Gait Training Using the Honda Walking Assistive Device® in a Patient Who Underwent Total Hip Arthroplasty: A Single-Subject Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Case Presentation
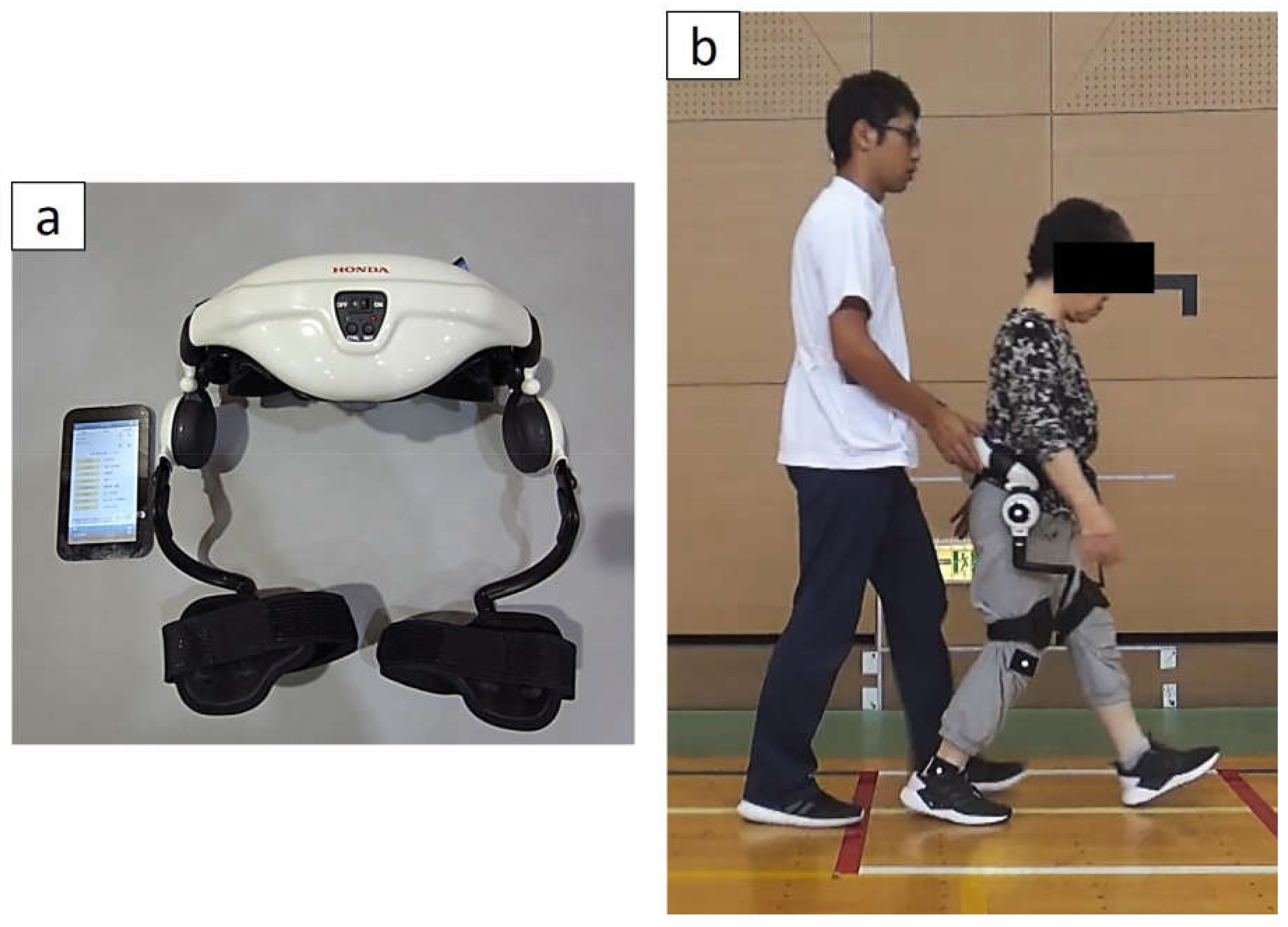
2.2. HWA Intervention
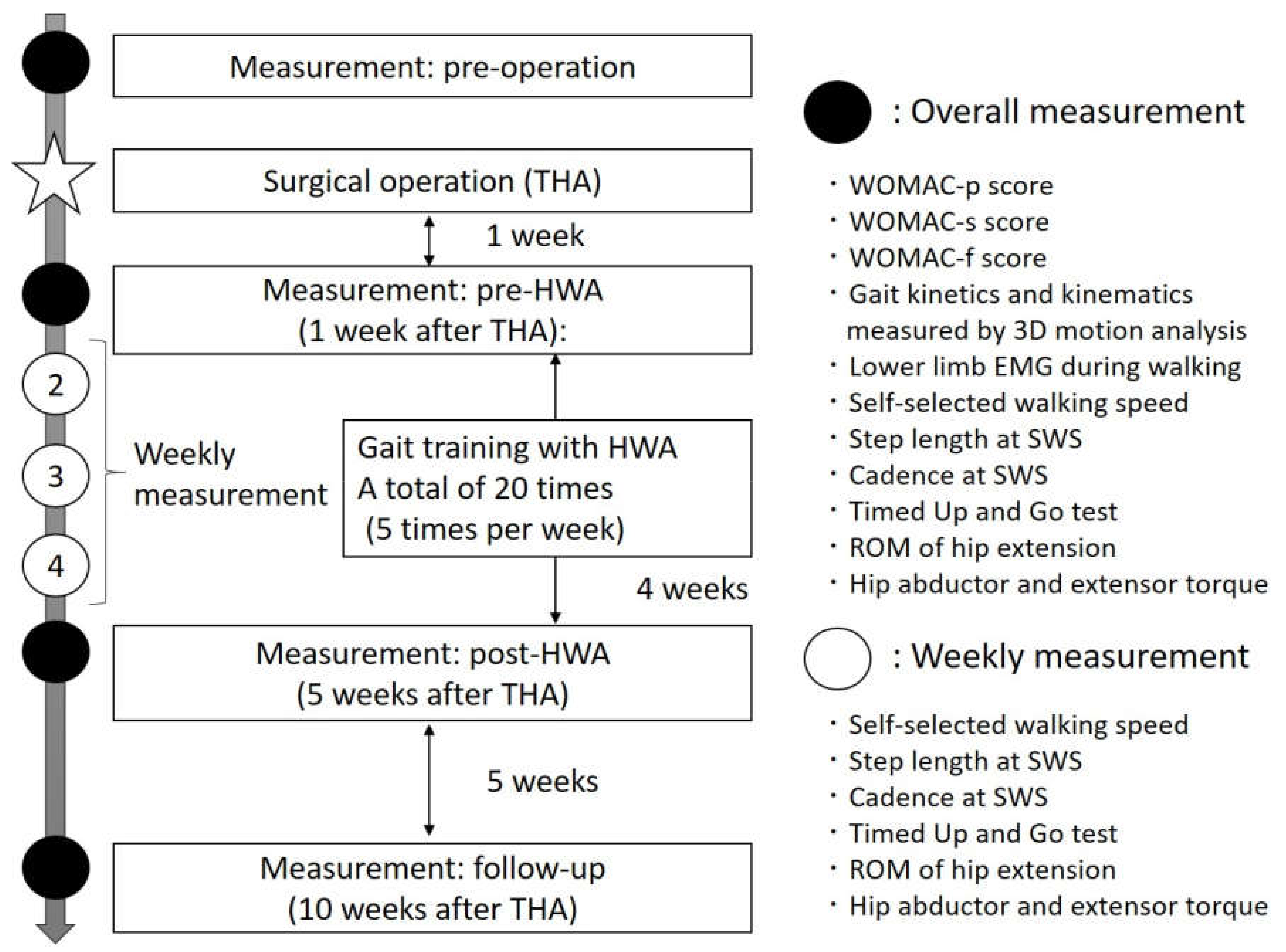
2.3. Outcome Measures
2.4. Gait Analysis Using Three-Dimensional (3D) Gait Analysis and EMG
3. Results
3.1. Gait Ability and Hip Function Parameters
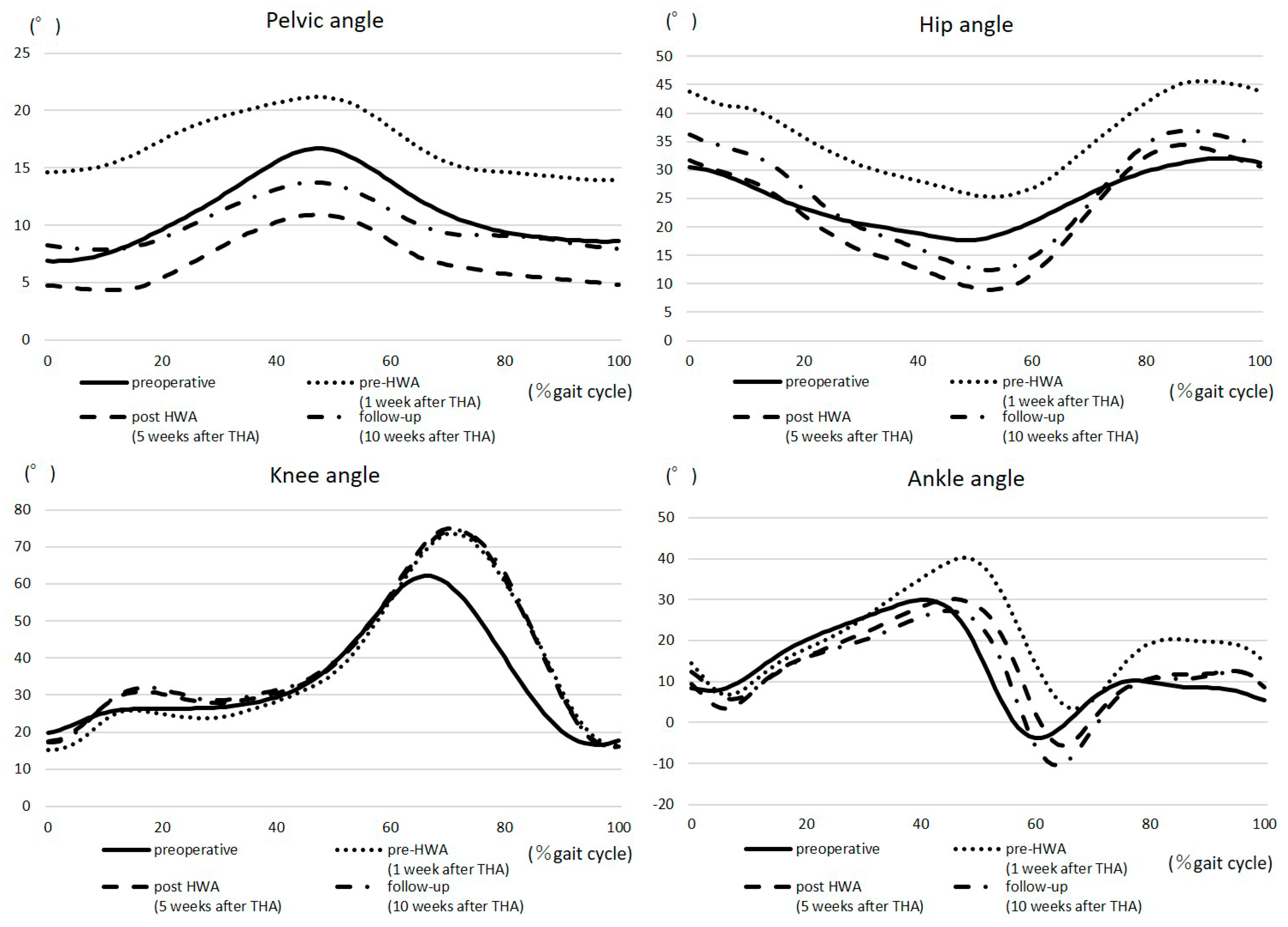
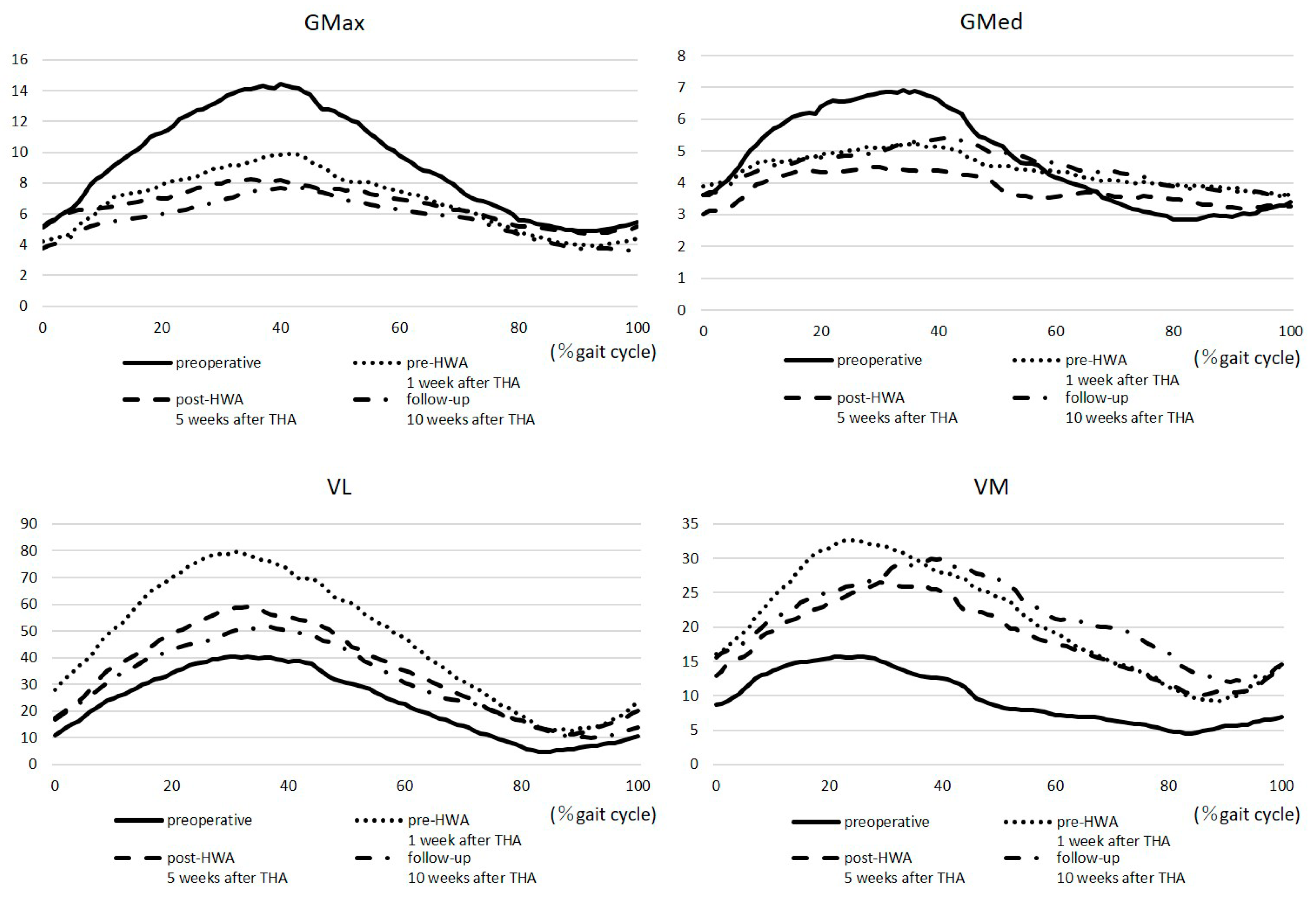
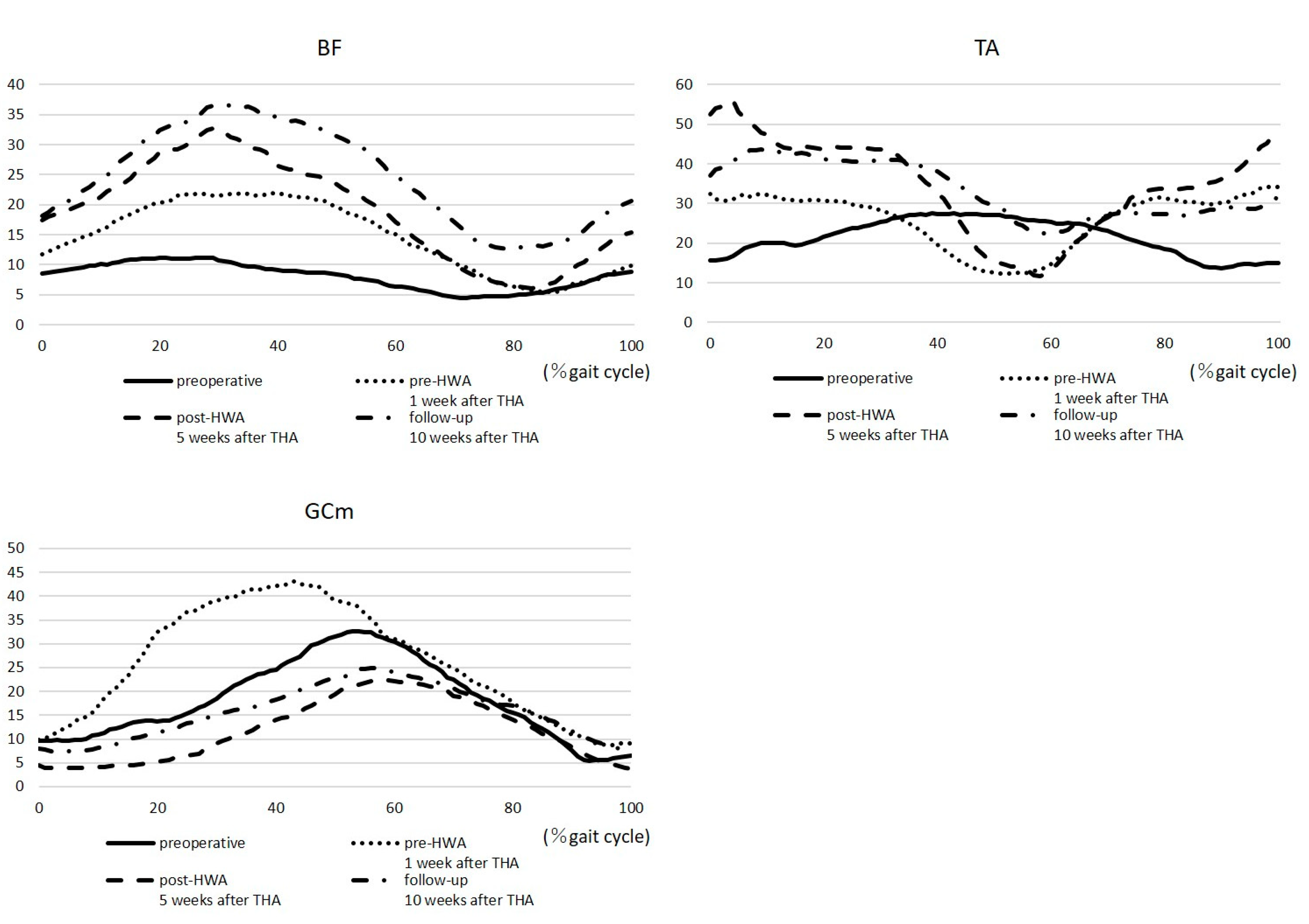
3.2. Gait Kinematic Parameters and iEMG
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Herberts, P.; Malchau, H. Long-term registration has improved the quality of hip replacement: A review of the Swedish THR Register comparing 160,000 cases. Acta Orthop. Scand. 2000, 71, 111–121. [Google Scholar] [CrossRef]
- Wylde, V.; Blom, A.W.; Whitehouse, S.L.; Taylor, A.H.; Pattison, G.T.; Bannister, G.C. Patient-reported outcomes after total hip and knee arthroplasty. comparison of midterm results. J. Arthroplast. 2009, 24, 210–216. [Google Scholar] [CrossRef]
- Cowie, J.G.; Turnball, G.S.; Ker, A.M.; Breusch, S.J. Return to work and sports after total hip replacement. Arch. Orthop. Trauma Surg. 2013, 133, 695–700. [Google Scholar] [CrossRef]
- Rapp, W.; Brauner, T.; Weber, L.; Grau, S.; Mündermann, A.; Horstmann, T. Improvement of walking speed and gait symmetry in older patients after hip arthroplasty: A prospective cohort study. BMC Musculoskelet. Disord. 2015, 16, 1–8. [Google Scholar] [CrossRef]
- Murray, M.P.; Gore, D.R.; Brewer, B.J.; Gardner, G.M.; Sepic, S.B. A comparison of the funtional performance of patients with Charnley and Müller total hip replacement. A two-year follow-up of eighty-nine cases. Acta Orthop. Scand. 1979, 50, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Miki, H.; Sugano, N.; Hagio, K.; Nishii, T.; Kawakami, H.; Kakimoto, A.; Nakamura, N.; Yoshikawa, H. Recovery of walking speed and symmetrical movement of the pelvis and lower extremity joints after unilateral THA. J. Biomech. 2004, 37, 443–455. [Google Scholar] [CrossRef] [PubMed]
- Bennett, D.; Humphreys, L.; O’Brien, S.; Kelly, C.; Orr, J.F.; Beverland, D.E. Gait kinematics of age-stratified hip replacement patients—A large scale, long-term follow-up study. Gait Posture 2008, 28, 194–200. [Google Scholar] [CrossRef]
- Colgan, G.; Walsh, M.; Bennett, D.; Rice, J.; O’Brien, T. Gait analysis and hip extensor function early post total hip replacement. J. Orthop. 2016, 13, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Kolk, S.; Minten, M.J.M.; Van Bon, G.E.A.; Rijnen, W.H.; Geurts, A.C.; Verdonschot, N.; Weerdesteyn, V. Gait and gait-related activities of daily living after total hip arthroplasty: A systematic review. Clin. Biomech. 2014, 29, 705–718. [Google Scholar] [CrossRef] [PubMed]
- Bennett, D.; Ryan, P.; O’Brien, S.; Beverland, D.E. Gait kinetics of total hip replacement patients—A large scale, long-term follow-up study. Gait Posture 2017, 53, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Beaulieu, M.L.; Lamontagne, M.; Beaulé, P.E. Lower limb biomechanics during gait do not return to normal following total hip arthroplasty. Gait Posture 2010, 32, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Yue, Z.; Wang, J. Robotics in lower-limb rehabilitation after stroke. Behav. Neurol. 2017, 2017, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Holanda, L.J.; Silva, P.M.M.; Amorim, T.C.; Lacerda, M.O.; Simão, C.R.; Morya, E. Robotic assisted gait as a tool for rehabilitation of individuals with spinal cord injury: A systematic review. J. Neuroeng. Rehabil. 2017, 14, 126. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, I.; Pinto, S.M.; Chagas, D.D.V.; Praxedes dos Santos, J.L.; de Sousa Oliveira, T.; Batista, L.A. Robotic gait training for individuals with cerebral palsy: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2017, 98, 2332–2344. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, K.; Mutsuzaki, H.; Sano, A.; Koseki, K.; Fukaya, T.; Mizukami, M.; Yamazaki, M. Training with Hybrid Assistive Limb for walking function after total knee arthroplasty. J. Orthop. Surg. Res. 2018, 13, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Steffen, T.M.; Hacker, T.; Mollinger, L. Age- and gender-related test performance in community dwellingelderly people: Six minute walk test, berg balance scale, timed up and go test, and gait speed. Phys. Ther. 2002, 82, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Dwyer, M.K.; Stafford, K.; Mattacola, C.G.; Uhl, T.L.; Giordani, M. Comparison of gluteus medius muscle activity during functional tasks in individuals with and without osteoarthritis of the hip joint. Clin. Biomech. 2013, 28, 757–761. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Preoperative | Pre-HWA | Post-HWA | Follow-Up | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 1 Week | 2 Weeks | 3 Weeks | 4 Weeks | 5 Weeks | 10 Weeks | After THA | |||
| ROM of hip extension at the operative side | (°) | −10 | −25 | −15 | −10 | −10 | −5 | 0 | |
| Hip abductor torque at the operative side | (Nm/kg) | 0.35 | 0.68 | 0.79 | 0.76 | 0.65 | 0.92 | 0.80 | |
| Hip abductor torque at the non-operative side | (Nm/kg) | 0.52 | 0.91 | 0.82 | 0.85 | 0.76 | 0.88 | 0.96 | |
| Hip extensor torque at the operative side | (Nm/kg) | 0.81 | 0.93 | 1.55 | 1.60 | 1.34 | 1.56 | 1.59 | |
| Hip extensor torque at the non-operative side | (Nm/kg) | 0.82 | 1.17 | 1.37 | 1.68 | 1.70 | 1.59 | 1.62 | |
| Timed Up and Go (TUG) test | (s) | 11.3 | 12.7 | 9.9 | 9.7 | 9.7 | 9.6 | 9.7 | |
| Gait speed at SWS | (m/s) | 1.05 | 1.20 | 1.31 | 1.35 | 1.31 | 1.36 | 1.33 | |
| Step length at SWS | (m) | 0.50 | 0.58 | 0.58 | 0.59 | 0.59 | 0.61 | 0.56 | |
| Cadence at SWS | (step/min) | 126.1 | 124.7 | 136.6 | 138.0 | 134.1 | 133.0 | 143.9 | |
| WOMAC-p | 10 | 5 | 0 | 0 | |||||
| WOMAC-s | 5 | 2 | 2 | 3 | |||||
| WOMAC-f | 42 | 28 | 19 | 5 |
| (°) | Normal [8] | Preoperative | Pre-HWA | Post-HWA | Follow-Up | |
|---|---|---|---|---|---|---|
| 1 Week | 5 Weeks | 10 Weeks | After THA | |||
| Maximum anterior pelvic tilt | 9.2 | 16.7 | 21.2 | 10.9 | 13.7 | |
| Minimum anterior pelvic tilt | 4.4 | 6.9 | 13.9 | 4.3 | 7.9 | |
| Pelvic tilt range | 4.8 | 9.8 | 7.3 | 6.6 | 5.9 | |
| Maximum hip flexion | 33.4 | 30.4 | 45.7 | 34.4 | 36.9 | |
| Maximum hip extension in stance | 9.0 | −17.7 | −25.3 | −8.9 | −12.4 | |
| Hip range | 42.4 | 12.8 | 20.4 | 25.4 | 24.5 | |
| Maximum knee flexion | 64.6 | 62.1 | 73.6 | 75.0 | 74.5 | |
| Maximum knee extension | 0.8 | −16.5 | −15.2 | −15.8 | −16.2 | |
| Knee range | 65.4 | 45.6 | 58.5 | 59.2 | 58.3 | |
| Maximum ankle dorsiflexion | 13.9 | 3.8 | -3.4 | 5.6 | 10.4 | |
| Maximum ankle plantarflexion | 24.3 | 29.8 | 40.2 | 30.1 | 27.2 | |
| Ankle range | 38.1 | 33.6 | 36.8 | 35.7 | 37.6 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koseki, K.; Mutsuzaki, H.; Yoshikawa, K.; Endo, Y.; Maezawa, T.; Takano, H.; Yozu, A.; Kohno, Y. Gait Training Using the Honda Walking Assistive Device® in a Patient Who Underwent Total Hip Arthroplasty: A Single-Subject Study. Medicina 2019, 55, 69. https://doi.org/10.3390/medicina55030069
Koseki K, Mutsuzaki H, Yoshikawa K, Endo Y, Maezawa T, Takano H, Yozu A, Kohno Y. Gait Training Using the Honda Walking Assistive Device® in a Patient Who Underwent Total Hip Arthroplasty: A Single-Subject Study. Medicina. 2019; 55(3):69. https://doi.org/10.3390/medicina55030069
Chicago/Turabian StyleKoseki, Kazunori, Hirotaka Mutsuzaki, Kenichi Yoshikawa, Yusuke Endo, Takayuki Maezawa, Hanako Takano, Arito Yozu, and Yutaka Kohno. 2019. "Gait Training Using the Honda Walking Assistive Device® in a Patient Who Underwent Total Hip Arthroplasty: A Single-Subject Study" Medicina 55, no. 3: 69. https://doi.org/10.3390/medicina55030069