Long Term Results of Modified Intersphincteric Resections for Low Rectal Cancer: A Single Center Experience

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
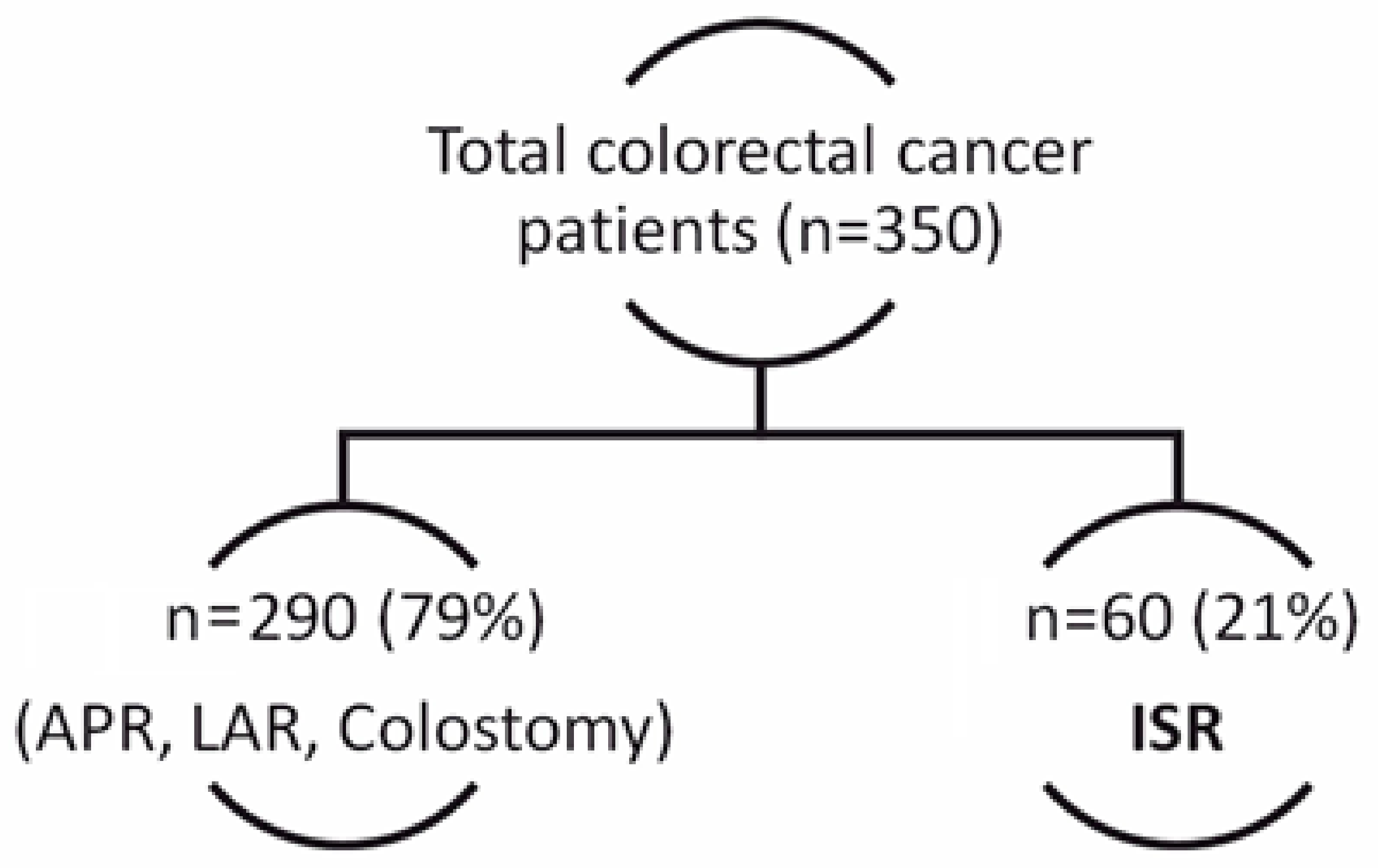
2.1. Selection Criteria
2.2. Exclusion Criteria
2.3. Diagnostic Management and Preoperative Staging
2.4. Surgical Technique
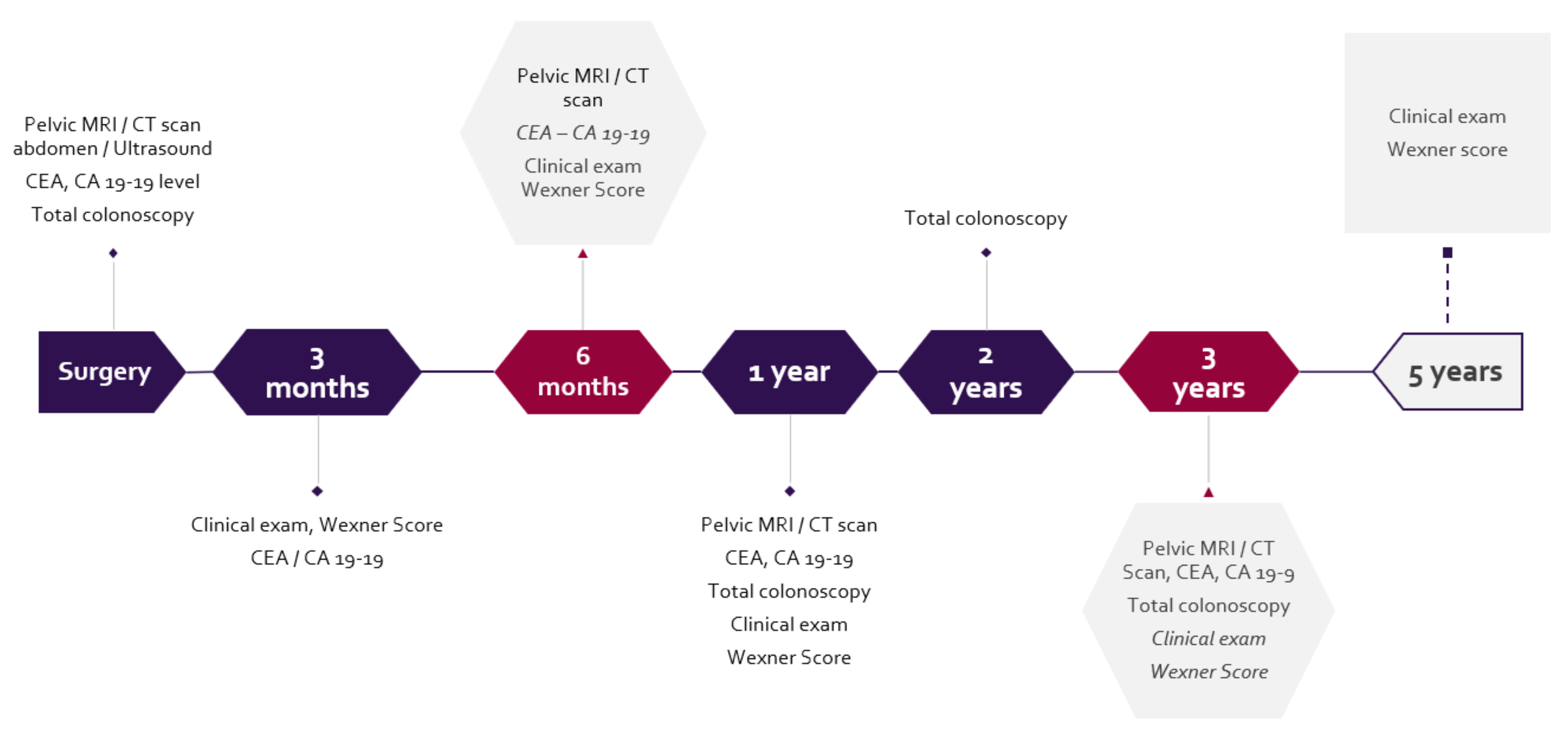
2.5. Assessment and Follow-Up
2.6. Statistical Assessment
3. Results
3.1. Clinicopathological Characteristics and Operative Particularities
3.2. Postoperative Complications
3.3. Overall Survival
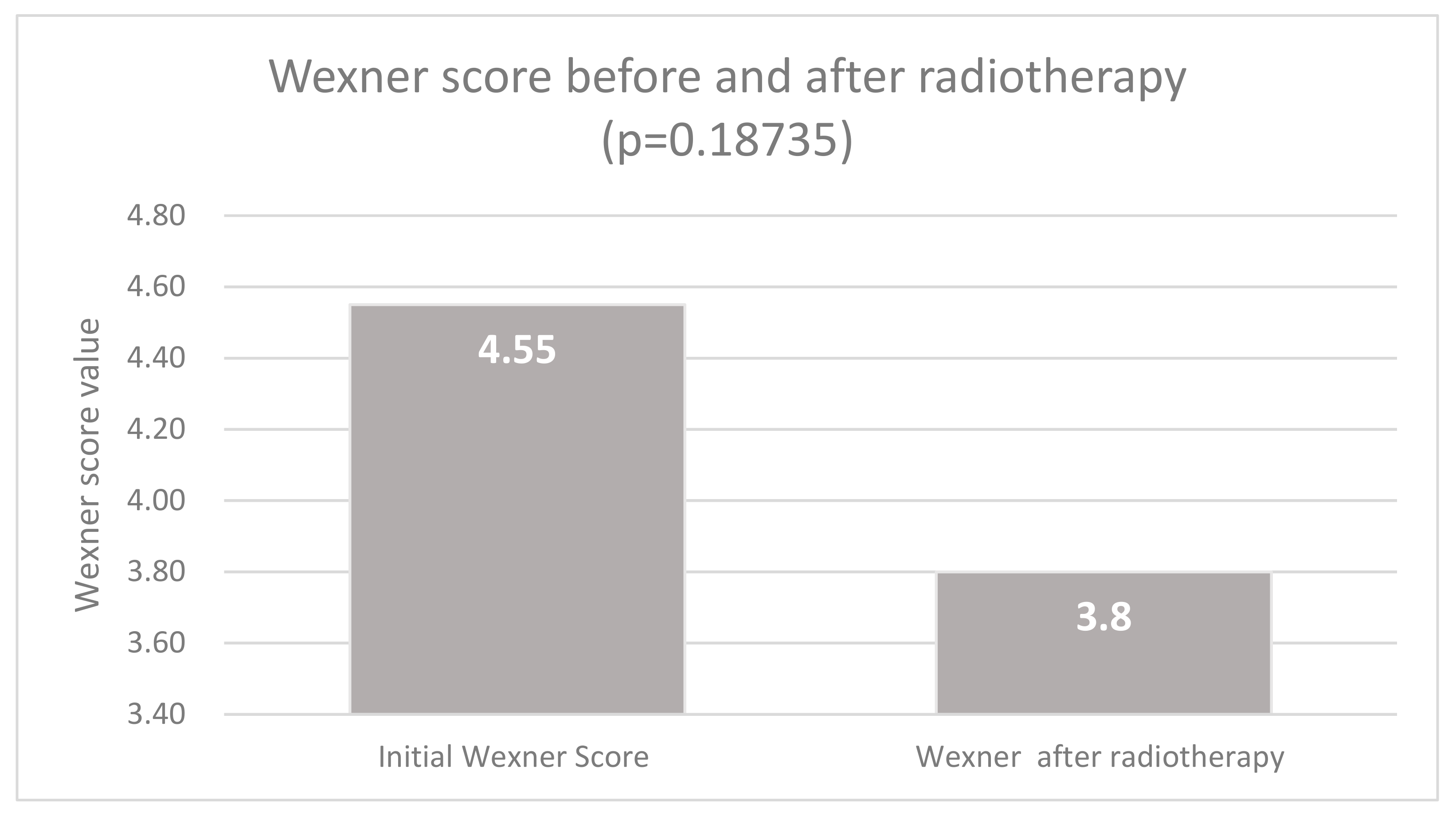
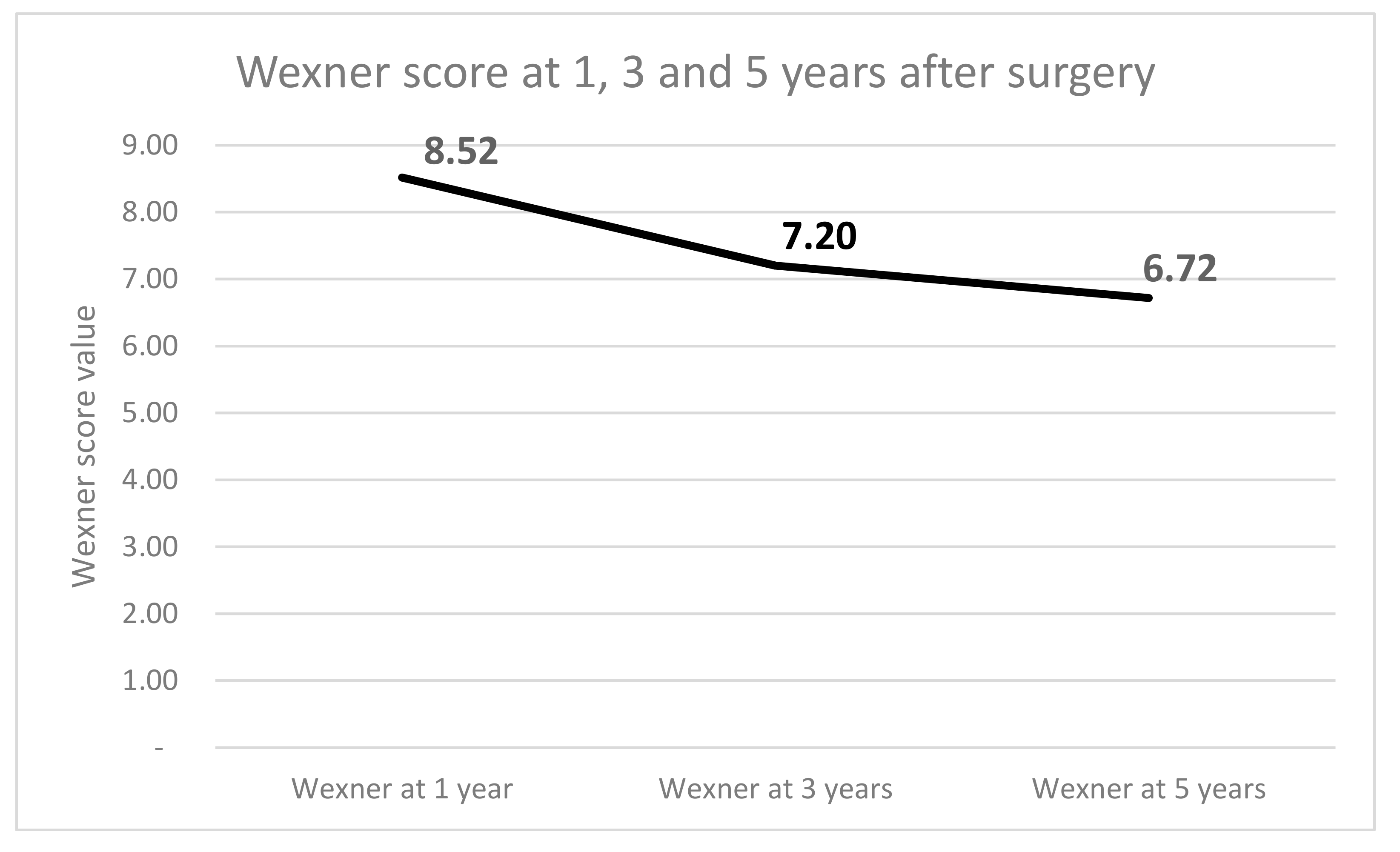
3.4. Wexner Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Schiessel, R.; Karner-Hanusch, J.; Herbst, F.; Teleky, B.; Wunderlich, M. Intersphincteric resection for low rectal tumours. Br. J. Surg. 1994, 81, 1376–1378. [Google Scholar] [CrossRef]
- Heald, R.J.; Ryall, R.D.H. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet 1986, 327, 1479–1482. [Google Scholar] [CrossRef]
- Kapiteijn, E.; Marijnen, C.A.; Nagtegaal, I.D.; Putter, H.; Steup, W.H.; Wiggers, T.; Leer, J.W. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N. Engl. J. Med. 2001, 345, 638–646. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, D.; Lörinc, E.; Holm, T.; Iversen, H.; Cedermark, B.; Glimelius, B.; Martling, A. Tumour regression in the randomized Stockholm III trial of radiotherapy regimens for rectal cancer. Br. J. Surg. 2015, 102, 972–978. [Google Scholar] [CrossRef] [PubMed]
- Breugom, A.J.; Swets, M.; Bosset, J.F.; Collette, L.; Sainato, A.; Cionini, L.; Liefers, G.J. Adjuvant chemotherapy after preoperative (chemo) radiotherapy and surgery for patients with rectal cancer: A systematic review and meta-analysis of individual patient data. Lancet Oncol. 2015, 16, 200–207. [Google Scholar] [CrossRef]
- Glynne-Jones, R.L.; Wyrwicz, E.; Tiret, G.; Brown, C.; Rödel, A.; Cervantes, D. Arnold, on behalf of the ESMO Guidelines Committee, Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv22–iv40. [Google Scholar] [CrossRef]
- Smith, N.J.; Shihab, O.; Arnaout, A.; Swift, R.I.; Brown, G. MRI for detection of extramural vascular invasion in rectal cancer. Am. J. Roentgenol. 2008, 191, 1517–1522. [Google Scholar] [CrossRef] [PubMed]
- Shihab, O.C.; Heald, R.J.; Rullier, E.; Brown, G.; Holm, T.; Quirke, P.; Moran, B.J. Defining the surgical planes on MRI improves surgery for cancer of the low rectum. Lancet Oncol. 2009, 10, 1207–1211. [Google Scholar] [CrossRef]
- Rullier, E.; Denost, Q.; Vendrely, V.; Rullier, A.; Laurent, C. Low rectal cancer: Classification and standardization of surgery. Dis. Colon Rectum 2013, 56, 560–567. [Google Scholar] [CrossRef]
- Rullier, E.; Laurent, C.; Bretagnol, F.; Rullier, A.; Vendrely, V.; Zerbib, F. Sphincter-saving resection for all rectal carcinomas: The end of the 2-cm distal rule. Ann. Surg. 2005, 241, 465–469. [Google Scholar] [CrossRef]
- Solh, W.; Wexner, S.D. Scoring Systems. In Pelvic Floor Dysfunction; Davila, G.W., Ghoniem, G.M., Wexner, S.D., Eds.; Springer: London, UK, 2006. [Google Scholar]
- Bugg, W.G.; Andreou, A.K.; Biswas, D.; Toms, A.P.; Williams, S.M. The prognostic significance of MRI-detected extramural venous invasion in rectal carcinoma. Clin. Radiol. 2014, 69, 619–623. [Google Scholar] [CrossRef] [PubMed]
- Taylor, F.G.; Swift, R.I.; Blomqvist, L.; Brown, G. A systematic approach to the interpretation of preoperative staging MRI for rectal cancer. Am. J. Roentgenol. 2008, 191, 1827–1835. [Google Scholar] [CrossRef] [PubMed]
- Hötker, A.M.; Tarlinton, L.; Mazaheri, Y.; Woo, K.M.; Gönen, M.; Saltz, L.B.; Gollub, M.J. Multiparametric MRI in the assessment of response of rectal cancer to neoadjuvant chemoradiotherapy: A comparison of morphological, volumetric and functional MRI parameters. Eur. Radiol. 2016, 26, 4303–4312. [Google Scholar] [CrossRef] [PubMed]
- Battersby, N.J.; How, P.; Moran, B.; Stelzner, S.; West, N.P.; Branagan, G.; Gudgeon, M. Prospective validation of a low rectal cancer magnetic resonance imaging staging system and development of a local recurrence risk stratification model. Ann. Surg. 2016, 263, 751–760. [Google Scholar] [CrossRef] [PubMed]
- MERCURY Study Group. Diagnostic accuracy of preoperative magnetic resonance imaging in predicting curative resection of rectal cancer: Prospective observational study. Br. Med. J. 2006, 333, 779–782. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Li, X.; Xu, L.; Shi, D.; Tong, T.; Huang, D.; Peng, J. Characteristics and prognostic significance of preoperative magnetic resonance imaging-assessed circumferential margin in rectal cancer. Gastroenterol. Res. Pract. 2015. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.; Richards, C.J.; Newcombe, R.G.; Dallimore, N.S.; Radcliffe, A.G.; Carey, D.P.; Williams, G.T. Rectal carcinoma: Thin-section MR imaging for staging in 28 patients. Radiology 1999, 211, 215–222. [Google Scholar] [CrossRef]
- Heald, R.J.; Moran, B.J.; Ryall, R.D.; Sexton, R.; MacFarlane, J.K. Rectal cancer: The Basingstoke experience of total mesorectal excision, 1978–1997. Arch. Surg. 1998, 133, 894–898. [Google Scholar] [CrossRef]
- MacFarlane, J.K.; Ryall, R.D.H.; Heald, R.J. Mesorectal excision for rectal cancer. Lancet 1993, 341, 457–460. [Google Scholar] [CrossRef]
- van Gijn, W.; Marijnen, C.A.; Nagtegaal, I.D.; Kranenbarg, E.M.; Putter, H.; Wiggers, T.; Rutten, H.J.; Påhlman, L.; Glimelius, B.; van de Velde, C.J.; et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled TME trial. Lancet Oncol. 2011, 12, 575–582. [Google Scholar] [CrossRef]
- Molnar, C.; Vlad-Olimpiu, B.; Marian, B.; Cornelia, T.; Simona, G. Survival and functional and oncological outcomes following intersphincteric resection for low rectal cancer: Short-term results. J. Int. Med. Res. 2018, 46, 1617–1625. [Google Scholar] [CrossRef]
- Rubinkiewicz, M.; Zarzycki, P.; Czerwińska, A.; Wysocki, M.; Gajewska, N.; Torbicz, G.; Pędziwiatr, M. A quest for sphincter-saving surgery in ultralow rectal tumours—A single-centre cohort study. World J. Surg. Oncol. 2018, 16, 218. [Google Scholar] [CrossRef]
- Park, I.J.; Kim, J.C. Intersphincteric Resection for Patients with Low-Lying Rectal Cancer: Oncological and Functional Outcomes. Ann. Coloproctol. 2018, 34, 167. [Google Scholar] [CrossRef] [PubMed]
- Laurent, C.; Paumet, T.; Leblanc, F.; Denost, Q.; Rullier, E. Intersphincteric resection for low rectal cancer: Laparoscopic vs open surgery approach. Colorectal Dis. 2012, 14, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Chi, P.; Huang, S.H.; Lin, H.M.; Lu, X.R.; Huang, Y.; Jiang, W.Z.; Ye, D.X. Laparoscopic transabdominal approach partial intersphincteric resection for low rectal cancer: Surgical feasibility and intermediate-term outcome. Ann. Surg. Oncol. 2015, 22, 944–951. [Google Scholar] [CrossRef]
- Chen, H.; Ma, B.; Gao, P.; Wang, H.; Song, Y.; Tong, L.; Wang, Z. Laparoscopic intersphincteric resection versus an open approach for low rectal cancer: A meta-analysis. World J. Surg. Oncol. 2017, 15, 229. [Google Scholar] [CrossRef] [PubMed]
- Schoellhammer, H.F.; Gregorian, A.C.; Sarkisyan, G.G.; Petrie, B.A. How important is rigid proctosigmoidoscopy in localizing rectal cancer? Am. J. Surg. 2008, 196, 904–908. [Google Scholar] [CrossRef] [PubMed]
- Shirouzu, K.; Murakami, N.; Akagi, Y. Intersphincteric resection for very low rectal cancer: A review of the updated literature. Ann. Gastroenterol. Surg. 2017, 1, 24–32. [Google Scholar] [CrossRef]
- Akagi, Y.; Kinugasa, T.; Shirouzu, K. Intersphincteric resection for very low rectal cancer: A systematic review. Surg. Today 2013, 43, 838–847. [Google Scholar] [CrossRef]
- Spanos, C.P. Intersphincteric resection for low rectal cancer: An overview. Int. J. Surg. Oncol. 2012. [Google Scholar] [CrossRef]
- Martin, S.T.; Heneghan, H.M.; Winter, D.C. Systematic review of outcomes after intersphincteric resection for low rectal cancer. Br. J. Surg. 2012, 99, 603–612. [Google Scholar] [CrossRef] [PubMed]
- Hallböök, O.; Påhlman, L.; Krog, M.; Wexner, S.D.; Sjödahl, R. Randomized comparison of straight and colonic J pouch anastomosis after low anterior resection. Ann. Surg. 1996, 224, 58. [Google Scholar] [CrossRef] [PubMed]
- Lazorthes, F.; Chiotasso, P.; Gamagami, R.A.; Istvan, G.; Chevreau, P. Late clinical outcome in a randomized prospective comparison of colonic J pouch and straight coloanal anastomosis. Br. J. Surg. 1997, 84, 1449–1451. [Google Scholar] [CrossRef] [PubMed]
- Fichera, A.; Michelassi, F. Long-term prospective assessment of functional results after proctectomy with coloanal anastomosis. J. Gastrointest. Surg. 2001, 5, 153–157. [Google Scholar] [CrossRef]
- Yamamoto, S.; Fujita, S.; Akasu, T.; Inada, R.; Takawa, M.; Moriya, Y. Short-term outcomes of laparoscopic intersphincteric resection for lower rectal cancer and comparison with open approach. Dig. Surg. 2011, 28, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, T.H.; Church, J.M.; Fleshman, J.W.; Kane, R.L.; Mavrantonis, C.; Thorson, A.G.; Lowry, A.C. Fecal incontinence quality of life scale. Dis. Colon Rectum 2000, 43, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Vaizey, C.J.; Carapeti, E.; Cahill, J.A.; Kamm, M.A. Prospective comparison of faecal incontinence grading systems. Gut 1999, 44, 77–80. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, B.D.S.; Reis, I.G.N.; Coelho, F.M.D.O.; Buzatti, K.C.D.L.R. Fecal incontinence and quality of life assessment through questionnaires. J. Coloproctol. (Rio de Janeiro) 2017, 37, 341–348. [Google Scholar] [CrossRef]
- Saito, N.; Moriya, Y.; Shirouzu, K.; Maeda, K.; Mochizuki, H.; Koda, K.; Kobayashi, A. Intersphincteric resection in patients with very low rectal cancer: A review of the Japanese experience. Dis. Colon Rectum 2006, 49, S13–S22. [Google Scholar] [CrossRef]
- Ursi, P.; Santoro, A.; Gemini, A.; Arezzo, A.; Pironi, D.; Renzi, C.; Sagar, J. Comparison of outcomes following intersphincteric resection vs low anterior resection for low rectal cancer: A systematic review. Il Giornale di Chirurgia 2018, 39, 123–142. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Never | Rarely | Sometimes | Usually | Always | |
|---|---|---|---|---|---|
| Solid | 0 | 1 | 2 | 3 | 4 |
| Liquid | 0 | 1 | 2 | 3 | 4 |
| Gas | 0 | 1 | 2 | 3 | 4 |
| Wears pad | 0 | 1 | 2 | 3 | 4 |
| Alters lifestyle | 0 | 1 | 2 | 3 | 4 |
| Parameter | Value (n = 60) |
|---|---|
| Age (years) | 67.32 ± 21.45 (range 57–81) |
| Male/female ratio | 2.16:1 |
| Tumor characteristics | |
| Distance from anal verge (cm) | 3.15 ± 1.82 (range 1–4) |
| Localization | |
| Intra-anal (type III) | 13 (22%) |
| Juxta-anal (type II) | 47 (78%) |
| Procedure | |
| Partial ISR | 47 (78%) |
| Total ISR | 13 (22%) |
| Serum markers | |
| CEA > 12 ng/mL | 63% |
| CA 19–9 > 900 U/mL | 45% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Butiurca, V.-O.; Molnar, C.; Constantin, C.; Botoncea, M.; Bud, T.I.; Kovacs, Z.; Satala, C.; Gurzu, S. Long Term Results of Modified Intersphincteric Resections for Low Rectal Cancer: A Single Center Experience. Medicina 2019, 55, 764. https://doi.org/10.3390/medicina55120764
Butiurca V-O, Molnar C, Constantin C, Botoncea M, Bud TI, Kovacs Z, Satala C, Gurzu S. Long Term Results of Modified Intersphincteric Resections for Low Rectal Cancer: A Single Center Experience. Medicina. 2019; 55(12):764. https://doi.org/10.3390/medicina55120764
Chicago/Turabian StyleButiurca, Vlad-Olimpiu, Călin Molnar, Copotoiu Constantin, Marian Botoncea, Teodor Ioan Bud, Zsolt Kovacs, Cătălin Satala, and Simona Gurzu. 2019. "Long Term Results of Modified Intersphincteric Resections for Low Rectal Cancer: A Single Center Experience" Medicina 55, no. 12: 764. https://doi.org/10.3390/medicina55120764