Migraine without Aura and Subclinical Atherosclerosis in Young Females: Is Gut Microbiota to Blame?



Abstract
:1. Introduction
2. Materials and Methods
2.1. Methodology Addressing the Primary Aim
2.1.1. Selection of Candidates for the Study
2.1.2. Migraine Diagnostics
2.1.3. Assessment of Migraine Attack Severity
2.1.4. Assessment of Gut Microbiota and Confirmation of Dysbiosis
2.1.5. Imaging Subclinical Atherosclerosis by Carotid Intima-Media Thickness
2.2. Methodology Addressing the Secondary Aim
2.2.1. Assessment of Body Mass Index (BMI)
2.2.2. Blood Pressure (BP) Measurements
2.2.3. Blood, Urine and Stool Work Ups
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kurth, T.; Chabriat, H.; Bousser, M.G. Migraine and stroke a complex association with clinical implications. Lancet Neurol. 2012, 11, 92–100. [Google Scholar] [CrossRef]
- Sacco, S.; Ornello, R.; Ripa, P.; Pistoia, F.; Carolei, A. Migraine and hemorrhagic stroke: A meta-analysis. Stroke 2013, 44, 3032–3038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurth, T.; Winter, A.C.; Dushkes, R.; Mukamal, K.J.; Rimm, E.B.; Willett, W.C.; Manson, J.E.; Rexrode, K.M. Migraine and risk of cardio-vascular disease in women: Prospective cohort study. BMJ 2016, 353, i2610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bigal, M.E.; Kurth, T.; Santanello, N.; Buse, D.; Golden, W.; Robbins, M.; Lipton, R.B. Migraine and cardiovascular disease: A population-based study. Neurology 2010, 74, 628–635. [Google Scholar] [CrossRef] [Green Version]
- Winsvold, B.S.; Hagen, K.; Aamodt AHStovner, L.J.; Holmen, J.; Zwart, J.A. Headache, migraine and cardiovascular risk factors: The HUNT study. Eur. J. Neurol. 2011, 18, 504–511. [Google Scholar] [CrossRef]
- Glass, C.K.; Witztum, J.L. Atherosclerosis. The road ahead. Cell 2001, 104, 503–516. [Google Scholar] [CrossRef] [Green Version]
- Taylor, A.J.; Burke, A.P.; O’Maley, P.G.; Farb, A.; Malcom, G.T.; Smialek, J.; Virmani, R. A comparison of the Framingham risk index, coronary artery calcification and culprit plaque morphology in sudden cardiac death. Circulation 2000, 101, 1243–1248. [Google Scholar] [CrossRef]
- Michos, E.D.; Nasir, K.; Braunstein, J.B.; Rumberger, J.A.; Budoff, M.J.; Post, W.S.; Blumenthal, R.S.L. Framingham risk equation underestimates subclinical atherosclerosis risk in asymptomatic women. Atherosclerosis 2016, 184, 201–206. [Google Scholar] [CrossRef]
- Fernandez-Friera, R.; Fuster, V.; Lopez-Melgar, B.; Oliva, B.; García-Ruiz, J.M.; Mendiguren, J.; Bueno, H.; Pocock, S.; Ibáñez, B.; Fernández-Ortiz, A.; et al. Normal LDL-cholesterol levels are associated with subclinical atherosclerosis in the absence of risk factors. J. Am. Coll. Cardiol. 2017, 70, 2979–2991. [Google Scholar] [CrossRef]
- Libby, P. Inflammation in atherosclerosis. Nature 2002, 420, 868–874. [Google Scholar] [CrossRef]
- Hansson, G.K. Inflammation, atherosclerosis and coronary artery disease. N. Engl. J. Med. 2005, 352, 1685–1695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, L.A.; Rosenfeld, E. Infection and ATS development. Arch. Med. Res. 2015, 46, 339–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindskog, A.; Bäckhed, J.F. Role of gut microbiota in atherosclerosis. Nat. Rev. Cardiol. 2017, 14, 79–87. [Google Scholar]
- Wang, Z.; Klipfell, E.; Bennett, B.J.; Koeth, R.; Levison, B.S.; DuGar, B.; Feldstein, A.E.; Britt, E.B.; Fu, X.; Chung, Y.M.; et al. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature 2011, 472, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Lau, K.; Srivatsav, V.; Rizwan, A.; Nashed, A.; Liu, R.; Shen, R.; Akhtar, M. Bridging the gap between gut microbial dysbiosis and cardiovascular diseases. Nutrients 2017, 9, 859. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Li, H. The role of gut microbiota in atherosclerosis and hypertension. Front. Pharm. 2018, 9, 1082. [Google Scholar] [CrossRef]
- Li, X.; Shimizu, Y.; Kimura, I. Gut microbial metabolite short-chain fatty acids and obesity. Biosci. Microbiota Food Health 2017, 36, 135–140. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Zhang, A.; Miao, J.; Sun, H.; Yan, G.L.; Wu, F.F.; Wang, X.J. Gut microbiota as important modulator of metabolism in health and disease. RSC Adv. 2018, 8, 42380–42389. [Google Scholar] [CrossRef] [Green Version]
- Lipton, R.B.; Bigal, M.E.; Steiner, T.J.; Silberstein, S.D.; Olesen, J. Classification of primary headaches. Neurology 2004, 63, 427–435. [Google Scholar] [CrossRef]
- Stewart, W.F.; Lipton, R.B.; Dowson, A.J.; Sawyer, J. Development and testing of the migraine disability assessment (MIDAS) questionnaire to assess headache related disability. Neurology 2001, 56, S20–S28. [Google Scholar] [CrossRef]
- Brown, R.; Poxton, I.R.; Wilkinson, J.F. Centrifuges, colorimeters and bacterial counts. In Mackie and McCartney Practical Medical Microbiology, 14th ed.; Collee, J.G., Duguid, J.P., Fraser, A.G., Marmion, B.P., Eds.; Churchill Livingstone: Edinburgh, UK, 1999; pp. 200–247. [Google Scholar]
- Sandrin, T.R.; Goldstein, J.E.; Shoemaker, S. MALDI TOF MS profiling of bacteria at the strain level: A review. Mass Spectrom. Rev. 2013, 32, 188–217. [Google Scholar] [CrossRef] [PubMed]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redon, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A.; et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension. Eur. Heart J. 2013, 34, 2159–2219. [Google Scholar] [PubMed] [Green Version]
- Dogan, S.; Duivenvoorden, R.; Grobbee, D.; Kastelein, J.J.; Shear, C.L.; Evans, G.W.; Visseren, F.L.; Bots, M.L.; Radiance 1 and Radiance 2 Study Groups. Ultrasound protocols to measure carotid intima-media thickness in trials; comparison of reproducibility, rate of progression, and effect of intervention in subjects with familial hypercholesterolemia and subjects with mixed dyslipidemia. Ann. Med. 2010, 42, 447–464. [Google Scholar] [CrossRef] [PubMed]
- Goulart, A.C.; Itamar, S.; Santo, I.S.; Bittencourt, M.S. Migraine and subclinical atherosclerosis in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Cephalalgia 2015, 36, 840–848. [Google Scholar] [CrossRef]
- Yilmaz, A.; Akkucuk, M.H.; Torun, E.; Arikan, S.; Can, U.; Tekindal, M.A. Migraine and subclinical ATS: Endothelial dysfunction biomarkers and CIMT: A case-control study. Neurol. Sci. 2019, 40, 703–711. [Google Scholar] [CrossRef]
- Besir, F.H.; Koçer, A.; Dikici, S.; Yazgan, S.; Ozdem, Ş. The evaluation of atherosclerosis in migraine patients. Pain Pract. 2013, 13, 41–45. [Google Scholar] [CrossRef]
- González-Quintanilla, V.; Toriello, M.; Palacio, E.; González-Gay, M.A.; Castillo, J.; Montes, S.; Martínez-Nieto, R.; Fernandez, J.; Rojo, A.; Gutiérrez, S.; et al. Systemic and cerebral endothelial dysfunction in chronic migraine. A case-control study with an active comparator. Cephalalgia 2015, 36, 552–560. [Google Scholar]
- Saçmacı, H.; Turan, Y. Increased epicardial fat thickness and carotid intima-media thickness in migraine patients. Neurol. Sci. 2019, 15. [Google Scholar] [CrossRef]
- Emoto, T.; Yamashita, T.; Sasaki, N.; Hirota, Y.; Hayashi, T.; So, A.; Kasahara, K.; Yodoi, K.; Matsumoto, T.; Mizoguchi, T.; et al. Analysis of gut microbiota in coronary artery disease patients: A possible link between gut microbiota and coronary artery disease. J. Atheroscler. Thromb. 2016, 23, 908–921. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, A.; Hyde, E.; Sangwan, N.; Gilbert, J.A.; Viirre, E.; Knight, R. Migraines are correlated with higher levels of nitrate-, nitrite-, and nitric oxide-reducing oral microbes in the American gut project cohort. MSystems 2016, 1, e00105-16. [Google Scholar] [CrossRef] [Green Version]
- Kamada, N.; Seo, S.U.; Chen, G.I.; Núñez, G. Role of the gut microbiota in immunity and inflammatory disease. Nat. Rev. Immunol. 2013, 13, 321–335. [Google Scholar] [CrossRef]
- Parekh, P.J.; Arusi, E.; Vinik, A.I.; Johnson, D.A. The role and influence of gut microbiota in pathogenesis and management of obesity and metabolic syndrome. Front. Endocrinol. 2014, 5, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajslev, T.A.; Andersen, C.S.; Gamborg, M.; Sørensen, T.I.; Jess, T. Childhood overweight after establishment of the gut microbiota: The role of delivery mode, pregnancy weight and early administration of antibiotics. Int. J. Obes. 2011, 35, 522–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jess, T. Microbiota, antibiotics and obesity. N. Enl. J. Med. 2014, 371, 2526–2528. [Google Scholar] [CrossRef] [PubMed]
- Falony, G.; Joossens, M.; Vieira-Silva, S.; Wang, J.; Darzi, Y.; Faust, K.; Kurilshikov, A.; Bonder, M.J.; Valles-Colomer, M.; Vandeputte, D.; et al. Population-level analysis of gut microbiome variation. Science 2016, 352, 560–564. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.K.; Bolland, M.J.; van Pelt, N.C.; Horne, A.M.; Mason, B.H.; Ames, R.W.; Grey, A.B.; Ruygrok, P.N.; Gamble, G.D.; Reid, I.R. Relationships between vascular calcification, calcium metabolism, bone density and fractures. J. Bone Min. Res. 2010, 25, 2777–2785. [Google Scholar] [CrossRef] [PubMed]
- Silverman, N.G.; Blaha, M.J.; Krumholz, H.M.; Budoff, M.J.; Blankstein, R.; Sibley, C.T.; Agatston, A. Impact of coronary artery calcium on coronary heart disease events in individuals at the extremes of traditional risk factor burden: The multi-ethnic study of atherosclerosis. Eur. Heart J. 2014, 35, 2232–2241. [Google Scholar] [CrossRef] [PubMed]
- Manco, M.; Putignani, L.; Bottazzo, G.F. Gut microbiota lipopolysaccharides and innate immunity in the pathogenesis of obesity and cardiovascular risk. Endocr. Rev. 2010, 31, 817–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senthong, V.; Li, X.S.; Hudec, T.; Coughlin, J.; Wu, Y.; Levison, B.; Wang, Z.; Hazen, S.L.; Tang, W.H. Plasma TMAO, a gut microbe generated metabolite, is associated with atherosclerotic burden. J. Am. Coll. Cardiol. 2016, 67, 2620–2628. [Google Scholar] [CrossRef]
- Loomba, R.; Seguritan, V.; Li, W.; Long, T.; Klitgord, N.; Bhatt, A.; Dulai, P.S.; Caussy, C.; Bettencourt, R.; Highlander, S.K.; et al. Gut microbiom-based metagenomic signature for non invasive detection of advance fibrosis in human nonalcoholic fatty liver disease. Cell Metab. 2017, 25, 1054–1062. [Google Scholar] [CrossRef]
- Georgescu, D.; Reisz, D.; Gurban, C.V.; Georgescu, L.A.; Ionita, I.; Ancusa, O.E.; Lighezan, D. Migraine in young females with irritable bowel syndrome: Still a challenge. Neuropsychiatr. Dis. Treat. 2018, 14, 22–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Watanabe, K.; Kimura, I. Gut microbiota dysbiosis drives and implies novel therapeutic strategies for diabetes mellitus and related metabolic diseases. Front. Immunol. 2017, 8, 1882. [Google Scholar] [CrossRef] [PubMed]
- Koopen, A.M.; Groen, A.K.; Nieuwdorp, M. Human microbiome as therapeutic intervention target to reduce cardiovascular disease risk. Curr. Opin. Lipidol. 2016, 27, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Anbazhagan, A.N.; Priyamvada, S.; Priyadarshini, M. Gut microbiota in vascular disease: Therapeutic target? Curr. Vasc. Pharmacol. 2017, 15, 291–295. [Google Scholar] [PubMed]
- Santisteban, M.M.; Qi, Y.; Zubcevic, J.; Kim, S.; Yang, T.; Shenoy, V.; Cole-Jeffrey, C.T.; Lobaton, G.O.; Stewart, D.C.; Rubiano, A.; et al. Hypertension-linked pathophysiological alterations in the gut. Circ. Res. 2017, 120, 312–323. [Google Scholar] [CrossRef] [PubMed]
- Day, R.; Stone, S.; Harper, A. Probiotics for the prophylaxis of migraine: A systematic review of randomized placebo controlled trials. J. Int. Med. 2019, 8, 1441. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| DB Negative (n = 60) | DB Positive (n = 45) | p-Value | |
|---|---|---|---|
| Age (years) | 40.33 ± 3.44 | 39.40 ± 3.48 | 0.1796 |
| Urban Location | 81.66% | 80% | 0.8311 |
| High Educational level (graduated College) | 71.11% | 86.66% | 0.0498 |
| Marital situation (married) | 80% | 88.88% | 0.2238 |
| Migraine duration (years) | 10.12 ± 3.22 | 13.91 ± 5.21 | <0.0001 |
| MIDAS | 11.25 ± 2.48 | 16.09 ± 4.78 | <0.0001 |
| Body mass index (kg/m2) | 24.108 ± 0.696 | 24.627 ± 1.076 | 0.0028 |
| Body mass index (25–29.9kg/m2) | 25% | 44.44% | 0.03 |
| Systolic blood pressure (mmHg) | 116.25 ± 4.65 | 118.40 ± 6.15 | 0.0438 |
| DB Negative (n = 60) | DB Positive (n = 45) | p-Value | |
|---|---|---|---|
| Hemoglobin (g/dL) | 12.40 ± 1.245 | 12.27 ± 0.462 | 0.4102 |
| Leukocytes/mm3 | 7.339 × 103 ± 0.676 × 103 | 7.641 × 103 ± 0.695 × 103 | 0.0276 |
| Platelets/mm3 | 235.82 × 103 ± 57.14 × 103 | 228.00 × 103 ± 44.24 × 103 | 0.4478 |
| ALT (IU/dL) | 22.28 ± 3.88 | 26.13 ± 4.97 | <0.0001 |
| Creatinine (mg/dL) | 0.74 ± 0.089 | 0.76 ± 0.085 | 0.3743 |
| Hemoglobin A1c (%) | 5.063 ± 0.14 | 5.328 ± 0.371 | <0.0001 |
| Hemoglobin A1c:5.7%–6.4% | 5% | 20% | 0.0173 |
| Ionic calcium (mg/dL) | 8.8817 ± 0.181 | 9.427 ± 0.568 | <0.0001 |
| CRP (mg/dL) | 0.557 ± 0.300 | 0.687 ± 0.441 | 0.06 |
| TNF-alpha (pg/mL2) | 6.82 ± 2.57 | 8.97 ± 2.55 | 0.0047 |
| CIMT (mm) | 0.767 ± 0.157 | 0.991 ± 0.25 | <0.0001 |
| CIMT>0.9 mm | 15% | 40% | 0.039 |
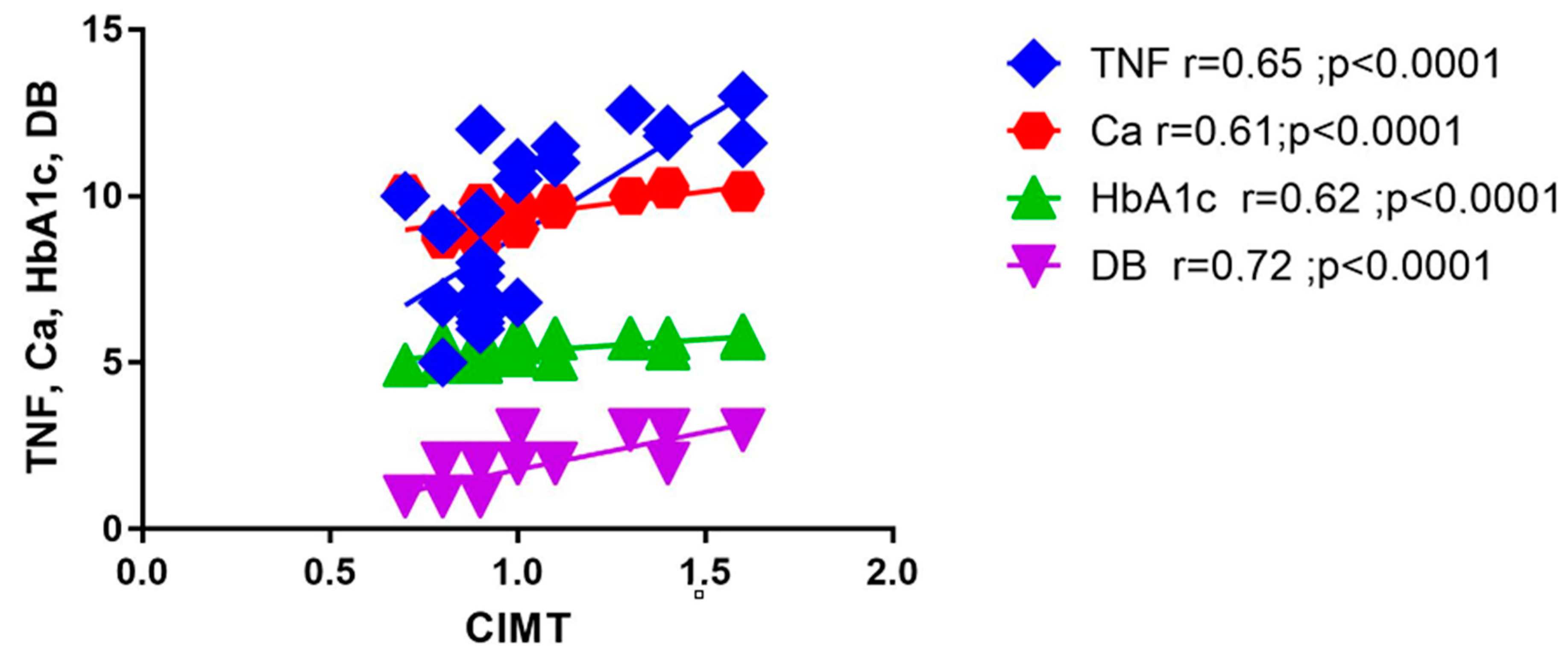
| Variables | r | P | |
|---|---|---|---|
| 1 | CIMT vs. TNF-alpha | 0.65 | <0.0001 |
| 2 | CIMT vs. Ca | 0.61 | <0.0001 |
| 3 | CIMT vs. HbA1c | 0.62 | <0.0001 |
| 4 | CIMT vs. DB | 0.72 | <0.0001 |
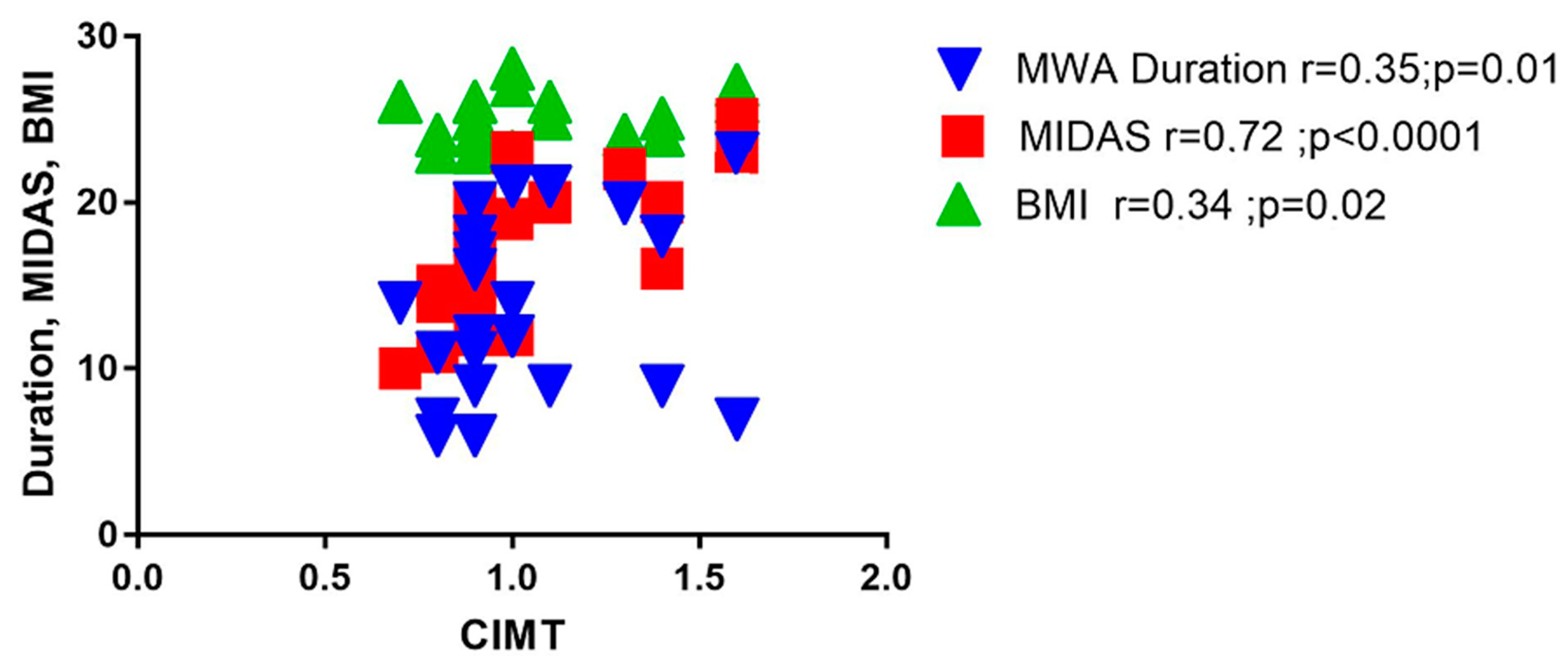
| 5 | CIMT vs. MWA duration | 0.35 | 0.01 |
| 6 | CIMT vs. MIDAS | 0.72 | <0.0001 |
| 7 | CIMT vs. BMI | 0.34 | 0.02 |
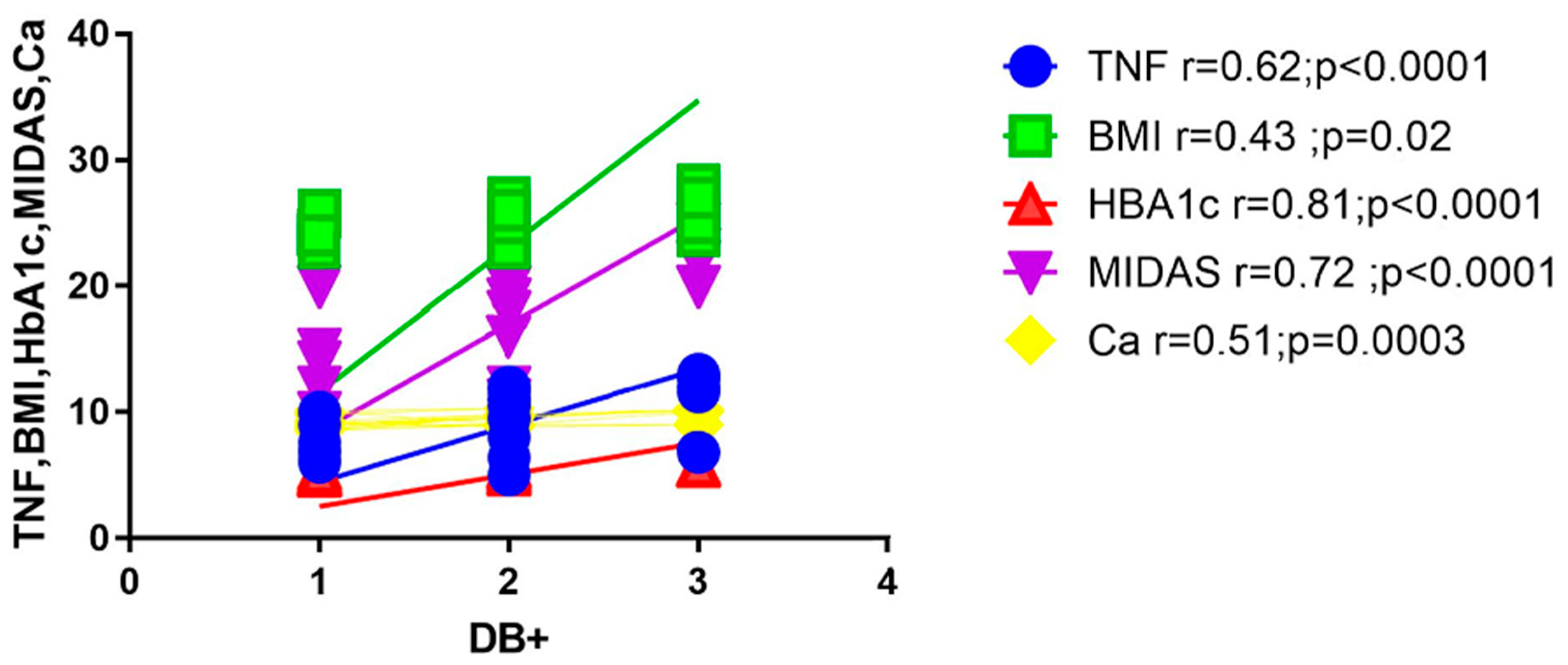
| 8 | DB vs. TNF-alpha | 0.62 | <0.0001 |
| 9 | DB vs. BMI | 0.43 | 0.02 |
| 10 | DB vs. HbA1c | 0.81 | <0.0001 |
| 11 | DB vs. MIDAS | 0.72 | <0.0001 |
| 12 | DB vs.Ca | 0.51 | 0.0003 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Georgescu, D.; Iurciuc, M.S.; Ionita, I.; Dragan, S.; Muntean, M.; Ancusa, O.E.; Reisz, D.; Ionita, M.; Lighezan, D. Migraine without Aura and Subclinical Atherosclerosis in Young Females: Is Gut Microbiota to Blame? Medicina 2019, 55, 786. https://doi.org/10.3390/medicina55120786
Georgescu D, Iurciuc MS, Ionita I, Dragan S, Muntean M, Ancusa OE, Reisz D, Ionita M, Lighezan D. Migraine without Aura and Subclinical Atherosclerosis in Young Females: Is Gut Microbiota to Blame? Medicina. 2019; 55(12):786. https://doi.org/10.3390/medicina55120786
Chicago/Turabian StyleGeorgescu, Doina, Mircea Stefan Iurciuc, Ioana Ionita, Simona Dragan, Mihaela Muntean, Oana Elena Ancusa, Daniela Reisz, Mihai Ionita, and Daniel Lighezan. 2019. "Migraine without Aura and Subclinical Atherosclerosis in Young Females: Is Gut Microbiota to Blame?" Medicina 55, no. 12: 786. https://doi.org/10.3390/medicina55120786