Indexes of Angiogenic Activation in Myocardial Samples of Patients with Advanced Chronic Heart Failure

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Heart Tissue Specimens from Ischemic and non-Ischemic Dilated Cardiomyopathy Patients Study Population
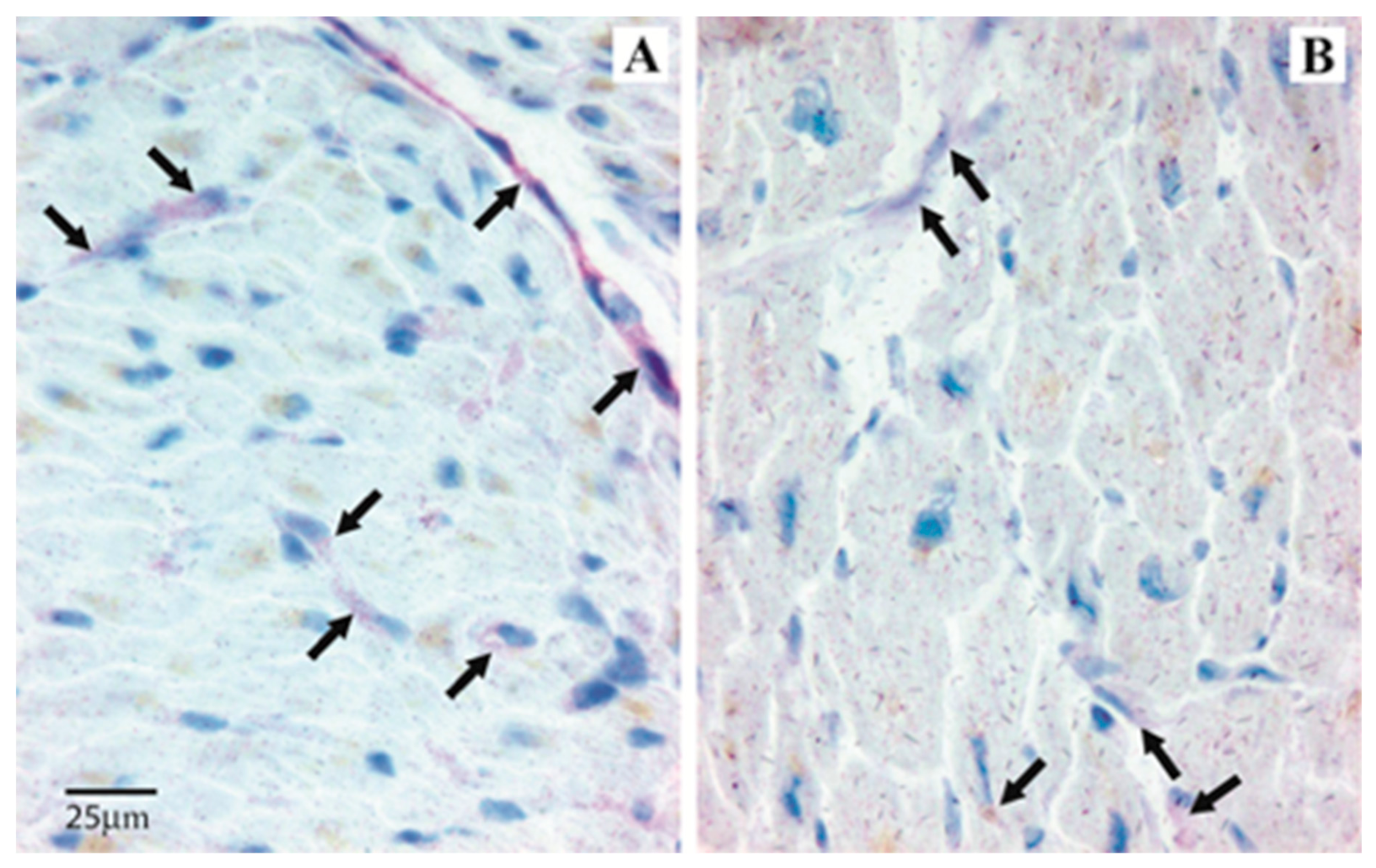
2.2. Immunohistochemistry in the Heart Tissue
2.3. Scoring System for Immunohistochemistry
2.4. Statistical Analysis
3. Results
Immunohistochemistry in the Heart Tissue
4. Discussion
Study Limitation
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Roura, S.; Bayes-Genis, A. Vascular dysfunction in idiopathic dilated cardiomyopathy. Nat. Rev. Cardiol. 2009, 6, 590–598. [Google Scholar] [CrossRef]
- Moryja, J.; Minamino, T. Angiogenesis, Cancer, and Vascular Aging. Front. Cardiovasc. Med. 2017, 4, 65. [Google Scholar]
- Eklund, L.; Kangas, J.; Saharinen, P. Angiopoietin-Tie signalling in the cardiovascular and lymphatic systems. Clin. Sci. (Lond.) 2017, 131, 87–103. [Google Scholar] [CrossRef] [PubMed]
- Felmeden, D.C.; Blann, A.D.; Lip, G.Y. Angiogenesis: Basic pathophysiology and implications for disease. Eur. Heart J. 2003, 24, 586–603. [Google Scholar] [CrossRef]
- de Lucia, C.; Eguchi, A.; Koch, W.J. New Insights in Cardiac β-Adrenergic Signaling During Heart Failure and Aging. Front. Pharmacol. 2018, 9, 904. [Google Scholar] [CrossRef]
- Rengo, G.; Cannavo, A.; Liccardo, D.; Zincarelli, C.; de Lucia, C.; Pagano, G.; Komici, K.; Parisi, V.; Scala, O.; Agresta, A.; et al. Vascular endothelial growth factor blockade prevents the beneficial effects of β-blocker therapy on cardiac function, angiogenesis, and remodeling in heart failure. Circ. Heart Fail. 2013, 6, 1259–1267. [Google Scholar] [CrossRef]
- La Rocca, G.; Di Stefano, A.; Eleuteri, E.; Anzalone, R.; Magno, F.; Corrao, S.; Loria, T.; Martorana, A.; Di Gangi, C.; Colombo, M.; et al. Oxidative stress induces myeloperoxidase expression in endocardial endothelial cells from patients with chronic heart failure. Basic Res. Cardiol. 2009, 104, 307–320. [Google Scholar] [CrossRef]
- Chin, B.S.; Chung, N.A.; Gibbs, C.R.; Blann, A.D.; Lip, G.Y. Vascular endothelial growth factor and soluble P-selectin in acute and chronic congestive heart failure. Am. J Cardiol. 2002, 90, 1258–1260. [Google Scholar] [CrossRef]
- Chong, A.Y.; Caine, G.J.; Freestone, B.; Blann, A.D.; Lip, G.Y. Plasma angiopoietin-1, angiopoietin-2, and angiopoietin receptor tie-2 levels in congestive heart failure. J. Am. Coll. Cardiol. 2004, 43, 423–428. [Google Scholar] [CrossRef]
- Patel, J.V.; Sosin, M.; Gunarathne, A.; Hussain, I.; Davis, R.C.; Hughes, E.A.; Lip, G.Y. Elevated angiogenin levels in chronic heart failure. Ann. Med. 2008, 40, 474–479. [Google Scholar] [CrossRef]
- Ohtsuka, T.; Inoue, K.; Hara, Y.; Morioka, N.; Ohshima, K.; Suzuki, J.; Ogimoto, A.; Shigematsu, Y.; Higaki, J. Serum markers of angiogenesis and myocardial ultrasonic tissue characterization in patients with dilated cardiomyopathy. Eur. J. Heart Fail. 2005, 7, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Fujisawa, T.; Niu, X.L.; Ahmad, S.; Al-Ani, B.; Chudasama, K.; Abbas, A.; Potluri, R.; Bhandari, V.; Findley, C.M.; et al. Angiopoietin-2 confers Atheroprotection in apoE-/- mice by inhibiting LDL oxidation via nitric oxide. Circ. Res. 2009, 104, 1333–1336. [Google Scholar] [CrossRef] [PubMed]
- Theelen, T.L.; Lappalainen, J.P.; Sluimer, J.C.; Gurzeler, E.; Cleutjens, J.P.; Gijbels, M.J.; Biessen, E.A.; Daemen, M.J.; Alitalo, K.; Ylä-Herttuala, S. Angiopoietin-2 blocking antibodies reduce early atherosclerotic plaque development in mice. Atherosclerosis 2015, 241, 297–304. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.; Adamopoulos, S.; Anker, S.D.; Auricchio, A.; Böhm, M.; Dickstein, K.; Falk, V.; Filippatos, G.; Fonseca, C.; Gomez-Sanchez, M.A.; et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The task force for the diagnosis and treatment of acute and chronic heart failure 2012 of the european society of cardiology. Developed in collaboration with the heart failure association (HFA) of the ESC. Eur. Heart J. 2012, 14, 1787–1847. [Google Scholar]
- Eleuteri, E.; Di Stefano, A.; Tarro Genta, F.; Vicari, C.; Gnemmi, I.; Colombo, M.; Mezzani, A.; Giannuzzi, P. Stepwise increase of angiopoietin-2 serum levels is related to haemodynamic and functional impairment in stable chronic heart failure. Eur. J. Cardiovasc. Prev. Rehabil. 2011, 18, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Tello-Montoliu, A.; Marín, F.; Patel, J.; Roldán, V.; Mainar, L.; Vicente, V.; Sogorb, F.; Lip, G.Y. Plasma angiogenin levels in acute coronary syndromes: Implications for prognosis. Eur. Heart J. 2007, 28, 3006–3011. [Google Scholar] [CrossRef]
- Eleuteri, E.; Di Stefano, A.; Giordano, A.; Corrà, U.; Tarro Genta, F.; Gnemmi, I.; Giannuzzi, P. Prognostic value of angiopoietin-2 in patients with chronic heart failure. Int. J. Cardiol. 2016, 212, 364–368. [Google Scholar] [CrossRef]
- Lukasz, A.; Beutel, G.; Kümpers, P.; Denecke, A.; Westhoff-Bleck, M.; Schieffer, B.; Bauersachs, J.; Kielstein, J.T.; Tutarel, O. Angiopoietin-2 in adults with congenital heart disease and heart failure. PLoS ONE 2013, 8, e66861. [Google Scholar] [CrossRef]
- Arita, Y.; Nakaoka, Y.; Matsunaga, T.; Kidoya, H.; Yamamizu, K.; Arima, Y.; Kataoka-Hashimoto, T.; Ikeoka, K.; Yasui, T.; Masaki, T.; et al. Myocardium-derived angiopoietin-1 is essential for coronary vein formation in the developing heart. Nat. Commun. 2014, 5, 4552. [Google Scholar] [CrossRef]
- Ren, D.; Zhu, Q.; Li, J.; Ha, T.; Wang, X.; Li, Y. Overexpression of angiopoietin-1 reduces doxorubicin-induced apoptosis in cardiomyocytes. J. Biomed. Res. 2012, 26, 432–438. [Google Scholar] [CrossRef]
- Kim, I.; Kim, H.G.; Moon, S.O.; Chae, S.W.; So, J.N.; Koh, K.N.; Ahn, B.C.; Koh, G.Y. Angiopoietin-1 induces endothelial cell sprouting through the activation of focal adhesion kinase and plasmin secretion. Circ. Res. 2000, 86, 952–959. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Cell Type | Angiogenin | Ang-1 | Ang-2 | Tie-2 | PICP |
|---|---|---|---|---|---|
| Cardiomyocyte perinuclear space | +++ | +++ | − | +++ | +++ |
| Endothelial Cells | +−− | +−− | +++ | +++ | −−− |
| Infiltrating Inflammatory Cells | +−− | +−− | +−− | +−− | −−− |
| Subjects (n) | Angiogenin | Ang-1 | Ang-2 | Tie-2 | PICP |
|---|---|---|---|---|---|
| ICM (9) | 1.25 (0.75–1.75) | 2.625 (1.25–3) | 0.625 (0.25–1.25) * | 1.375 (1.125–1.75) | 2.25 (1.5–2.5) |
| NIDCM (7) | 0.5 (0.375–2) | 2.5 (0.25–2.75) | 0.25 (0–0.75) | 1.75 (0–2.125) | 2.25 (1.5–2.5) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Komici, K.; Gnemmi, I.; Sangiorgi, C.; Ricciardolo, F.L.M.; Rinaldi, M.; Di Stefano, A.; Eleuteri, E. Indexes of Angiogenic Activation in Myocardial Samples of Patients with Advanced Chronic Heart Failure. Medicina 2019, 55, 766. https://doi.org/10.3390/medicina55120766
Komici K, Gnemmi I, Sangiorgi C, Ricciardolo FLM, Rinaldi M, Di Stefano A, Eleuteri E. Indexes of Angiogenic Activation in Myocardial Samples of Patients with Advanced Chronic Heart Failure. Medicina. 2019; 55(12):766. https://doi.org/10.3390/medicina55120766
Chicago/Turabian StyleKomici, Klara, Isabella Gnemmi, Claudia Sangiorgi, Fabio Luigi Massimo Ricciardolo, Mauro Rinaldi, Antonino Di Stefano, and Ermanno Eleuteri. 2019. "Indexes of Angiogenic Activation in Myocardial Samples of Patients with Advanced Chronic Heart Failure" Medicina 55, no. 12: 766. https://doi.org/10.3390/medicina55120766