Pregnancy and Childbirth in Uterus Didelphys: A Report of Three Cases




Abstract
:1. Introduction
2. Case Reports
2.1. Case 1
2.2. Case 2
2.3. Case 3
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Venetis, C.; Papadopoulos, S.P.; Campo, R.; Gordts, S.; Tarlatzis, B.C.; Grimbizis, G.F. Clinical implications of congenital uterine anomalies: A meta-analysis of comparative studies. Reprod. Biomed. Online 2014, 29, 665–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, Y.; Jayaprakasan, K.; Zamora, J.; Thornton, J.G.; Raine-Fenning, N.; Coomarasamy, A. The prevalence of congenital uterine anomalies in unselected and high-risk populations: A systematic review. Hum. Reprod. Update 2011, 17, 761–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, K.L.; Persaud, T.V.N.; Torchia, M.G. The Urogenital System. In Before We Are Born: Essential of Embryology and Birth Defects, 7th ed.; Saunders/Elsevier: Philadelphia, PA, USA, 2008; pp. 162–189. [Google Scholar]
- Chan, Y.Y.; Jayaprakasan, K.; Tan, A.; Thornton, J.G.; Coomarasamy, A.; Raine-Fenning, N.J. Reproductive outcomes in women with congenital uterine anomalies: A systematic review. Ultrasound Obstet. Gynecol. 2011, 38, 371–382. [Google Scholar] [CrossRef] [PubMed]
- The American Fertility Society. The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, Mullerian anomalies and intrauterine adhesions. Fertil. Steril. 1988, 49, 944–955. [Google Scholar] [CrossRef]
- Grimbizis, G.F.; Gordts, S.; Sardo, A.D.S.; Brucker, S.; De Angelis, C.; Gergolet, M.; Li, T.-C.; Tanos, V.; Brölmann, H.; Gianaroli, L.; et al. The ESHRE/ESGE consensus on the classification of female genital tract congenital anomalies. Hum. Reprod. 2013, 28, 2032–2044. [Google Scholar] [CrossRef] [PubMed]
- Laufer, M.R.; De Cherney, A.H. Clinical Manifestations and Diagnosis of Congenital Anomalies of the Uterus; UpToDate: Waltham, MA, USA; Wolters Kluwer: South Holland, The Netherlands, 2019. [Google Scholar]
- Kiserud, T.; Piaggio, G.; Carroli, G.; Widmer, M.; Carvalho, J.; Jensen, L.N.; Giordano, D.; Cecatti, J.G.; Aleem, H.A.; Talegawkar, S.A.; et al. The World Health Organization fetal growth charts: A multinational longitudinal study of ultrasound biometric measurements and estimated fetal weight. PLoS Med. 2017, 14, e1002220. [Google Scholar]
- Bishop, E.H. Pelvic Scoring for Elective Induction. Obstet Gynecol. 1964, 24, 14199536. [Google Scholar]
- Grimbizis, G.F.; Camus, M.; Tarlatzis, B.C.; Bontis, J.N.; Devroey, P. Clinical implications of uterine malformations and hysteroscopic treatment results. Hum. Reprod. Update 2001, 7, 161–174. [Google Scholar] [CrossRef] [PubMed]
- Rezai, S.; Bisram, P.; Alcantara, I.L.; Upadhyay, R.; Lara, C.; Elmadjian, M. Didelphys Uterus: A Case Report and Review of the Literature. Case Rep. Obstet. Gynecol. 2015, 2015, 865821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukunaga, T.; Fujii, S.; Inoue, C.; Mukuda, N.; Murakami, A.; Tanabe, Y.; Harada, T.; Ogawa, T. The spectrum of imaging appearances of müllerian duct anomalies: Focus on MR imaging. Jpn. J. Radiol. 2017, 35, 697–706. [Google Scholar] [CrossRef] [PubMed]
- Heinonen, P.K. Clinical implications of the didelphic uterus: Long-term follow-up of 49 cases. Eur. J. Obstet. Gynecol. Reprod. Boil. 2000, 91, 183–190. [Google Scholar] [CrossRef]
- Pankaja, S.; Ip, P.; O’Mahony, F. Successful Pregnancy with Uterus Didelphys. J. Androl. Gynaecol. 2016, 4, 3. [Google Scholar]
- Hua, M.; Odibo, A.O.; Longman, R.E.; Macones, G.A.; Roehl, K.A.; Cahill, A.G. Congenital uterine anomalies and adverse pregnancy outcomes. Am. J. Obstet. Gynecol. 2011, 205, 558.e1–558.e5. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhao, Y.-Y.; Qiao, J. Obstetric outcome of women with uterine anomalies in China. Chin. Med. J. 2010, 123, 418–422. [Google Scholar]
- Gudu, W.; Barsenga, M. Uterus Didelphys with Term Pregnancy Diagnosed in Labor as a Cause of Dystocia: Case Report. EJRH 2020, 12, 55–59. [Google Scholar]
- Othman, M. Uterine Didelphys Pregnancy Management. J. Adv. Med. Med. Res. 2018, 26, 1–5. [Google Scholar] [CrossRef]
- Altwerger, G.; Pritchard, A.M.; Black, J.D.; Sfakianaki, A.K. Uterine Didelphys and Vaginal Birth after Cesarean Delivery. Obstet. Gynecol. 2015, 125, 157–159. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Uterine Anomaly | Cervical/Vaginal Anomaly | |
|---|---|---|
| Main Class | Main Sub-Class | Co-Existent Class |
| Class 0 Normal uterus Class I Dysmorphic uterus Class II Septate uterus Class III Bicorporeal uterus Class IV Hemi-uterus Class V Aplastic Class VI Unclassified malformations | a. T-shaped b. Infantilis c. Others a. Partial b. Complete a. Partial b. Complete c. Bicorporeal septate a. With rudimentary cavity (communicating or not horn) b. Without rudimentary cavity (horn without cavity/no horn) a. With rudimentary cavity (bi- or unilateral horn) b. Without rudimentary cavity (bi- or unilateral uterine remnants/aplasia) | C0: Normal cervix C1: Septate cervix C2: Double ‘normal’ cervix C3: Unilateral cervical aplasia C4: Cervical aplasia V0: Normal vagina V1: Longitudinal non-obstructing vaginal septum V2: Longitudinal obstructing vaginal septum V3: Transverse vaginal septum and/or imperforate hymen V4: Vaginal aplasia |
| Case 1 | Case 2 | Case 3 | |
|---|---|---|---|
| Maternal age at booking | 21 | 25 | 27 |
| Parity | Primipara | Primipara | Multipara |
| Prenatal complications | No | No | No |
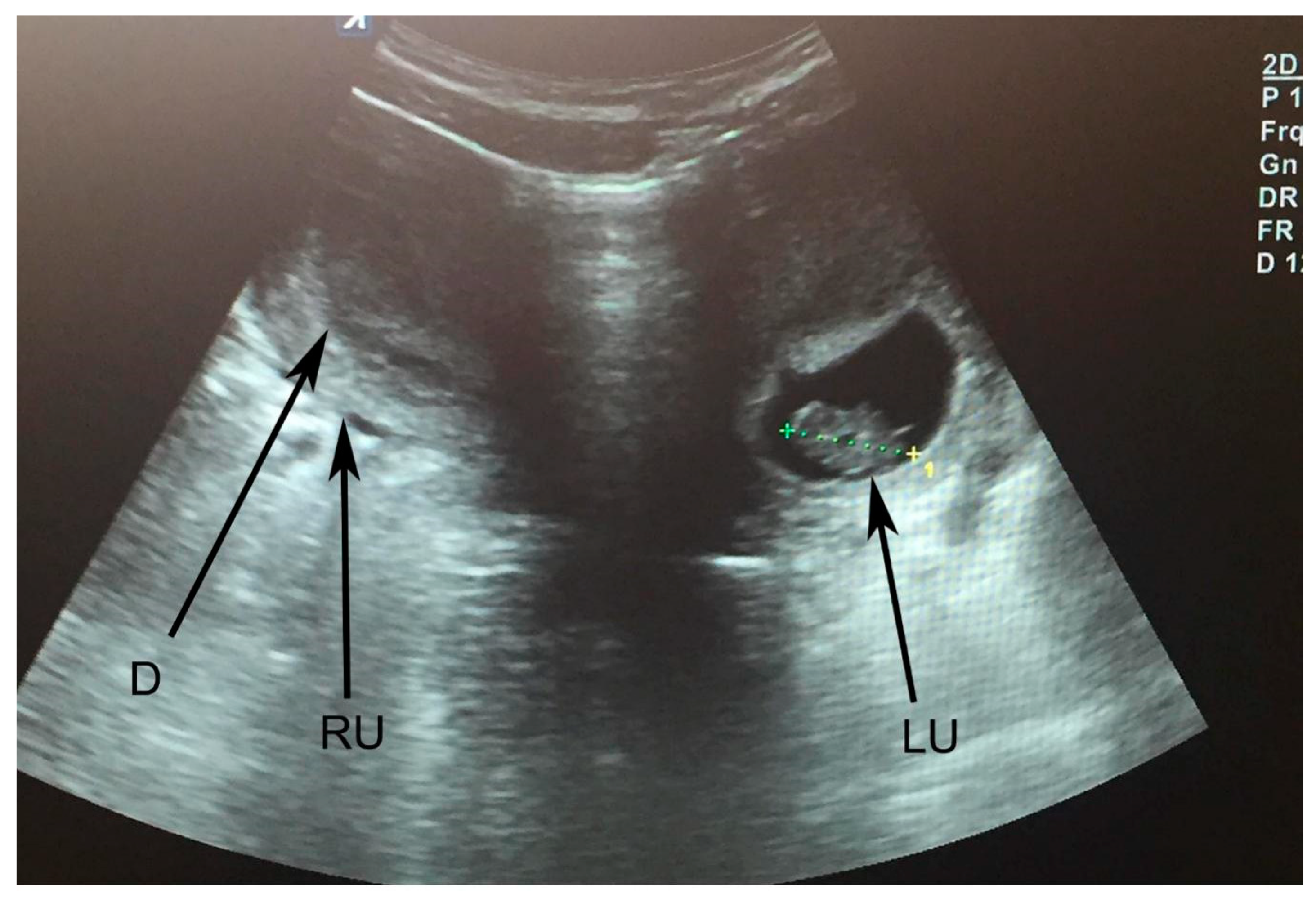
| Prenatal USG | Pregnancy at left uterus; no kidney anomalies | Pregnancy at left uterus; no kidney anomalies | Pregnancy at right uterus; no kidney anomalies |
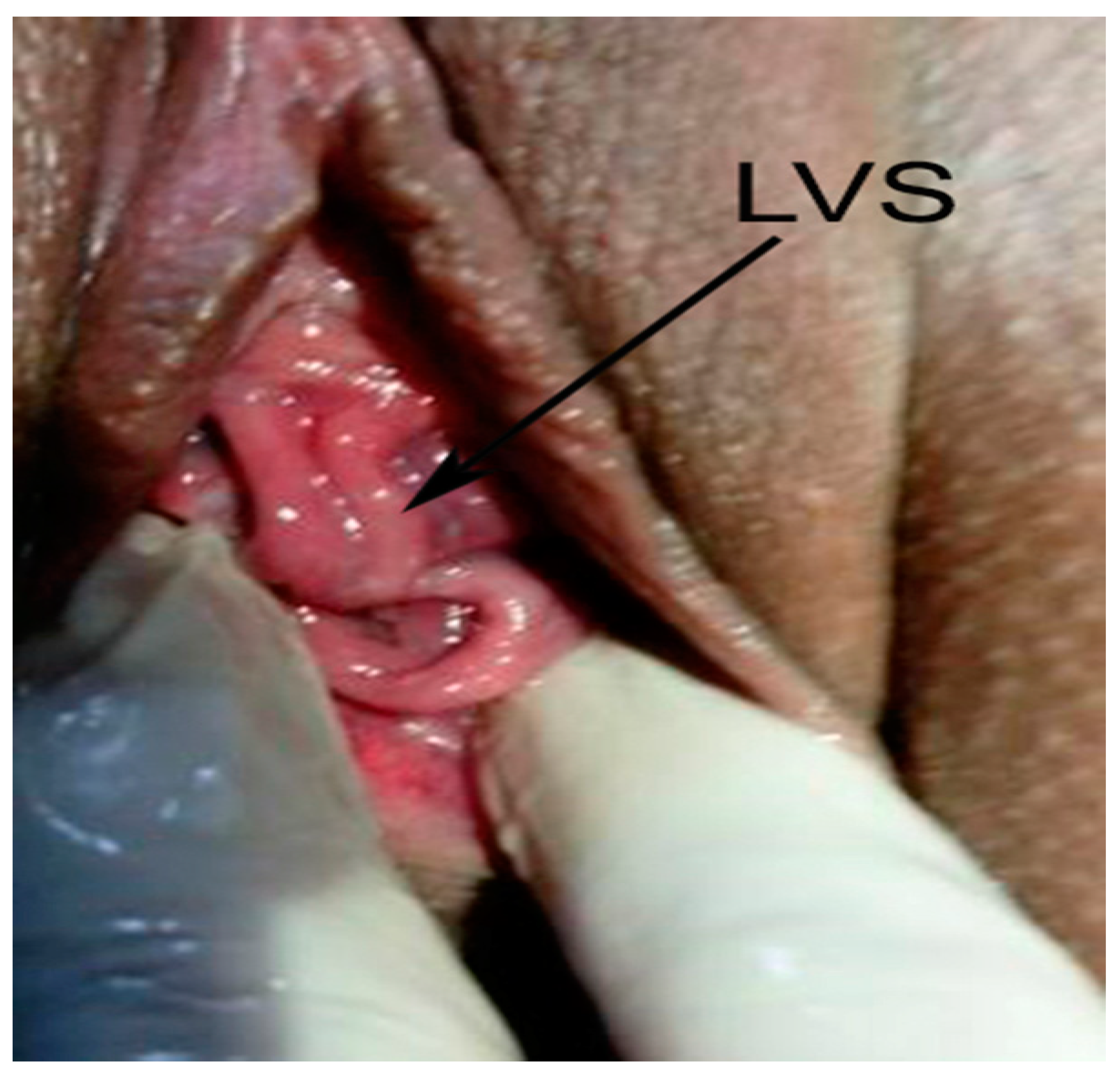
| Vaginal septum | Longitudinal | No | Longitudinal |
| Miscarriages | First pregnancy-missed abortion at two uterine cavities | No | First pregnancy-spontaneous abortion at 7 weeks |
| Gestation at delivery | 38 weeks | 39 weeks | 38 weeks |
| Type of delivery | Emergency CS | Emergency CS | Vaginal |
| Malpresentation at delivery | Cephalic | Cephalic | Cephalic |
| Birth weight | 2580 g | 2730 g | 3250 g |
| Apgar score | 9–10 | 9–10 | 9–10 |
| Complications at postpartum period | No | No | Pain in the ascending colon, No acute abdomen |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Slavchev, S.; Kostov, S.; Yordanov, A. Pregnancy and Childbirth in Uterus Didelphys: A Report of Three Cases. Medicina 2020, 56, 198. https://doi.org/10.3390/medicina56040198
Slavchev S, Kostov S, Yordanov A. Pregnancy and Childbirth in Uterus Didelphys: A Report of Three Cases. Medicina. 2020; 56(4):198. https://doi.org/10.3390/medicina56040198
Chicago/Turabian StyleSlavchev, Stanislav, Stoyan Kostov, and Angel Yordanov. 2020. "Pregnancy and Childbirth in Uterus Didelphys: A Report of Three Cases" Medicina 56, no. 4: 198. https://doi.org/10.3390/medicina56040198