Global Longitudinal Strain of the Systemic Ventricle Is Correlated with Plasma Galectin-3 and Predicts Major Cardiovascular Events in Adult Patients with Congenital Heart Disease

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Methods
3. Results
3.1. Arrhythmias
3.2. Biomarkers
3.3. Global Longitudinal Strain
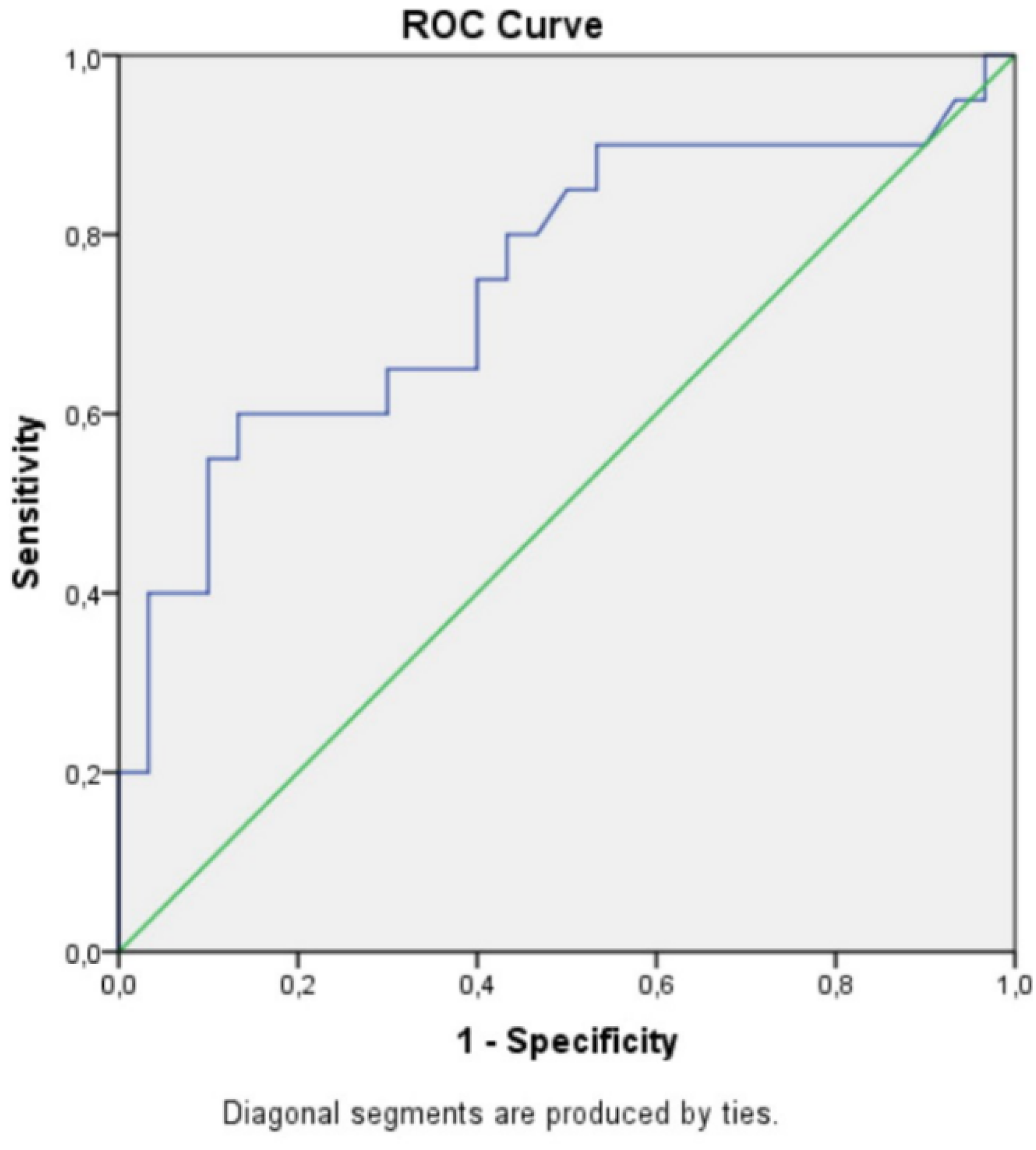
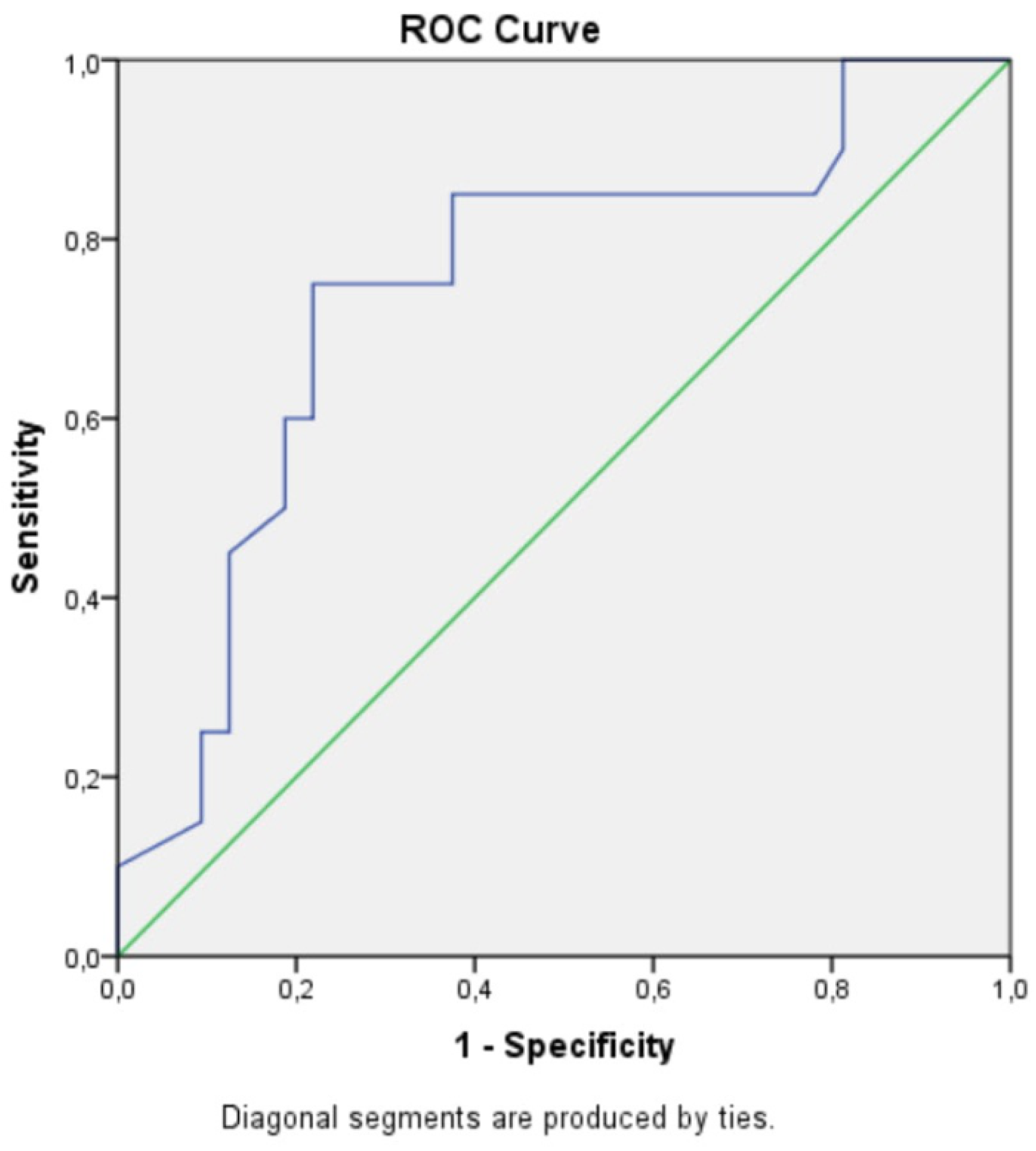
3.4. Clinical Outcomes and Prognostic Associations
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Zomer, A.C.; Vaartjes, I.; Uiterwaal, C.S.; van der Velde, E.T.; van den Merkhof, L.F.; Baur, L.H.; Ansink, T.J.M.; Cozijnsen, L.; Pieper, P.G.; Meijboom, F.J.; et al. Circumstances of death in adult congenital heart disease. Int. J. Cardiol. 2012, 154, 168–172. [Google Scholar] [CrossRef]
- Budts, W.; Roos-Hesselink, J.; Rädle-Hurst, T.; Eicken, A.; McDonagh, T.A.; Lambrinou, E.; Crespo-Leiro, M.G.; Walker, F.; Frogoudaki, A.A. Treatment of heart failure in adult congenital heart disease: A position paper of the Working Group of Grown-Up Congenital Heart Disease and the Heart Failure Association of the European Society of Cardiology. Eur. Heart J. 2016, 37, 1419–1427. [Google Scholar] [CrossRef] [Green Version]
- Walsh, E.P.; Cecchin, F. Arrhythmias in adult patients with congenital heart disease. Circulation 2007, 115, 534–545. [Google Scholar] [CrossRef] [Green Version]
- Besler, C.; Lang, D.; Urban, D.; Rommel, K.-P.; von Roeder, M.; Fengler, K.; Blazek, S.; Kandolf, R.; Klingel, K.; Thiele, H.; et al. Plasma and Cardiac Galectin-3 in Patients with Heart Failure Reflects Both Inflammation and Fibrosis: Implications for Its Use as a Biomarker. Circ. Heart Fail. 2017, 10, e003804. [Google Scholar] [CrossRef] [PubMed]
- Smiseth, O.A.; Torp, H.; Opdahl, A.; Haugaa, K.H.; Urheim, S. Myocardialstrainimaging: How useful is it in clinical decision making? Eur. Heart J. 2016, 37, 1196–1207. [Google Scholar] [CrossRef]
- Spartera, M.; Damascelli, A.; Mozes, F.; De Cobelli, F.; La Canna, G. Three-dimensional speckle tracking longitudinal strain is related to myocardial fibrosis determined by late-gadolinium enhancement. Int. J. Cardiovasc. Imaging 2017, 33, 1351–1360. [Google Scholar] [CrossRef]
- Bax, J.J.; Delgado, V.; Sogaard, P.; Singh, J.P.; Abraham, T.; Borer, S.; Dickstein, K.; Gras, D.; Brugada, J.; Robertson, M.; et al. Prognostic implications of left ventricular globallongitudinalstrain in heart failure patients with narrow QRS complex treated with cardiac resynchronization therapy: A subanalysis of the randomized EchoCRT trial. Eur. Heart J. 2017, 38, 720–726. [Google Scholar]
- Ikonomidis, I.; Tzortzis, S.; Triantafyllidi, H.; Parissis, J.; Papadopoulos, C.; Venetsanou, K.; Trivilou, P.; Paraskevaidis, I.; Lekakis, J. Association of impaired left ventricular twisting-untwisting with vascular dysfunction, neurohumoral activation and impaired exercise capacity in hypertensive heart disease. Eur. J. Heart Fail. 2015, 17, 1240–1251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.J.; Park, J.B.; Park, J.H.; Cho, G.Y. Global Longitudinal Strain to Predict Mortality in Patients with Acute Heart Failure. J. Am. Coll. Cardiol. 2018, 71, 1947–1957. [Google Scholar] [CrossRef]
- Opotowsky, A.R.; Baraona, F.; Owumi, J.; Loukas, B.; Singh, M.N.; Valente, A.M.; Wu, F.; Cheng, S.; Veldtman, G.; Rimm, E.B.; et al. Galectin-3 Is Elevated and Associated with Adverse Outcomes in Patients With Single-Ventricle Fontan Circulation. J. Am. Heart Assoc. 2016, 5, e002706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. SocEchocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baggen, V.J.M.; van den Bosch, A.E.; Eindhoven, J.A.; Menting, M.E.; Witsenburg, M.; Cuypers, J.A.A.E.; Boersma, E.; Roos-Hesselink, J.W. Prognostic value of galectin-3 in adults with congenital heart disease. Heart 2018, 104, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Choi, J.O.; Park, S.W.; Cho, G.-Y.; Oh, J.K.; Lee, J. In-Whan Seong. Normal references of right ventricular strainvalues by two-dimensional strain echocardiography according to the age and gender. Int. J. Cardiovasc. Imaging 2018, 34, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, T.; Dulgheru, R.; Bernard, A.; Ilardi, F.; Contu, L.; Addetia, K.; Caballero, L.; Akhaladze, N.; Athanassopoulos, G.D.; Barone, D.; et al. Echocardiographic reference ranges for normal left ventricular 2D strain: Results from the EACVI NORRE study. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 833–840. [Google Scholar] [CrossRef] [PubMed]
- Hangaa, K.; Dejgaard, L. Global longitudinal strain ready for use and Guideline implementation. J. Am. Coll. Cardiol. 2018, 71, 1958–1959. [Google Scholar]
- Cameli, M.; Mondillo, S.; Righini, F.M.; Lisi, M.; Dokollari, A.; Lindqvist, P.; Maccherini, M.; Henein, M. Left Ventricular Deformation and Myocardial Fibrosis in Patients With Advanced Heart Failure Requiring Transplantation. J. Card Fail. 2016, 22, 901–907. [Google Scholar] [CrossRef]
- Orwat, S.; Diller, G.P.; Kempny, A.; Radke, R.; Peters, B.; Kühne, T.; Boethig, D.; Gutberlet, M.; Dubowy, K.; Beerbaum, P.; et al. Myocardial deformation parameters predict outcome in patients with repaired tetralogy of Fallot. Heart 2016, 102, 209–215. [Google Scholar] [CrossRef]
- Eindhoven, J.A.; Menting, M.E.; van den Bosch, A.E.; McGhie, J.S.; Witsenburg, M.; Cuypers, J.A.A.E.; Boersma, E.; Roos-Hesselink, J.W. Quantitative assessment of systolic right ventricular function using myocardial deformation in patients with a systemic right ventricle. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 380–388. [Google Scholar] [CrossRef] [Green Version]
- DiLorenzo, M.; Okan, E.; Wang, Y.; Banerjee, A.; Sato, T.; Ky, B.; Goldmuntz, E.; Mercer-Rosa, L. Longitudinal Changes in Right Ventricular Function in Tetralogy of Fallot in the Initial Years after Surgical Repair. J. Am. Soc. Echocardiogr. 2018, 31, 816–821. [Google Scholar] [CrossRef]
- Menting, M.E.; van den Bosch, A.E.; McGhie, J.S.; Eindhoven, J.A.; Cuypers, J.A.A.E.; Witsenburg, M.; Geleijnse, M.L.; Helbing, W.A.; Roos-Hesselink, J.W. Assessment of ventricular function in adults with repaired Tetralogy of Fallot usingmyocardial deformationimaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 1347–1357. [Google Scholar]
- Menting, M.E.; van den Bosch, A.E.; McGhie, J.S.; Cuypers, J.A.A.E.; Witsenburg, M.; Geleijnse, M.L.; Helbing, W.A.; Roos-Hesselink, J.W. Ventricular myocardial deformation in adults after early surgical repair of atrial septal defect. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Diller, G.P.; Radojevic, J.; Kempny, A.; Alonso-Gonzalez, R.; Emmanouil, L.; Orwat, S.; Swan, L.; Uebing, A.; Li, W.; Dimopoulos, K.; et al. Systemic right ventricular longitudinal strain is reduced in adults with transposition of the great arteries, relates to subpulmonary ventricular function, and predicts adverse clinical outcome. Am. Heart J. 2012, 163, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Rydman, R.; Gatzoulis, M.A.; Ho, S.Y.; Ernst, S.; Swan, L.; Li, W.; Wong, T.; Sheppard, M.; McCarthy, K.P.; Roughton, M.; et al. Systemic right ventricular fibrosis detected by cardiovascular magnetic resonance is associated with clinical outcome, mainly new-onset atrial arrhythmia, in patients after atrial redirection surgery for transposition of the great arteries. Circ. Cardiovasc. Imaging. 2015, 8, e002628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samyn, M.M.; Yan, K.; Masterson, C.; Goot, B.H.; Saudek, D.; Lavoie, J.; Kinney, A.; Krolikowski, M.; Hor, K.; Cohen, S. Echocardiography vs cardiac magnetic resonance imaging assessment of the systemicright ventricle for patients with d-transposition of the great arteries status post atrial switch. Congenit. Heart Dis. 2019, 14, 1138–1148. [Google Scholar] [CrossRef]
- Diller, G.P.; Kempny, A.; Liodakis, E.; Alonso-Gonzalez, R.; Inuzuka, R.; Uebing, A.; Orwat, S.; Dimopoulos, K.; Swan, L.; Li, W.; et al. Left ventricular longitudinal function predicts life-threatening ventricular arrhythmia and death in adults with repaired tetralogy of Fallot. Circulation 2012, 125, 2440–2446. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Main CHD Diagnosis | N (%) |
|---|---|
| Atrial Septal Defect | 19 (32.7) |
| Ventricular septal defect | 3 (5.2) |
| Aortic stenosis/regurgitation/LVOT abnormality | 3 (5.2) |
| Coarctation of the aorta | 4 (6.9) |
| Pulmonary stenosis | 3 (5.2) |
| Pulmonary regurgitation | 1 (1.7) |
| Tetralogy of Fallot | 14 (24.1) |
| Transposition of the great arteries | 2 (3.4) |
| CC Transposition of the great arteries | 3 (5.2) |
| Single ventricle | 4 (6.9) |
| Eisenmenger syndrome | 2 (3.4) |
| Sex (male), n (%) | 26 (44.8) |
| Age (years) | 37 ± 16.8 |
| NYHA class, n (%) | |
| I | 29 (50) |
| II | 26 (44.8) |
| III | 3 (5.2) |
| Sinus rhythm, n (%) | 52 (89.6) |
| Systemic ventricle, n (%) | |
| LV, n (%) | 49 (84.4) |
| RV, n (%) | 5 (8.6) |
| SiV, n (%) | 4 (6.9) |
| SVEF, % | 55 ± 6 |
| Subpulmonary ventricular pressure, mmHg | 46 ± 22 |
| SVGLS, % | −15,247 ± 4.32 |
| Plasma galectin, ng/mL | 17.07 ± 6.38 |
| NTproBNP, pg/mL (IQR) | 119 (174.3) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frogoudaki, A.A.; Pantelakis, I.; Bistola, V.; Kroupis, C.; Birba, D.; Ikonomidis, I.; Alexopoulos, D.; Filippatos, G.; Parissis, J. Global Longitudinal Strain of the Systemic Ventricle Is Correlated with Plasma Galectin-3 and Predicts Major Cardiovascular Events in Adult Patients with Congenital Heart Disease. Medicina 2020, 56, 305. https://doi.org/10.3390/medicina56060305
Frogoudaki AA, Pantelakis I, Bistola V, Kroupis C, Birba D, Ikonomidis I, Alexopoulos D, Filippatos G, Parissis J. Global Longitudinal Strain of the Systemic Ventricle Is Correlated with Plasma Galectin-3 and Predicts Major Cardiovascular Events in Adult Patients with Congenital Heart Disease. Medicina. 2020; 56(6):305. https://doi.org/10.3390/medicina56060305
Chicago/Turabian StyleFrogoudaki, Alexandra A., Ioannis Pantelakis, Vasiliki Bistola, Christos Kroupis, Dionysia Birba, Ignatios Ikonomidis, Dimitrios Alexopoulos, Gerasimos Filippatos, and John Parissis. 2020. "Global Longitudinal Strain of the Systemic Ventricle Is Correlated with Plasma Galectin-3 and Predicts Major Cardiovascular Events in Adult Patients with Congenital Heart Disease" Medicina 56, no. 6: 305. https://doi.org/10.3390/medicina56060305