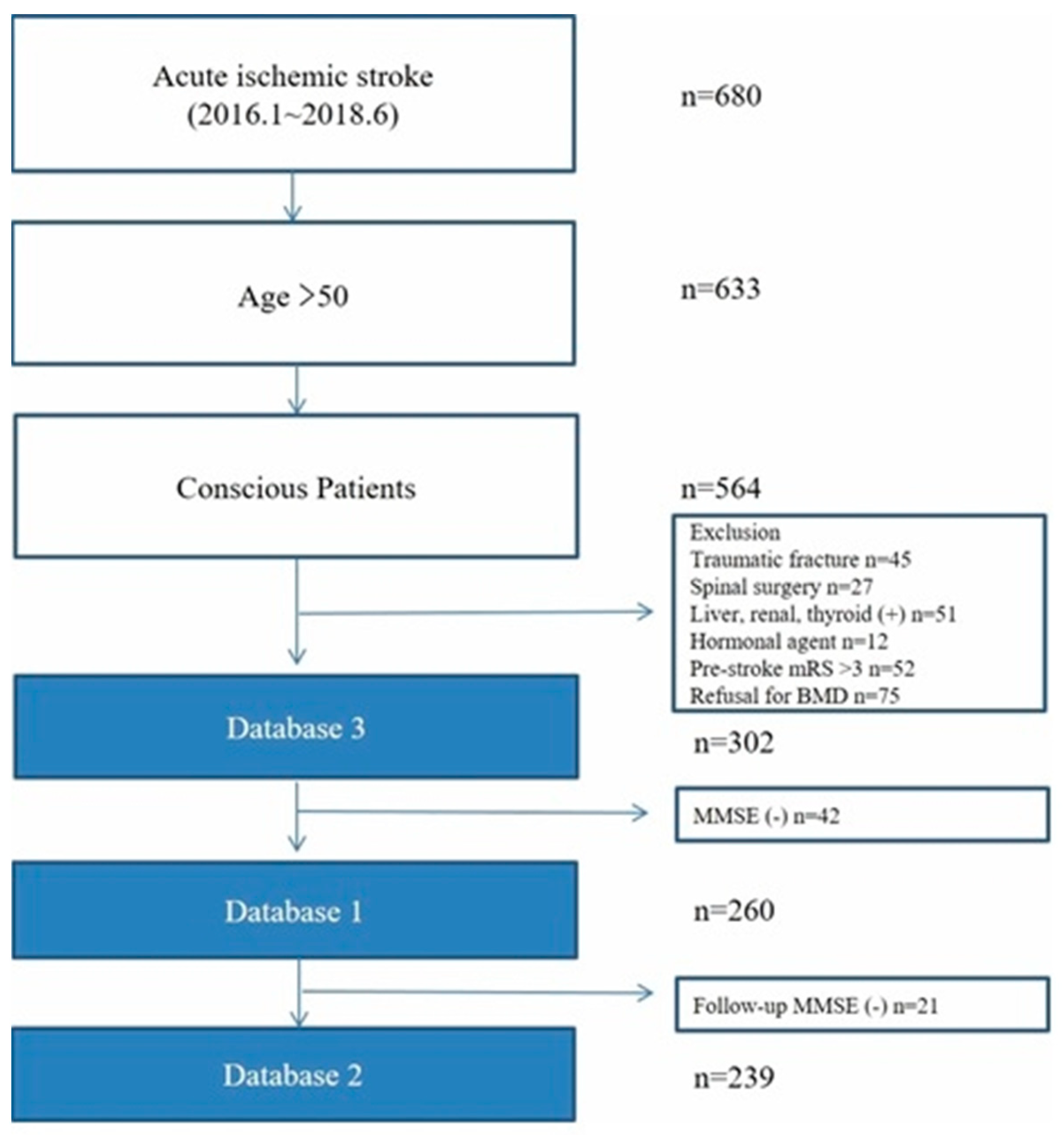
2.1. Study Population
2.2. Data Collection and Outcome Measures
2.3. BMD Measurements
2.4. Cognitive Function Test
2.5. Assessment of WMD
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Osteoporosis and Cognitive Function
3.3. Association between Osteoporosis and Cognitive Function
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Jorgensen, L.; Engstad, T.; Jacobsen, B.K. Bone mineral density in acute stroke patients: Low bone mineral density may predict first stroke in women. Stroke 2001, 32, 47–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.B.; Cho, A.H.; Butcher, K.S.; Kim, T.W.; Ryu, S.Y.; Kim, Y.I. Low bone mineral density is associated with poor clinical outcome in acute ischemic stroke. Int. J. Stroke 2013, 8, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Nordstrom, A.; Eriksson, M.; Stegmayr, B.; Gustafson, Y.; Nordstrom, P. Low bone mineral density is an independent risk factor for stroke and death. Cerebrovasc. Dis. 2010, 29, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Myint, P.K.; Clark, A.B.; Kwok, C.S.; Loke, Y.K.; Yeong, J.K.; Luben, R.N.; Wareham, N.J.; Khaw, K.T. Bone mineral density and incidence of stroke: European prospective investigation into cancer-norfolk population-based study, systematic review, and meta-analysis. Stroke 2014, 45, 373–382. [Google Scholar] [CrossRef] [Green Version]
- Donnan, G.A.; Fisher, M.; Macleod, M.; Davis, S.M. Stroke. Lancet 2008, 371, 1612–1623. [Google Scholar] [CrossRef]
- Watanabe, Y. An assessment of osteoporosis in stroke patients on rehabilitation admission. Int. J. Rehabil. Res. 2004, 27, 163–166. [Google Scholar] [CrossRef] [PubMed]
- Barzilay, J.I.; Buzkova, P.; Fink, H.A.; Cauley, J.A.; Robbins, J.A.; Garimella, P.S.; Jalal, D.I.; Mukamal, K.J. Systemic markers of microvascular disease and bone mineral density in older adults: The cardiovascular health study. Osteoporos. Int. 2016, 27, 3217–3225. [Google Scholar] [CrossRef]
- Minn, Y.K.; Suk, S.H.; Do, S.Y. Osteoporosis as an independent risk factor for silent brain infarction and white matter changes in men and women: The PRESENT project. Osteoporos. Int. 2014, 25, 2465–2469. [Google Scholar] [CrossRef]
- Chutinet, A.; Rost, N.S. White matter disease as a biomarker for long-term cerebrovascular disease and dementia. Curr. Treat. Options Cardiovasc. Med. 2014, 16, 292. [Google Scholar] [CrossRef] [Green Version]
- Jorgensen, L.; Jacobsen, B.K. Changes in muscle mass, fat mass, and bone mineral content in the legs after stroke: A 1 year prospective study. Bone 2001, 28, 655–659. [Google Scholar] [CrossRef]
- Pendlebury, S.T.; Rothwell, P.M. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: A systematic review and meta-analysis. Lancet Neurol. 2009, 8, 1006–1018. [Google Scholar] [CrossRef]
- Ko, Y.; Lee, S.; Chung, J.W.; Han, M.K.; Park, J.M.; Kang, K.; Park, T.H.; Park, S.S.; Cho, Y.J.; Hong, K.S.; et al. MRI-based Algorithm for Acute Ischemic Stroke Subtype Classification. J. Stroke 2014, 16, 161–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broderick, J.P.; Adeoye, O.; Elm, J. Evolution of the Modified Rankin Scale and Its Use in Future Stroke Trials. Stroke 2017, 48, 2007–2012. [Google Scholar] [CrossRef] [PubMed]
- Genant, H.K.; Cooper, C.; Poor, G.; Reid, I.; Ehrlich, G.; Kanis, J.; Nordin, B.E.; Barrett-Connor, E.; Black, D.; Bonjour, J.P.; et al. Interim report and recommendations of the World Health Organization Task-Force for Osteoporosis. Osteoporos. Int. 1999, 10, 259–264. [Google Scholar] [CrossRef]
- Han, C.; Jo, S.A.; Jo, I.; Kim, E.; Park, M.H.; Kang, Y. An adaptation of the Korean mini-mental state examination (K-MMSE) in elderly Koreans: Demographic influence and population-based norms (the AGE study). Arch. Gerontol. Geriatr. 2008, 47, 302–310. [Google Scholar] [CrossRef]
- Nishiwaki, Y.; Breeze, E.; Smeeth, L.; Bulpitt, C.J.; Peters, R.; Fletcher, A.E. Validity of the Clock-Drawing Test as a screening tool for cognitive impairment in the elderly. Am. J. Epidemiol. 2004, 160, 797–807. [Google Scholar] [CrossRef] [PubMed]
- Wahlund, L.O.; Westman, E.; van Westen, D.; Wallin, A.; Shams, S.; Cavallin, L.; Larsson, E.M. From the Imaging Cognitive Impairment Network, Imaging biomarkers of dementia: Recommended visual rating scales with teaching cases. Insights Imaging 2017, 8, 79–90. [Google Scholar] [CrossRef] [Green Version]
- Jung, Y.I.; Jeong, E.H.; Lee, H.; Seo, J.; Yu, H.J.; Hong, J.Y.; Sunwoo, M.K. Validation of MoCA-MMSE Conversion Scales in Korean Patients with Cognitive Impairments. Dement. Neurocogn. Disord. 2018, 17, 148–155. [Google Scholar] [CrossRef]
- Lim, K.B.; Kim, J.; Lee, H.J.; Yoo, J.; You, E.C.; Kang, J. Correlation Between Montreal Cognitive Assessment and Functional Outcome in Subacute Stroke Patients With Cognitive Dysfunction. Ann. Rehabil. Med. 2018, 42, 26–34. [Google Scholar] [CrossRef]
- Bergeron, D.; Flynn, K.; Verret, L.; Poulin, S.; Bouchard, R.W.; Bocti, C.; Fulop, T.; Lacombe, G.; Gauthier, S.; Nasreddine, Z.; et al. Multicenter Validation of an MMSE-MoCA Conversion Table. J. Am. Geriatr. Soc. 2017, 65, 1067–1072. [Google Scholar] [CrossRef]
- Beaupre, G.S.; Lew, H.L. Bone-density changes after stroke. Am. J. Phys. Med. Rehabil. 2006, 85, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Poole, K.E.; Reeve, J.; Warburton, E.A. Falls, fractures, and osteoporosis after stroke: Time to think about protection? Stroke 2002, 33, 1432–1436. [Google Scholar] [CrossRef] [Green Version]
- Seitz, D.P.; Adunuri, N.; Gill, S.S.; Rochon, P.A. Prevalence of dementia and cognitive impairment among older adults with hip fractures. J. Am. Med. Dir. Assoc. 2011, 12, 556–564. [Google Scholar] [CrossRef]
- Sun, J.H.; Tan, L.; Yu, J.T. Post-stroke cognitive impairment: Epidemiology, mechanisms and management. Ann. Transl. Med. 2014, 2, 80. [Google Scholar] [PubMed]
- Simpson, J.E.; Hosny, O.; Wharton, S.B.; Heath, P.R.; Holden, H.; Fernando, M.S.; Matthews, F.; Forster, G.; O’Brien, J.T.; Barber, R.; et al. Microarray RNA expression analysis of cerebral white matter lesions reveals changes in multiple functional pathways. Stroke 2009, 40, 369–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.J.; Zhang, L.; Papasian, C.J.; Deng, H.W. Genome-wide Association Studies for Osteoporosis: A 2013 Update. J. Bone Metab. 2014, 21, 99–116. [Google Scholar] [CrossRef] [Green Version]
- Smith, E.E.; Egorova, S.; Blacker, D.; Killiany, R.J.; Muzikansky, A.; Dickerson, B.C.; Tanzi, R.E.; Albert, M.S.; Greenberg, S.M.; Guttmann, C.R. Magnetic resonance imaging white matter hyperintensities and brain volume in the prediction of mild cognitive impairment and dementia. Arch. Neurol. 2008, 65, 94–100. [Google Scholar] [CrossRef] [Green Version]
- Prins, N.D.; van Dijk, E.J.; den Heijer, T.; Vermeer, S.E.; Koudstaal, P.J.; Oudkerk, M.; Hofman, A.; Breteler, M.M. Cerebral white matter lesions and the risk of dementia. Arch. Neurol. 2004, 61, 1531–1534. [Google Scholar] [CrossRef] [Green Version]
- Meguro, K.; Ishii, H.; Kasuya, M.; Akanuma, K.; Meguro, M.; Kasai, M.; Lee, E.; Hashimoto, R.; Yamaguchi, S.; Asada, T. Incidence of dementia and associated risk factors in Japan: The Osaki-Tajiri Project. J. Neurol. Sci. 2007, 260, 175–182. [Google Scholar] [CrossRef]
- Debette, S.; Beiser, A.; DeCarli, C.; Au, R.; Himali, J.J.; Kelly-Hayes, M.; Romero, J.R.; Kase, C.S.; Wolf, P.A.; Seshadri, S. Association of MRI markers of vascular brain injury with incident stroke, mild cognitive impairment, dementia, and mortality: The Framingham Offspring Study. Stroke 2010, 41, 600–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alissa, E.M.; Alnahdi, W.A.; Alama, N.; Ferns, G.A. Bone mineral density and cardiovascular risk factors in postmenopausal women with coronary artery disease. Bonekey Rep. 2015, 4, 758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uyama, O.; Yoshimoto, Y.; Yamamoto, Y.; Kawai, A. Bone changes and carotid atherosclerosis in postmenopausal women. Stroke 1997, 28, 1730–1732. [Google Scholar] [CrossRef] [PubMed]
- Cummings, S.R.; Bates, D.; Black, D.M. Clinical use of bone densitometry: Scientific review. JAMA 2002, 288, 1889–1897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stojanovic, O.I.; Lazovic, M.; Lazovic, M.; Vuceljic, M. Association between atherosclerosis and osteoporosis, the role of vitamin D. Arch. Med. Sci. 2011, 7, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Barengolts, E.I.; Berman, M.; Kukreja, S.C.; Kouznetsova, T.; Lin, C.; Chomka, E.V. Osteoporosis and coronary atherosclerosis in asymptomatic postmenopausal women. Calcif. Tissue Int. 1998, 62, 209–213. [Google Scholar] [CrossRef]
- Sinnott, B.; Syed, I.; Sevrukov, A.; Barengolts, E. Coronary calcification and osteoporosis in men and postmenopausal women are independent processes associated with aging. Calcif. Tissue Int. 2006, 78, 195–202. [Google Scholar] [CrossRef]
- Tamaki, J.; Iki, M.; Hirano, Y.; Sato, Y.; Kajita, E.; Kagamimori, S.; Kagawa, Y.; Yoneshima, H. Low bone mass is associated with carotid atherosclerosis in postmenopausal women: The Japanese Population-based Osteoporosis (JPOS) Cohort Study. Osteoporos. Int. 2009, 20, 53–60. [Google Scholar] [CrossRef]
- Farhat, G.N.; Cauley, J.A. The link between osteoporosis and cardiovascular disease. Clin. Cases. Miner. Bone Metab. 2008, 5, 19–34. [Google Scholar]
- McGovern, A.; Pendlebury, S.T.; Mishra, N.K.; Fan, Y.; Quinn, T.J. Test Accuracy of Informant-Based Cognitive Screening Tests for Diagnosis of Dementia and Multidomain Cognitive Impairment in Stroke. Stroke 2016, 47, 329–335. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Non-Osteoporosis (n = 190) | Osteoporosis (n = 70) | p-Value | |
|---|---|---|---|
| Age, years (SD) | 71.5 (10.9) | 76.7 (8.4) | 0.06 b |
| Female (%) | 90 (47.4) | 63 (90.0) | <0.001 a |
| BMI, kg/m2 (SD) | 24.4 (4.0) | 22.9 (3.6) | 0.90 b |
| Initial NIHSS score (%) | 0.70 a | ||
| 0–4 | 132 (69.5) | 48 (68.6) | |
| 5–11 | 45 (23.7) | 19 (27.1) | |
| >11 | 13 (6.8) | 3 (4.3) | |
| Stroke mechanisms (%) | 0.44 a | ||
| SVO | 50 (26.3) | 23 (32.9) | |
| LAA | 72 (37.9) | 21 (30.0) | |
| CE | 34 (17.9) | 10 (14.3) | |
| Other | 34 (17.9) | 16 (14.3) | |
| Prior stroke (%) | 46 (24.2) | 20 (28.6) | 0.52 a |
| Hypertension (%) | 121 (63.7) | 49 (70.0) | 0.38 a |
| Diabetes mellitus (%) | 73 (38.4) | 19 (27.1) | 0.11 a |
| Hyperlipidemia (%) | 28 (14.7) | 9 (12.9) | 0.84 a |
| Current smoker (%) | 33 (17.4) | 1 (1.4) | 0.001 a |
| Atrial fibrillation (%) | 38 (20.0) | 12 (17.1) | 0.72 a |
| Prior antithrombotic agent use (%) | 82 (43.2) | 29 (41.4) | 0.89 a |
| Education, years (SD) | 6.9 (4.3) | 6.3 (4.1) | 0.06 b |
| Lesions | 0.64 a | ||
| Supratentorial | 135 (71.1) | 52 (74.3) | |
| Infratentorial | 55 (28.9) | 18 (25.7) | |
| mRS >2 at discharge (%) | 47 (24.7) | 19 (27.1) | 0.75 a |
| mRS >2 at 3 months (%) | 64 (33.7) | 25 (35.7) | 0.77 a |
| MMSE score (IQR) | 22 (14-27) | 18 (11-22) | <0.001 c |
| LDL, mg/dL (SD) | 98.2 (34.5) | 89.4 (28.0) | 0.09 b |
| Creatinine, mg/dL (SD) | 0.97 (0.37) | 1.11 (0.97) | 0.03 b |
| HbA1c, % (SD) | 6.3 (1.4) | 6.2 (1.3) | 0.58 b |
| Mild Cognitive Impairment vs. No Cognitive Impairment | Severe Cognitive Impairment vs. No Cognitive Impairment | |||
|---|---|---|---|---|
| Adjusted OR (95% CI) in the Acute Phase | Adjusted OR (95% CI) in the Recovery Phase | Adjusted OR (95% CI) in the Acute Phase | Adjusted OR (95% CI) in the Recovery Phase | |
| Total BMD T-score < −2.5 a | 2.64 (1.05–6.61) * | 2.90 (0.80–10.52) | 2.22 (0.84–5.86) | 2.55 (0.69–9.51) |
| Femoral neck BMD T-score < −2.5 b | 3.09 (0.87–10.99) | 4.28 (0.43–42.21) | 4.09 (1.11–15.14) * | 11.17 (1.12–110.98) * |
| Lumbar spine BMD T-score < −2.5 a | 1.07 (0.40–2.84) | 2.94 (0.68–12.61) | 0.92 (0.34–2.50) | 1.53 (0.35–6.70) |
| Moderate WMD vs. Normal-to-Mild WMD | Severe WMD vs. Normal-to-Mild WMD | |||
|---|---|---|---|---|
| Adjusted OR (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value | |
| Total BMD T-score < −2.5 a | 1.96 (0.98–3.90) | 0.06 | 1.06 (0.509–2.26) | 0.88 |
| Femoral neck BMD T-score<−2.5 b | 2.71 (1.03–7.15) | 0.04 | 3.13 (1.14–8.60) | 0.03 |
| Lumbar spine BMD T-score < −2.5 a | 1.33 (0.64–2.76) | 0.45 | 0.74 (0.33–1.67) | 0.47 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-H.; Park, S.Y.; Jang, M.U.; Kim, Y.; Lee, J.; Kim, C.; Kim, Y.J.; Sohn, J.-H. Association between Osteoporosis and Cognitive Impairment during the Acute and Recovery Phases of Ischemic Stroke. Medicina 2020, 56, 307. https://doi.org/10.3390/medicina56060307
Lee S-H, Park SY, Jang MU, Kim Y, Lee J, Kim C, Kim YJ, Sohn J-H. Association between Osteoporosis and Cognitive Impairment during the Acute and Recovery Phases of Ischemic Stroke. Medicina. 2020; 56(6):307. https://doi.org/10.3390/medicina56060307
Chicago/Turabian StyleLee, Sang-Hwa, So Young Park, Min Uk Jang, Yerim Kim, Jungyoup Lee, Chulho Kim, Yeo Jin Kim, and Jong-Hee Sohn. 2020. "Association between Osteoporosis and Cognitive Impairment during the Acute and Recovery Phases of Ischemic Stroke" Medicina 56, no. 6: 307. https://doi.org/10.3390/medicina56060307