
Moringa oleifera: A Review on the Antiproliferative Potential in Breast Cancer Cells

Abstract
:1. Introduction
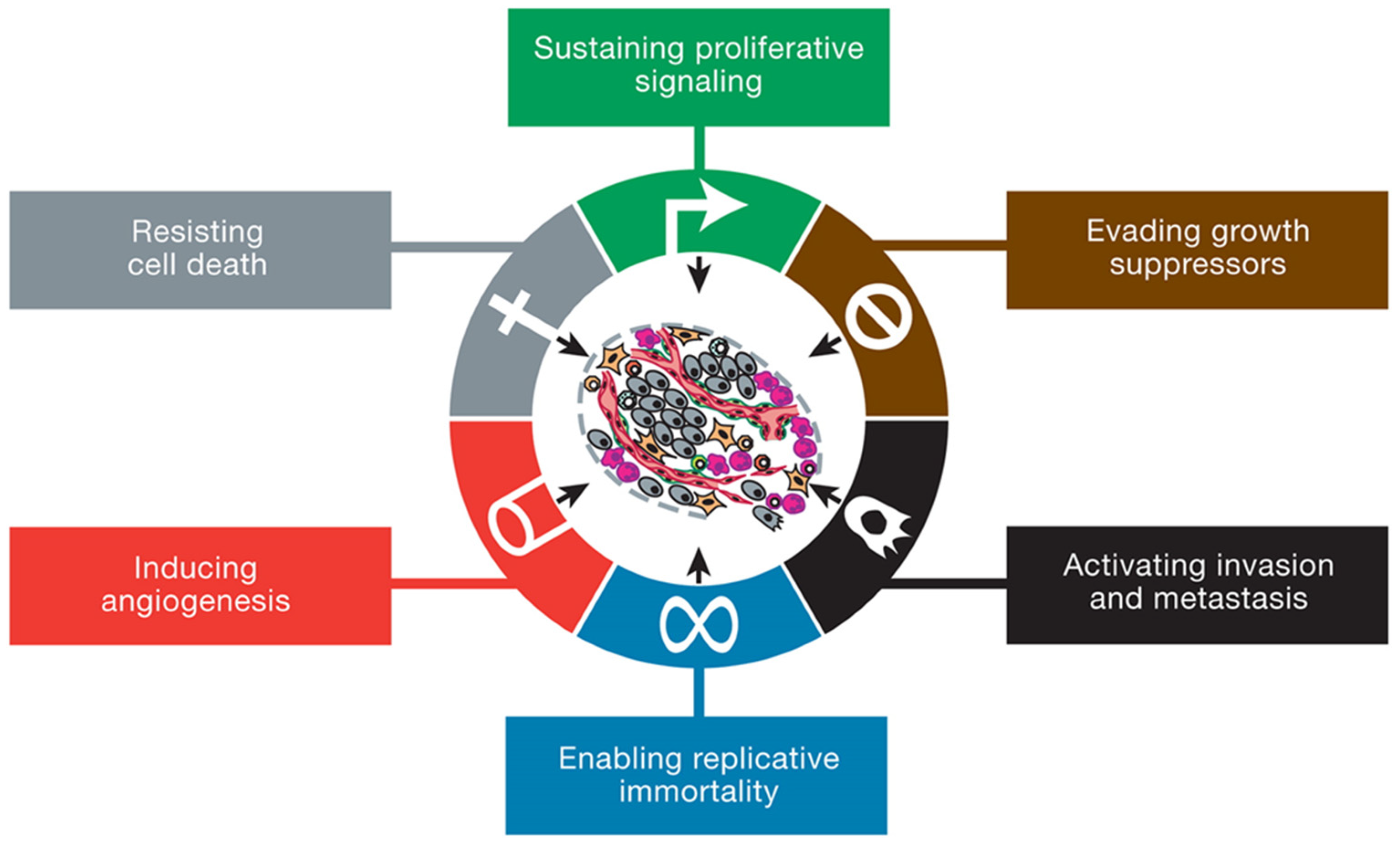
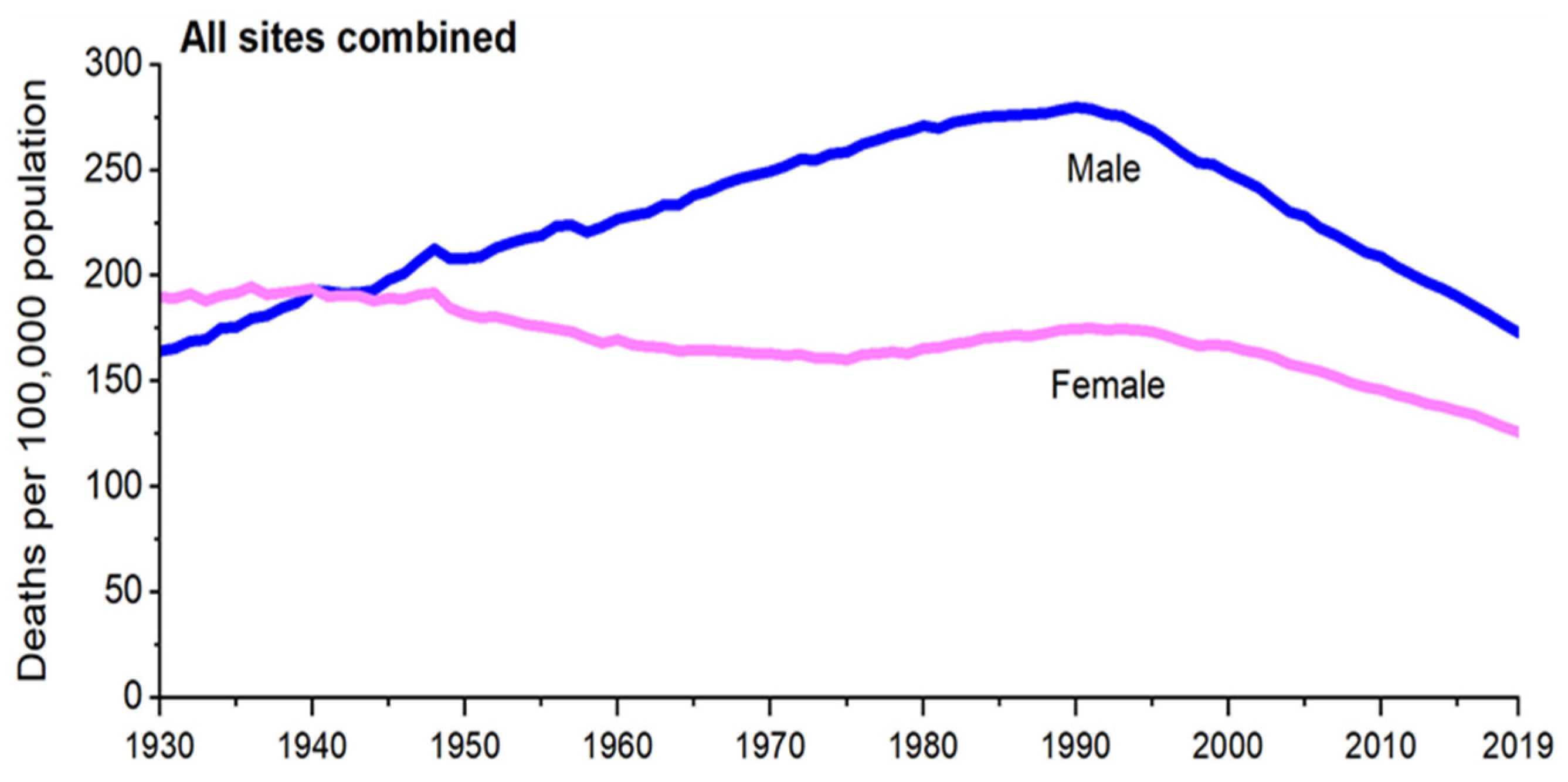
2. Cancer
3. Breast Cancer Epidemiology
4. Breast Cancer Aetiology
5. Breast Cancer Pathophysiology
6. Breast Cancer Diagnosis
7. Breast Cancer Classification
8. Breast Cancer Stages and Grades
9. Current Cancer Treatment Therapies
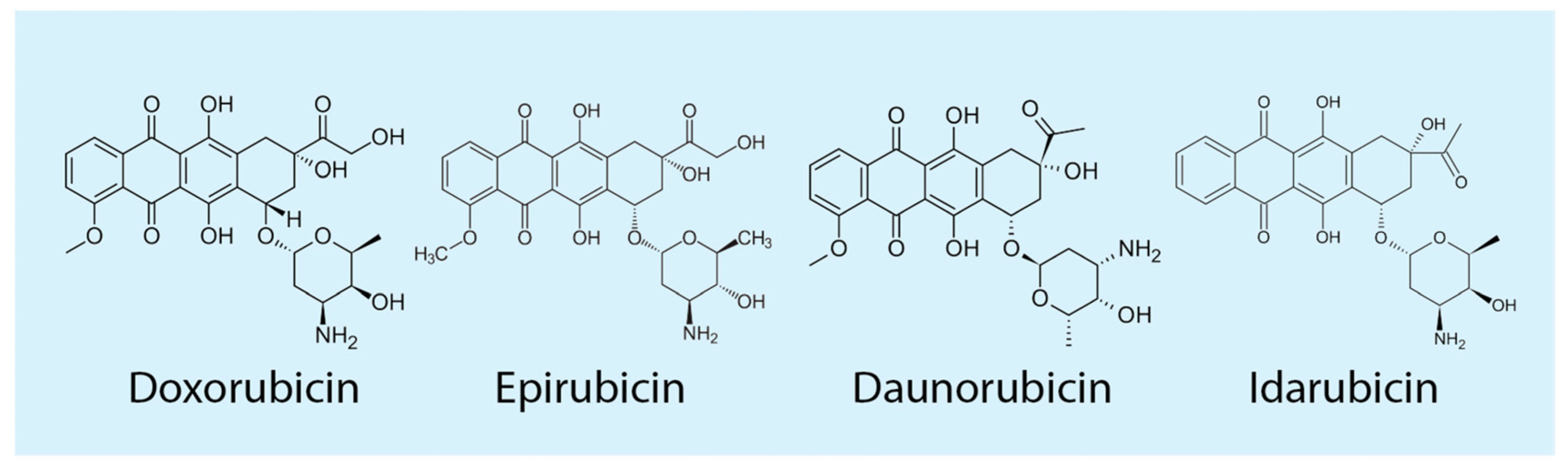
10. Mechanism of Action of Dox
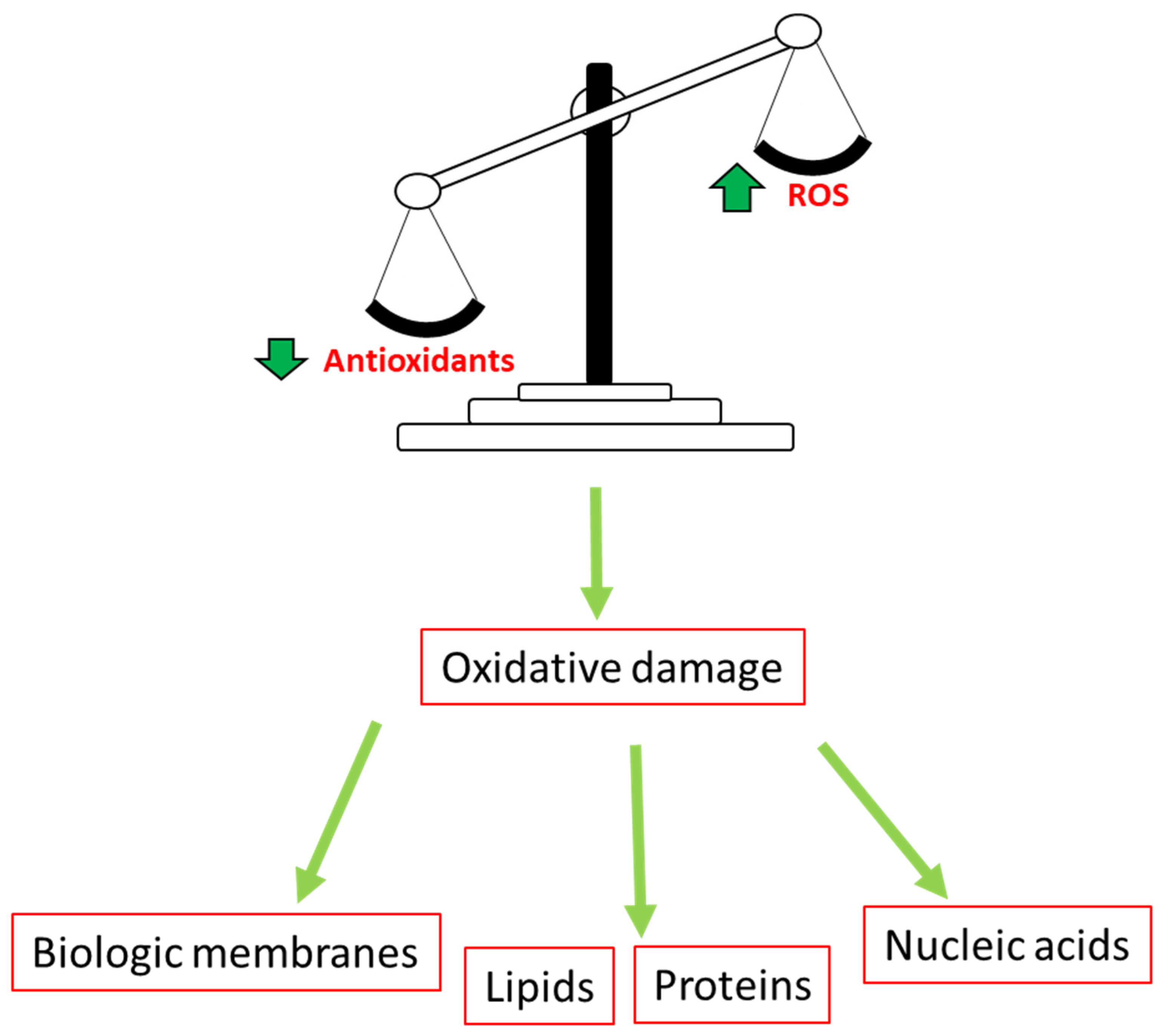
11. Role of Oxidative Stress in Cancer

12. Antioxidants and Breast Cancer
13. Nrf2 and Cancer
14. Role of Tumor Protein p53 in Cancer
15. Apoptosis (Programmed Cell Death) on Cancer Development

16. The Potential of Herbal Drugs in Chemotherapeutic Regimens
17. Moringa oleifera
18. Anti-Cancer Properties of Moringa oleifera
19. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- World Health Organization. Fact Sheet Detail: Cancer. Available online: https://www.who.int/health-topics/cancer#tab=tab_1 (accessed on 3 April 2022).
- National Cancer Institute. “What is Cancer” NCI 2021. Available online: https://www.cancer.gov/about-cancer/understanding/what-is-cancer#:~:text=Cancer%20is%20a%20disease%20caused,are%20also%20called%20genetic%20changes (accessed on 31 March 2021).
- Ohshika, S.; Saruga, T.; Ogawa, T.; Ono, H.; Ishibashi, Y. Distinction between benign and malignant soft tissue tumors based on an ultrasonographic evaluation of vascularity and elasticity. Oncol. Lett. 2021, 21, 281. [Google Scholar] [CrossRef] [PubMed]
- Institute, N.C. Common Cancer Types. NIH. 2021. Available online: http://www.cancer.gov/types/common-cancers (accessed on 31 March 2021).
- Fayed, L. Benign vs. Malignant Tumors: Causes and Treatments. Very Well Health. Available online: https://www.verywellhealth.com/what-does-malignant-and-benign-mean-514240 (accessed on 1 November 2022).
- Abrahams, B. The effects of various combinations of different classes of anticancer drugs and tyrosine kinase inhibitors on the human MCF-7 breast carcinoma cell line. Ph.D. Thesis, University of the Western Cape, Cape Town, South Africa, 2014. [Google Scholar]
- Waks, A.G.; Winer, E.P. Breast Cancer Treatment: A Review. JAMA 2019, 321, 288–300. [Google Scholar] [CrossRef]
- Seyfried, T.N.; Huysentruyt, L.C. On the origin of cancer metastasis. Crit. Rev. Oncog. 2013, 18, 43–73. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Fact Sheet Detail: Non-Communicable Diseases. Available online: http://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 25 March 2021).
- Lipshultz, S.E.; Franco, V.I.; Henkel, J.M.; Miller, T.L. Cardiovascular effects in childhood cancer survivors treated with anthracyclines. Cardiol. Res. Pract. 2011, 2011, 134679. [Google Scholar]
- McGowan, J.V.; Chung, R.; Maulik, A.; Piotrowska, I.; Walker, J.M.; Yellon, D.M. Anthracycline Chemotherapy and Cardiotoxicity. Cardiovasc. Drugs Ther. 2017, 31, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Johnson-Arbor, K.; Dubey, R. Doxorubicin. In Treasure Island (FL); Broadview Press: Peterborough, UK, 2022. [Google Scholar]
- Sangweni, N.F.; Moremane, M.; Riedel, S.; van Vuuren, D.; Huisamen, B.; Mabasa, L.; Barry, R.; Johnson, R. The Prophylactic Effect of Pinocembrin Against Doxorubicin-Induced Cardiotoxicity in an In Vitro H9c2 Cell Model. Front Pharmacol. 2020, 11, 1172. [Google Scholar] [CrossRef]
- Hortobagyi, G.N. Anthracyclines in the treatment of cancer. Drugs 1997, 54, 1–7. [Google Scholar]
- Abdullah, C.S.; Alam, S.; Aishwarya, R.; Miriyala, S.; Bhuiyan, M.A.N.; Panchatcharam, M.; Pattillo, C.B.; Orr, A.W.; Sadoshima, J.; Hill, J.A.; et al. Doxorubicin-induced cardiomyopathy associated with inhibition of autophagic degradation process and defects in mitochondrial respiration. Sci. Rep. 2019, 9, 2002. [Google Scholar] [CrossRef]
- Ji, X.; Lu, Y.; Tian, H.; Meng, X.; Wei, M.; Cho, W.C. Biomedicine & Pharmacotherapy Chemoresistance mechanisms of breast cancer and their countermeasures. Biomed. Pharmacother. 2019, 114, 108800. [Google Scholar] [CrossRef]
- Inamdar, N.; Edalat, S.; Kotwal, V.B.; Pawar, S. Herbal Drugs in Milieu of Modern Drugs. Int. J. Green Pharm. Aromather. 2009, 2, 2–9. [Google Scholar] [CrossRef]
- Jung, I.L. Soluble extract from Moringa oleifera leaves with a new anticancer activity. PLoS ONE 2014, 9, e95492. [Google Scholar] [CrossRef]
- Greenwell, M.; Rahman, P.K.S.M. Medicinal Plants: Their Use in Anticancer Treatment. Int. J. Pharm. Sci. Res. 2015, 6, 4103–4112. [Google Scholar]
- Mansoori, B.; Mohammadi, A.; Davudian, S.; Shirjang, S.; Baradaran, B. The Different Mechanisms of Cancer Drug Resistance: A Brief Review. Adv. Pharm. Bull. 2017, 7, 339–348. [Google Scholar] [CrossRef]
- Bukowski, K.; Kciuk, M.; Kontek, R. Molecular Sciences Mechanisms of Multidrug Resistance in Cancer Chemotherapy. Available online: www.mdpi.com/journal/ijms (accessed on 1 November 2022).
- Wang, H.; Oo Khor, T.; Shu, L.; Su, Z.Y.; Fuentes, F.; Lee, J.H.; Tony Kong, A.N. Plants vs. cancer: A review on natural phytochemicals in preventing and treating cancers and their drug ability. Anticancer. Agents Med. Chem. 2012, 12, 1281–1305. [Google Scholar] [CrossRef]
- Suphachai, C. Antioxidant and anticancer activities of Moringa oleifera leaves. J. Med. Plants Res. 2014, 8, 318–325. [Google Scholar] [CrossRef]
- Farooq, F.B.; Rai, M.; Tiwari, A.; Khan, A.A.; Farooq, S. Medicinal properties of Moringa oleifera: An overview of promising healer. J. Med. Plants Res. 2012, 6, 4368–4374. [Google Scholar]
- Boutayeb, A.; Boutayeb, S. The burden of non-communicable diseases in developing countries. Int. J. Equity Health 2005, 4, 2. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Editor, G.; Shen, Z. Genomic instability and cancer: An introduction. J. Mol. Cell Biol. 2011, 3, 1–3. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Martin, T.; Ye, L.; AJ, S.; Lane, J.; Jiang, W. Cancer Invasion and Metastasis: Molecular and Cellular Perspective. In Madame Curie Bioscience Database; Landes Bioscience: Austin, TX, USA, 2013; pp. 135–168. [Google Scholar]
- Dersarkissian, C. The Stages of Cancer According to the TNM System. Available online: https://www.webmd.com/cancer/cancer-stages (accessed on 1 November 2022).
- De Palma, M.; Hanahan, D. The biology of personalized cancer medicine: Facing individual complexities underlying hallmark capabilities. Mol. Oncol. 2012, 6, 111–127. [Google Scholar] [CrossRef]
- Yu, L.-H.; Huang, Q.-W.; Zhou, X.-H. Identification of Cancer Hallmarks Based on the Gene Co-expression Networks of Seven Cancers. Front Genet. 2019, 10, 99. [Google Scholar] [CrossRef] [PubMed]
- Iannuccelli, M.; Micarelli, E.; Surdo, P.L.; Palma, A.; Perfetto, L.; Rozzo, I.; Castagnoli, L.; Licata, L.; Cesareni, G. CancerGeneNet: Linking driver genes to cancer hallmarks. Nucleic. Acids. Res. 2020, 48, D416–D421. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Globocan. International Agency for Research on Cancer: South Africa fact sheet. Glob. Cancer Obs. 2020, 491, 1–2. [Google Scholar]
- Momenimovahed, Z.; Salehiniya, H. Epidemiological characteristics of and risk factors for breast cancer in the world. Breast Cancer 2019, 11, 151–164. [Google Scholar] [CrossRef]
- Xi, Y.; Xu, P. Global colorectal cancer burden in 2020 and projections to 2040. Transl. Oncol. 2021, 14, 101174. [Google Scholar] [CrossRef]
- Li, C.I.; Malone, K.E.; Daling, J.R.; Potter, J.D.; Bernstein, L.; Marchbanks, P.A.; Strom, B.L.; Simon, M.S.; Press, M.F.; Ursin, G.; et al. Timing of menarche and first full-term birth in relation to breast cancer risk. Am. J. Epidemiol. 2008, 167, 230–239. [Google Scholar] [CrossRef]
- Iversen, A.; Thune, I.; McTiernan, A.; Emaus, A.; Finstad, S.E.; Flote, V.; Wilsgaard, T.; Lipson, S.F.; Ellison, P.T.; Jasienska, G.; et al. Ovarian hormones and reproductive risk factors for breast cancer in premenopausal women: The Norwegian EBBA-I study. Hum. Reprod. 2011, 26, 1519–1529. [Google Scholar] [CrossRef]
- Dall, G.V.; Britt, K.L. Estrogen Effects on the Mammary Gland in Early and Late Life and Breast Cancer Risk. Front Oncol. 2017, 7, 110. [Google Scholar] [CrossRef]
- Travis, R.C.; Key, T.J. Oestrogen exposure and breast cancer risk. Breast Cancer Res. 2003, 5, 239–247. [Google Scholar] [CrossRef]
- Kotsopoulos, J. Menopausal hormones: Definitive evidence for breast cancer. Lancet 2019, 394, 1116–1118. [Google Scholar] [CrossRef]
- Mohanty, S.S.; Mohanty, P.K. Obesity as potential breast cancer risk factor for postmenopausal women. Genes Dis. 2021, 8, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.H.; Anders, C.K.; Litton, J.K.; Ruddy, K.J.; Bleyer, A. Breast cancer in adolescents and young adults. Pediatr Blood Cancer 2018, 65, e27397. [Google Scholar] [CrossRef]
- Vaz-Luis, I.; Partridge, A.H. Exogenous reproductive hormone use in breast cancer survivors and previvors. Nat. Rev. Clin. Oncol. 2018, 15, 249–261. [Google Scholar] [CrossRef]
- Balekouzou, A.; Yin, P.; Pamatika, C.M.; Bekolo, C.E.; Nambei, S.W.; Djeintote, M.; Kota, K.; Mossoro-Kpinde, C.D.; Shu, C.; Yin, M.; et al. Reproductive risk factors associated with breast cancer in women in Bangui: A case–control study. BMC Womens Health 2017, 17, 14. [Google Scholar] [CrossRef] [PubMed]
- Mattisson, I.; Wirfält, E.; Wallström, P.; Gullberg, B.; Olsson, H.; Berglund, G. High fat and alcohol intakes are risk factors of postmenopausal breast cancer: A prospective study from the Malmö diet and cancer cohort. Int. J. Cancer. 2004, 110, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Simbre, V.C.; Duffy, S.A.; Dadlani, G.H.; Miller, T.L.; Lipshultz, S.E. Cardiotoxicity of cancer chemotherapy: Implications for children. Pediatr Drugs 2005, 7, 187–202. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Holcomb, V.B.; Dang, F.; Porampornpilas, K.; Nunez, N.P. Alcohol consumption, obesity, estrogen treatment and breast cancer. J. Nat. Remedies 2010, 12, 205–218. [Google Scholar]
- Sieri, S.; Chiodini, P.; Agnoli, C.; Pala, V.; Berrino, F.; Trichopoulou, A.; Benetou, V.; Vasilopoulou, E.; Sánchez, M.-J.; Chirlaque, M.-D.; et al. Dietary fat intake and development of specific breast cancer subtypes. J. Natl. Cancer Inst. 2014, 106, dju068. [Google Scholar] [CrossRef]
- Liu, T.; Nguyen, N.; Colditz, G.A. Links between alcohol consumption and breast cancer. Womens Health 2015, 11, 65–77. [Google Scholar]
- Bird, B.R.J.H.; Swain, S.M. Cardiac Toxicity in Breast Cancer Survivors: Review of Potential Cardiac Problems. BMC Complement. Altern. Med. 2008, 14, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Trachtenberg, B.H.; Landy, D.C.; Franco, V.I.; Henkel, J.M.; Pearson, E.J.; Miller, T.L.; Lipshultz, S.E. Anthracycline-associated cardiotoxicity in survivors of childhood cancer. Pediatr. Cardiol. 2011, 32, 342–353. [Google Scholar] [CrossRef]
- Kalyanaraman, B. Redox Biology teaching the basics of the mechanism of doxorubicin-induced cardiotoxicity: Have we been barking up the wrong tree ? Redox Biol. 2020, 29, 101394. [Google Scholar] [CrossRef] [PubMed]
- Alkabban, F.M.; Ferguson, T. Breast Cancer. In Treasure Island (FL); Broadview Press: Peterborough, UK, 2022. [Google Scholar]
- Chalasani, P.; Farr, K.; Wu, V.; Jenkins, I.; Liu, A.; Parker, S.; Gadi, V.K.; Specht, J.; Linden, H. Single arm, phase two study of low-dose metronomic eribulin in metastatic breast cancer. Breast Cancer Res. Treat. 2021, 188, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Choi, L. Breast Cancer-Gynecology and Obstetrics-MSD Manual Professional Edition. Available online: https://www.msdmanuals.com/professional/gynecology-and-obstetrics/breast-disorders/breast-cancer (accessed on 1 November 2022).
- Nurses, O.; Breast, C.A. Oncology Nurses Quality. Available online: http://oncologynurse-ce.com/breast-cancer-pathophysiology/ (accessed on 25 March 2022).
- Loomans-Kropp, H.; Umar, A. Cancer prevention and screening: The next step in the era of precision medicine. NPJ Precis Oncol. 2019, 1, 3. [Google Scholar] [CrossRef]
- McDonald, E.S.; Clark, A.S.; Tchou, J.; Zhang, P.; Freedman, G.M. Clinical Diagnosis and Management of Breast Cancer. J. Nucl. Med. 2016, 57 (Suppl. 1), 9S–16S. [Google Scholar] [CrossRef]
- Casaubon, J.T.; Kashyap, S.; Regan, J.P. BRCA 1 and 2. Stat Pearls. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470239/ (accessed on 1 November 2022).
- Sparano, J.A. Breast Cancer Staging. Medscape. Available online: https://emedicine.medscape.com/article/2007112-overview (accessed on 3 November 2022).
- Park, M.; Kim, D.; Ko, S.; Kim, A.; Mo, K.; Yoon, H. Breast Cancer Metastasis: Mechanisms and Therapeutic Implications. Int. J. Mol. Sci. 2022, 23, 6806. [Google Scholar] [CrossRef]
- Verity, S. What Are the Stages and Grades of Breast Cancer? WebMD. Available online: https://www.webmd.com/breast-cancer/stages-grades-breast-cancer (accessed on 1 January 2022).
- Reilly, R. Breast Cancer. In xPharm: The Comprehensive Pharmacology Reference; Enna, S.J., Bylund, D.B., Eds.; Elsevier: Amsterdam, The Netherlands, 2008; Available online: https://www.sciencedirect.com/science/article/pii/B9780080552323608098 (accessed on 10 January 2022).
- Zhang, Y.; Li, H.; Zhang, J.; Zhao, C.; Lu, S.; Qiao, J.; Han, M. The combinatory effects of natural products and chemotherapy drugs and their mechanisms in breast cancer treatment. Phytochem. Rev. 2020, 19, 1179–1197. [Google Scholar] [CrossRef]
- Metri, K.; Bhargav, H.; Chowdhury, P.; Koka, P.S. Ayurveda for chemo-radiotherapy induced side effects in cancer patients. J. Stem. Cells. 2013, 8, 115–129. [Google Scholar]
- Tang, Y.; Wang, Y.; Kiani, M.F.; Wang, B. Classification, Treatment Strategy, and Associated Drug Resistance in Breast Cancer. Clin. Breast Cancer 2016, 16, 335–343. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Immunotherapy. 2019. Available online: https://www.cancer.org/treatment/treatments-and-side-effects/treatment-types/immunotherapy.html (accessed on 30 November 2021).
- Society, A.C. Targeted Therapy. 2022. Available online: https://www.cancer.gov/about-cancer/treatment/types/targeted-therapies#:~:text=Targeted (accessed on 10 January 2022).
- American Cancer Society. Mastectomy. 2021. Available online: https://www.cancer.org/cancer/breast-cancer/treatment/surgery-for-breast-cancer/mastectomy.html (accessed on 10 January 2022).
- American Cancer Society. Chemotherapy for Breast Cancer. 2021. Available online: https://www.cancer.org/cancer/breast-cancer/treatment/chemotherapy-for-breast-cancer.html (accessed on 10 January 2022).
- Panche, A.N.; Diwan, A.D.; Chandra, S.R. Flavonoids: An Overview. J. Nutr. Sci. 2016, 5, e47. [Google Scholar] [CrossRef] [PubMed]
- Marinello, J.; Delcuratolo, M.; Capranico, G. Anthracyclines as Topoisomerase II Poisons: From Early Studies to New Perspectives. Int. J. Mol. Sci. 2018, 19, 3480. [Google Scholar] [CrossRef] [PubMed]
- Borgatti, A. Chemotherapy. In Washabau; Day, M.J.B.T.-C., Ed.; W.B. Saunders: Saint Louis, PE, USA, 2013; pp. 494–499. [Google Scholar]
- American Cancer Society. Risk of Dying from Cancer Continues to Drop at an Accelerated Pace. Available online: https://www.cancer.org/latest-news/facts-and-figures-2022.html#:~:text=The (accessed on 3 November 2022).
- Siegel, R.L.; Miller, K.; Fuchs, H.; Jemal, A. Cancer statistics. CA: A Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
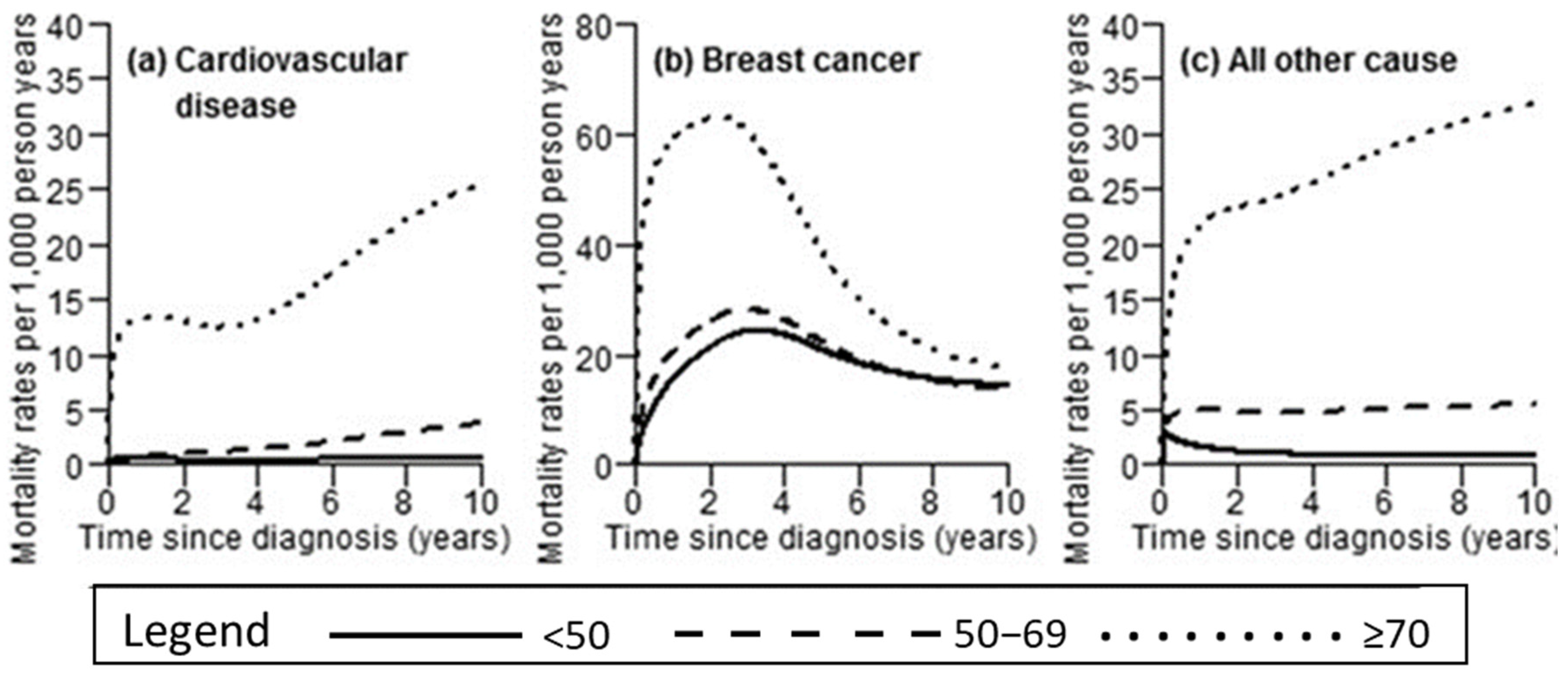
- Berkman, A.; Cole, B.F.; Ades, P.A.; Dickey, S.; Higgins, S.T.; Trentham-Dietz, A.; Sprague, B.L.; Lakoski, S.G. Racial differences in breast cancer, cardiovascular disease, and all-cause mortality among women with ductal carcinoma in situ of the breast. Breast Cancer Res. Treat. 2014, 148, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Gernaat, S.A.M.; Ho, P.J.; Rijnberg, N.; Emaus, M.J.; Baak, L.M.; Hartman, M.; Grobbee, D.E.; Verkooijen, H.M. ‘Risk of death from cardiovascular disease following breast cancer: A systematic review. Breast Cancer Res. Treat. 2017, 164, 537–555. [Google Scholar] [CrossRef] [PubMed]
- Topoisomerase: Definition & Function Study.com. 2017. Available online: https://study.com/academy/lesson/topoisomerase-definition-function.html (accessed on 8 June 2022).
- Octavia, Y.; Tocchetti, C.G.; Gabrielson, K.L.; Janssens, S.; Crijns, H.J.; Moens, A.L. Doxorubicin-induced cardiomyopathy: From molecular mechanisms to therapeutic strategies. J. Mol. Cell Cardiol. 2012, 52, 1213–1225. [Google Scholar] [CrossRef]
- Abd-Rabou, A.A.; Abdalla, A.M.; Ali, N.A.; Zoheir, K.M.A. Moringa oleifera root induces cancer apoptosis more effectively than leave nanocomposites and its free counterpart. Asian Pac. J. Cancer Prev. 2017, 18, 2141–2149. [Google Scholar]
- Hecht, F.; Pessoa, C.F.; Gentile, L.B.; Rosenthal, D.; Carvalho, D.P.; Fortunato, R.S. The role of oxidative stress on breast cancer development and therapy. Tumor. Biol. 2016, 37, 4281–4291. [Google Scholar] [CrossRef]
- Pizzino, G.; Irrera, N.; Cucinotta, M.; Pallio, G.; Mannino, F.; Arcoraci, V.; Squadrito, F.; Altavilla, D.; Bitto, A. Oxidative Stress: Harms and Benefits for Human Health. Oxid. Med. Cell Longev. 2017, 2017, 8416763. [Google Scholar] [CrossRef]
- Ray, P.D.; Huang, B.-W.; Tsuji, Y. Reactive oxygen species (ROS) homeostasis and redox regulation in cellular signaling. Cell Signal. 2012, 24, 981–990. [Google Scholar] [CrossRef] [PubMed]
- Fuchs-tarlovsky, V. Role of antioxidants in cancer therapy. Nutrition 2013, 29, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.-Z.; Yang, S.; Wu, G. Free radicals, antioxidants, and nutrition. Nutrition 2002, 18, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Simpson, T.; Pase, M.P.; Stough, C. Bacopa monnieri as an Antioxidant Therapy to Reduce Oxidative Stress in the Aging Brain. Evid. Based Complement. Altern. Med. 2015, 2015, 615384. [Google Scholar] [CrossRef]
- Aggarwal, V.; Tuli, H.S. Role of Reactive Oxygen Species in Cancer Progression: Molecular Mechanisms and Recent Advancements. Biomolecules 2019, 9, 735. [Google Scholar] [CrossRef]
- Forman, H.J.; Zhang, H.; Rinna, A. Glutathione: Overview of its protective roles, measurement, and biosynthesis. Mol. Asp. Med. 2009, 30, 1–12. [Google Scholar] [CrossRef]
- Harvey, C.J.; Thimmulappa, R.K.; Singh, A.; Blake, D.J.; Ling, G.; Wakabayashi, N.; Fujii, J.; Myers, A.; Biswal, S. Nrf2-regulated glutathione recycling independent of biosynthesis is critical for cell survival during oxidative stress. Free Radic. Biol. Med. 2009, 46, 443–453. [Google Scholar] [CrossRef]
- Zeisel, S.H. Antioxidants Suppress Apoptosis. J. Nutr. 2004, 134, 3179S–3180S. [Google Scholar] [CrossRef]
- Gesellschaft, I.B.L.; Mbh, I. Glutathione Assay. G-Biosciences 2016, 49, 1–16. [Google Scholar]
- Lee, J.D.; Cai, Q.; Shu, X.O.; Nechuta, S.J. The Role of Biomarkers of Oxidative Stress in Breast Cancer Risk and Prognosis: A Systematic Review of the Epidemiologic Literature. J. Women’s Health 2017, 26, 467–482. [Google Scholar] [CrossRef]
- Balendiran, G.K.; Dabur, R.; Fraser, D. The role of glutathione in cancer. Cell Biochem. Funct. 2004, 22, 343–352. [Google Scholar] [CrossRef]
- Ma, Q.; Qiang, M.; Ma, Q. Role of Nrf2 in Oxidative Stress and Toxicity. Annu. Rev. Pharmacol. Toxicol. 2013, 53, 401–426. [Google Scholar] [CrossRef] [PubMed]
- Isnaini, I.; Permatasari, N.; Mintaroem, K.; Prihartini, B.; Widodo, M. Oxidants-Antioxidants Profile in the Breast Cancer Cell Line MCF-7. Asian Pacific. J. Cancer Prev. 2018, 19, 3175–3178. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.M.T.; Shekhar, H.U. Impact of Oxidative Stress on Human Health; Springer: New Delhi, India, 2015; pp. 59–73. [Google Scholar]
- Sultana, D.R.; Shahin, A.D.; Jawadul, H. Measurement of oxidative stress and total antioxidant capacity in hyperthyroid patients following treatment with carbimazole and antioxidant. Heliyon 2022, 8, e08651. [Google Scholar] [CrossRef]
- Griñan-Lison, C.; Blaya-Cánovas, J.L.; López-Tejada, A.; Ávalos-Moreno, M.; Navarro-Ocón, A.; Cara, F.E.; González-González, A.; Lorente, J.A.; Marchal, J.A.; Granados-Principal, S. Antioxidants for the Treatment of Breast Cancer: Are We There Yet ? Antioxidants 2021, 2, 205. [Google Scholar] [CrossRef] [PubMed]
- Hayes, J.D.; Dinkova-Kostova, A.T.; Tew, K.D. Oxidative Stress in Cancer. Cancer Cell 2020, 38, 167–197. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.-H. Oxidative Stress, DNA Damage, and Breast Cancer. AACN Adv. Crit. Care 2002, 13, 540–549. [Google Scholar] [CrossRef]
- Perillo, B.; Di Donato, M.; Pezone, A.; Di Zazzo, E.; Giovannelli, P.; Galasso, G.; Castoria, G.; Migliaccio, A. ROS in cancer therapy: The bright side of the moon. Exp. Mol. Med. 2020, 52, 192–203. [Google Scholar] [CrossRef]
- Slika, H.; Mansour, H.; Wehbe, N.; Nasser, S.A.; Iratni, R.; Nasrallah, G.; Shaito, A.; Ghaddar, T.; Kobeissy, F.; Eid, A.H. Therapeutic potential of flavonoids in cancer: ROS-mediated mechanisms. Biomed. Pharmacother. 2022, 146, 112442. [Google Scholar] [CrossRef]
- Sigounas, G.; Hooker, J.; Anagnostou, A.; Steiner, M. S-allylmercaptocysteine inhibits cell proliferation and reduces the viability of erythroleukemia, breast, and prostate cancer cell lines. Nutr. Cancer 1997, 27, 186–191. [Google Scholar] [CrossRef]
- Prakash, K.; Pirozzi, G.; Elashoff, M.; Munger, W.; Waga, I.; Dhir, R.; Kakehi, Y.; Getzenberg, R.H. Symptomatic and asymptomatic benign prostatic hyperplasia: Molecular differentiation by using microarrays. Proc. Natl. Acad. Sci. USA 2002, 99, 7598–7603. [Google Scholar] [CrossRef] [PubMed]
- Borek, C. Dietary Antioxidants and Human Cancer. Integr. Cancer Ther. 2004, 3, 333–341. [Google Scholar] [CrossRef]
- Xue, D.-F.; Pan, S.-T.; Huang, G.; Qiu, J.-X. ROS enhances the cytotoxicity of cisplatin by inducing apoptosis and autophagy in tongue squamous cell carcinoma cells. Int. J. Biochem. Cell Biol. 2020, 122, 105732. [Google Scholar] [CrossRef] [PubMed]
- Zimta, A.A.; Cenariu, D.; Irimie, A.; Magdo, L.; Nabavi, S.M.; Atanasov, A.G.; Berindan-Neagoe, I. The role of Nrf2 activity in cancer development and progression. Cancers 2019, 11, 1755. [Google Scholar] [CrossRef]
- Lisek, K.; Campaner, E.; Ciani, Y.; Walerych, D.; Del Sal, G. Mutant p53 Tunes the NRF2-Dependent Antioxidant Response to Support Survival of Cancer Cells Vol. 9, Oncotarget; National Laboratory CIB, Area Science Park Padriciano: Trieste, Italy, 2018; pp. 20508–25023. [Google Scholar]
- Hu, J.; Cao, J.; Topatana, W.; Juengpanich, S.; Li, S.; Zhang, B.; Shen, J.; Cai, L.; Cai, X.; Chen, M. Targeting mutant p53 for cancer therapy: Direct and indirect strategies. J. Hematol. Oncol. 2021, 14, 157. [Google Scholar] [CrossRef] [PubMed]
- Diehn, M.; Cho, R.W.; Lobo, N.A.; Kalisky, T.; Dorie, M.J.; Kulp, A.N.; Qian, D.; Lam, J.S.; Ailles, L.E.; Wong, M.; et al. Association of reactive oxygen species levels and radioresistance in cancer stem cells. Nature 2009, 458, 780–783. [Google Scholar] [CrossRef]
- Lo, R.; Matthews, J. The aryl hydrocarbon receptor and estrogen receptor alpha differentially modulate nuclear factor erythroid-2-related factor 2 transactivation in MCF-7 breast cancer cells. Toxicol. Appl. Pharmacol. 2013, 270, 139–148. [Google Scholar] [CrossRef]
- Elmore, S.A. Apoptosis: A Review of Programmed Cell Death. Toxicol. Pathol. 2007, 35, 495–516. [Google Scholar] [CrossRef]
- Fedorova, O.; Daks, A.; Shuvalov, O.; Kizenko, A.; Petukhov, A.; Gnennaya, Y.; Barlev, N. Attenuation of p53 mutant as an approach for treatment Her2-positive cancer. Cell Death Discov. 2020, 6, 100. [Google Scholar] [CrossRef]
- Duffy, M.J.; Synnott, N.C.; Crown, J. Mutant p53 in breast cancer: Potential as a therapeutic target and biomarker. Breast Cancer Res. Treat 2018, 170, 0123456789. [Google Scholar] [CrossRef]
- Ozaki, T.; Nakagawara, A. Role of p53 in cell death and human cancers. Cancers 2011, 3, 994–1013. [Google Scholar] [CrossRef] [PubMed]
- Sreelatha, S.; Jeyachitra, A.; Padma, P.R. Antiproliferation and induction of apoptosis by Moringa oleifera leaf extract on human cancer cells. Food Chem. Toxicol. 2011, 49, 1270–1275. [Google Scholar] [CrossRef] [PubMed]
- Pfeffer, C.M.; Singh, A.T.K. Apoptosis: A target for anticancer therapy. Int. J. Mol. Sci. 2018, 19, 448. [Google Scholar] [CrossRef] [PubMed]
- Jan, R.; Chaudhry, G.-E.-S. Understanding Apoptosis and Apoptotic Pathways Targeted Cancer Therapeutics. Adv. Pharm. Bull. 2019, 9, 205–218. [Google Scholar] [CrossRef] [PubMed]
- Shabalala, S.; Louw, J.; Muller, C.J.F.; Johnson, R. Polyphenols, autophagy and doxorubicin-induced cardiotoxicity. Life Sci. 2017, 180, 160–170. [Google Scholar] [CrossRef]
- Mitry, M.A.; Edwards, J.G. Doxorubicin induced heart failure: Phenotype and molecular mechanisms. IJC Heart Vasc. 2016, 10, 17–24. [Google Scholar] [CrossRef]
- Gungor-Ordueri, N.E.; Kuscu, N.; Tasatargil, A.; Burgucu, D.; Karacan, M.; Celik-Ozenci, C. Doxorubicin-induced testicular damage is related to PARP-1 signaling molecules in mice. Pharmacol. Rep. 2019, 71, 591–602. [Google Scholar] [CrossRef]
- Bouchard, V.J.; Rouleau, M.; Poirier, G.G. PARP-1, a determinant of cell survival in response to DNA damage. Exp. Hematol. 2003, 31, 446–454. [Google Scholar] [CrossRef]
- Thomas, C.; Ji, Y.; Wu, C.; Datz, H.; Boyle, C.; MacLeod, B.; Patel, S.; Ampofo, M.; Currie, M.; Harbin, J.; et al. Hit and run versus long-term activation of PARP-1 by its different domains fine-tunes nuclear processes. Proc. Natl. Acad. Sci. USA 2019, 116, 9941–9946. [Google Scholar] [CrossRef]
- Pascal, J.M. The comings and goings of PARP-1 in response to DNA damage. DNA Repair 2018, 71, 177–182. [Google Scholar] [CrossRef]
- Xie, H.; Wang, W.; Xia, B.; Jin, W.-L.; Lou, G. Therapeutic applications of PARP inhibitors in ovarian cancer. Biomed. Pharmacother. 2020, 15, 127. [Google Scholar] [CrossRef] [PubMed]
- Pacher, P.; Liaudet, L.; Soriano, F.G.; Mabley, J.G.; Szabó, E.; Szabó, C. The role of poly (ADP-ribose) polymerase activation in the development of myocardial and endothelial dysfunction in diabetes. Diabetes 2002, 51, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; Vong, C.T.; Chen, H.; Gao, Y.; Lyu, P.; Qiu, L.; Zhao, M.; Liu, Q.; Cheng, Z.; Zou, J.; et al. Naturally occurring anti-cancer compounds: Shining from Chinese herbal medicine. Chin. Med. 2019, 14, 48. [Google Scholar] [CrossRef] [PubMed]
- Irfan, M.; Javed, Z.; Khan, K.; Khan, N.; Docea, A.O.; Calina, D.; Sharifi-Rad, J.; Cho, W.C. Apoptosis evasion via long non-coding RNAs in colorectal cancer. Cancer Cell Int. 2022, 22, 280. [Google Scholar] [CrossRef] [PubMed]
- HemaIswarya, S.; Doble, M. Potential synergism of natural products in the treatment of cancer. Phytother. Res. 2006, 20, 239–249. [Google Scholar] [CrossRef]
- Kassler, W.J.; Blanc, P.; Greenblatt, R. The use of medicinal herbs by human immunodeficiency virus-infected patients. Arch. Intern. Med. 1991, 151, 2281–2288. [Google Scholar] [CrossRef]
- Burstein, H.J.; Gelber, S.M.S.; Guadagnoli, E.; Weeks, J.C. Use of alternative medicine by women WITH early-stage breast CANCER. N. Engl. J. Med. 1999, 340, 1733–1739. [Google Scholar] [CrossRef]
- Gericke, N.; Albrecht, C.F.; Van Wyk, B.; Mayeng, B.; Mutwa, C.; Hutchings, A. Sutherlandia frutescens. Aust. J. Med. Herbal. 2001, 13, 9–15. [Google Scholar]
- Phulukdaree, A.; Moodley, D.; Chuturgoon, A.A. The effects of Sutherlandia frutescens extracts in cultured renal proximal and distal tubule epithelial cells. S. Afr. J. Sci. 2010, 106, 4–8. [Google Scholar] [CrossRef]
- Eddouks, M.; Chattopadhyay, D.; De Feo, V.; Cho, W.C.S. Medicinal plants in the prevention and treatment of chronic diseases 2013. Evid.-Based Complement. Altern Med. 2014, 2014, 180981. [Google Scholar] [CrossRef]
- Mahmood, K.T.; Mugal, T.; Haq, I.U. Moringa oleifera: A natural gift-a review. J. Pharm. Sci. Res. 2010, 2, 775–781. [Google Scholar]
- Gopalakrishnan, L.; Doriya, K.; Kumar, D.S. Moringa oleifera: A review on nutritive importance and its medicinal application. Food Sci. Hum. Wellness 2016, 5, 49–56. [Google Scholar] [CrossRef]
- Amaglo, N.K.; Bennett, R.N.; Curto, R.B.L.; Rosa, E.A.; Turco, V.L.; Giuffrida, A.; Curto, A.L.; Crea, F.; Timpo, G.M. Profiling selected phytochemicals and nutrients in different tissues of the multipurpose tree Moringa oleifera L., grown in Ghana. Food Chem. 2010, 122, 1047–1054. [Google Scholar] [CrossRef]
- Karim, N.U.; Siddiq, U.S.A.A.; Razak, M.R.M.; Zainol, M.K.M.; Abdullah, M.I. Effects of moringa leaves (Moringa oleifera) extraction on quality changes and melanosis of giant freshwater prawn (Macrobrachium rosenbergii) during chilled storage. Ital. J. Food Saf. 2018, 7, 6846. [Google Scholar] [CrossRef] [PubMed]
- Azlan, U.K.; Mediani, A.; Rohani, E.R.; Tong, X.; Han, R.; Misnan, N.M.; Jam, F.A.; Bunawan, H.; Sarian, M.N.; Hamezah, H.S. A Comprehensive Review with Updated Future Perspectives on the Ethnomedicinal and Pharmacological Aspects of Moringa oleifera. Molecules 2022, 27, 5765. [Google Scholar] [CrossRef] [PubMed]
- Zahirah, N.; Rani, A.; Husain, K.; Kumolosasi, E. Moringa Genus: A Review of Phytochemistry and Pharmacology. Front. Pharmacol. 2018, 9, 108. [Google Scholar]
- Fidrianny, I.; Kanapa, I.; Singgih, M. Phytochemistry and pharmacology of moringa tree: An overview. Biointerface Res. Appl. Chem. 2021, 11, 10776–10789. [Google Scholar]
- Delelegn, A.; Sahile, S.; Husen, A. Water purification and antibacterial efficacy of Moringa oleifera Lam. Agric. Food Secur. 2018, 7, 25. [Google Scholar] [CrossRef]
- Miyoshi, N.; Takabayashi, S.; Osawa, T.; Nakamura, Y. Benzyl isothiocyanate inhibits excessive superoxide generation in inflammatory leukocytes: Implication for prevention against inflammation-related carcinogenesis. Carcinogenesis 2004, 25, 567–575. [Google Scholar] [CrossRef]
- Tiloke, C.; Anand, K.; Gengan, R.M.; Chuturgoon, A.A. Moringa oleifera and their phytonanoparticles: Potential antiproliferative agents against cancer. Biomed. Pharmacother. 2018, 108, 457–466. [Google Scholar] [CrossRef]
- Lee, Y.J.; Shacter, E. Oxidative stress inhibits apoptosis in human lymphoma cells. J. Biol. Chem. 1999, 274, 19792–19798. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Kawakami, M.; Yoshihiro, A.; Miyoshi, N.; Ohigashi, H.; Kawai, K.; Osawa, T.; Uchida, K. Involvement of the mitochondrial death pathway in chemopreventive benzyl isothiocyanate-induced apoptosis. J. Biol. Chem. 2002, 277, 8492–8499. [Google Scholar] [CrossRef] [PubMed]
- Hermawan, A.; Nur, K.A.; Sarmoko Dewi, D.; Putri, P.; Meiyanto, E. Ethanolic Extract of Moringa oleifera Increased Cytotoxic Effect of Doxorubicin on HeLa Cancer Cells. J. Nat. Remedies. 2012, 12, 108–114. [Google Scholar]
- Tumer, T.B.; Rojas-Silva, P.; Poulev, A.; Raskin, I.; Waterman, C. Direct and indirect antioxidant activity of polyphenol- and isothiocyanate-enriched fractions from Moringa oleifera. J. Agric. Food Chem. 2015, 63, 1505–1513. [Google Scholar] [CrossRef] [PubMed]
- Tiloke, C. The Antiproliferative and Apoptosis Inducing Effects of Moringa oleifera Aqueous leaf Extract and Its Synthesised Gold Nanoparticles Modulation of Oncogenes and Tumour Suppressor Genes in Human Cancer Cell Lines; University of Kwa Zulu Natal: Berea, Durban, 2015. [Google Scholar]
- Islam, Z.; Islam, S.M.R.; Hossen, F.; Mahtab-Ul-Islam, K.; Hasan, M.R.; Karim, R. Moringa oleifera is a Prominent Source of Nutrients with Potential Health Benefits. Int. J. food Sci. 2021, 2021, 6627265. [Google Scholar] [CrossRef]
- Vergara-Jimenez, M.; Almatrafi, M.M.; Fernandez, M.L. Bioactive Components in Moringa oleifera Leaves Protect against Chronic Disease. Antioxidants 2017, 6, 91. [Google Scholar] [CrossRef]
- Packialakshmi, N.; Archana, J. Phytochemical analysis and antibacterial activity of Moringa oleifera to treat different kinds of water samples. Int. J. Phytopharm. 2014, 5, 233–238. [Google Scholar]
- Stohs, S.J.; Hartman, M.J. Review of the safety and efficacy of Moringa oleifera. Phyther Res. 2015, 29, 796–804. [Google Scholar] [CrossRef]
- Zordoky, B.N.M.; El-Kadi, A.O.S. Induction of several cytochrome P450 genes by doxorubicin in H9c2 cells. Vasc. Pharmacol. 2008, 49, 166–172. [Google Scholar] [CrossRef]
- Fantoukh, O.I.; Albadry, M.A.; Parveen, A.; Hawwal, M.F.; Majrashi, T.; Ali, Z.; Khan, S.I.; Chittiboyina, A.G.; Khan, I.A. Isolation, synthesis, and drug interaction potential of secondary metabolites derived from the leaves of miracle tree (Moringa oleifera) against CYP3A4 and CYP2D6 isozymes. Phytomedicine 2019, 60, 153010. [Google Scholar] [CrossRef]
- Zunica, E.R.M.; Yang, S.; Coulter, A.; White, C.; Kirwan, J.P.; Gilmore, L.A. Moringa oleifera Seed Extract Concomitantly Supplemented with Chemotherapy Worsens Tumor Progression in Mice with Triple Negative Breast Cancer and Obesity. Nutrients 2021, 13, 2923. [Google Scholar] [CrossRef] [PubMed]
- Asare, G.A.; Gyan, B.; Bugyei, K.; Adjei, S.; Mahama, R.; Addo, P.; Otu-Nyarko, L.; Wiredu, E.K.; Nyarko, A. Toxicity potentials of the nutraceutical Moringa oleifera at supra-supplementation levels. J. Ethnopharmacol. 2012, 139, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Tiloke, C.; Phulukdaree, A.; Chuturgoon, A.A. The antiproliferative effect of Moringa oleifera crude aqueous leaf extract on cancerous human alveolar epithelial cells. BMC Complement. Altern. Med. 2013, 13, 226. [Google Scholar] [CrossRef]
- Luo, H.; Rankin, G.O.; Li, Z.; Depriest, L.; Chen, Y.C. Kaempferol induces apoptosis in ovarian cancer cells through activating p53 in the intrinsic pathway. Food Chem. 2011, 128, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Tiloke, C.; Phulukdaree, A.; Gengan, R.M.; Chuturgoon, A.A. Moringa oleifera Aqueous Leaf Extract Induces Cell-Cycle Arrest and Apoptosis in Human Liver Hepatocellular Carcinoma Cells. Nutr. Cancer 2019, 71, 1165–1174. [Google Scholar] [CrossRef] [PubMed]
- Parvathy, M.V.S.; Umamaheshwari, A. Cytotoxic Effect of Moringa oleifera Leaf Extracts on Human Multiple Myeloma Cell Lines. Trends Med. Res. 2007, 2, 44–50. [Google Scholar]
- Fuel, M.; Mesas, C.; Martínez, R.; Ortiz, R.; Quiñonero, F.; Prados, J.; Porres, J.M.; Melguizo, C. Antioxidant and antiproliferative potential of ethanolic extracts from Moringa oleifera, Tropaeolum tuberosum and Annona cherimola in colorrectal cancer cells. Biomed. Pharmacother. 2021, 143, 112248. [Google Scholar] [CrossRef]
- Berkovich, L.; Earon, G.; Ron, I.; Rimmon, A.; Vexler, A.; Lev-Ari, S. Moringa oleifera aqueous leaf extract down-regulates nuclear factor-kappaB and increases cytotoxic effect of chemotherapy in pancreatic cancer cells. BMC Complement. Altern. Med. 2013, 13, 212. [Google Scholar] [CrossRef]
- Ghosh, N. Anticancer effect of Moringa oleifera leaf extract on human breast cancer cell. Ph.D. Thesis, Jadavpur University Kolkata, Kolkata, India, 2014. Available online: https://www.soursopwarrior.org/wp-content/uploads/2019/09/moringa-breast-anticancer-properties-3.pdf (accessed on 3 April 2022).
- Varalakshmi, K.; Nair, S. Anticancer, cytotoxic potential of Moringa oleifera extracts on HeLa cell line. J. Nat. Pharm. 2011, 2, 138. [Google Scholar] [CrossRef]
- Krishnamurthy, P.T.; Vardarajalu, A.; Wadhwani, A.; Patel, V. Identification and characterization of a potent anticancer fraction from the leaf extracts of Moringa oleifera L. Indian J. Exp. Biol. 2015, 53, 98–103. [Google Scholar]
- Albrahim, T.; Binobead, M.A. Research Article Roles of Moringa oleifera Leaf Extract in Improving the Impact of High Dietary Intake of Monosodium Glutamate-Induced Liver Toxicity. Oxid. Med. Cell Longev. 2018, 2018, 4501097. [Google Scholar] [CrossRef]
- Karim, N.A.A.; Ibrahim, M.D.; Kntayya, S.B.; Rukayadi, Y.; Hamid, H.A.; Razis, A.F.A. Moringa oleifera Lam: Targeting chemoprevention. Asian Pac. J. Cancer Prev. 2016, 17, 3675–3686. [Google Scholar] [PubMed]
- Zhang, D.; Xu, Q.; Wang, N.; Yang, Y.; Liu, J.; Yu, G.; Yang, X.; Xu, H.; Wang, H. A complex micellar system co-delivering curcumin with doxorubicin against cardiotoxicity and tumor growth. Int. J. Nanomed. 2018, 13, 4549–4561. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.-H.; Yang, C.-X.; Zhang, L.; Yang, C.-Y.; Xu, X.-Q. Baicalein, as a Prooxidant, Triggers Mitochondrial Apoptosis in MCF-7 Human Breast Cancer Cells Through Mobilization of Intracellular Copper and Reactive Oxygen Species Generation. OncoTargets Ther. 2019, 12, 10749–10761. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Constituents | Aqueous Extract |
|---|---|
| Alkaloids | ++ |
| Flavanoids | +++ |
| Saponins | +++ |
| Carbohydrates | ++ |
| Tannins | + |
| Steroids | ++ |
| Glycosides | + |
| Gums and mucilage | ++ |
| Lignin | ND |
| Phenols | + |
| Fixed oils and fats | ++ |
| Amino acids and proteins | ++ |
| Experimental Model | MO Dose | Experimental Outcome | Proposed Mechanism | References |
|---|---|---|---|---|
| Human B-lymphocyte plasmacytoma (U266B1 cell line) | Methanol extract IC50: 0.32 μg/mL | Increased cytotoxic activity | Inhibition of cell proliferation | Adapted from [163] |
| Lung cancer (A549 cell line) | Soluble cold distilled water extract 200 μg/mL | Demonstrated anti-cancer activity by reducing the expressions of AKT, NFKB, ERK, and cyclin D1 | Induced apoptosis by activating caspases | Adapted from [18] |
| Lung cancer (A549 cell line) | Water-soluble extract IC50: 166.7 μg/mL | Reduced levels of GSH, induction of DNA damage as a result of decreased levels of PARP-1 and Nrf2 | Apoptosis induced by activation of caspases | Adapted from [160] |
| Colorectal cancer (CRC) cell lines T84, HCT-15, SW480 and HT-29 | Ethanolic seed extract IC50: 0.001 μg/mL | Caspases 9, 8, and 3 overexpression and elevated the production of ROS | Induced apoptosis by autophagy | Adapted from [164] |
| Pancreatic cancer (Panc-1 cell line) | Aqueous leaf extract 0.75 mg/mL | Reduced the p65 expression | Inhibition of cell proliferation | Adapted from [165] |
| Breast adenocarcinoma (MCF-7) and epithelial breast cancer cell line (MDA-MB-231) | Crude methanolic leaf extract 50 and 25 μg/mL | Decreased cell growth | Apoptosis induced in a time- and dose-dependent manner | Adapted from [166] |
| Cervical cancer (HeLa cell line) | Methanol leaf extracts IC50: 70 μg/mL | A decrease in cell viability with increased apoptosis | Apoptosis induced by DNA fragmentation | Adapted from [167] |
| Hepatocarcinoma (HepG2) and breast adenocarcinoma (MCF-7) | Dichloromethane extract 100 μg/mL | Demonstrated anti-cancer activity by reducing mitochondrial membrane potential, cell viability, and increasing DNA damage | Induced apoptosis by up-regulating Bax proteins | Adapted from [82] |
| Hep2 human epidermoid | Methanol extract 200 μg/mL | Induced DNA fragmentation | Induced apoptosis by elevating ROS | Adapted from [168] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moremane, M.M.; Abrahams, B.; Tiloke, C. Moringa oleifera: A Review on the Antiproliferative Potential in Breast Cancer Cells. Curr. Issues Mol. Biol. 2023, 45, 6880-6902. https://doi.org/10.3390/cimb45080434
Moremane MM, Abrahams B, Tiloke C. Moringa oleifera: A Review on the Antiproliferative Potential in Breast Cancer Cells. Current Issues in Molecular Biology. 2023; 45(8):6880-6902. https://doi.org/10.3390/cimb45080434
Chicago/Turabian StyleMoremane, Malebogo M., Beynon Abrahams, and Charlette Tiloke. 2023. "Moringa oleifera: A Review on the Antiproliferative Potential in Breast Cancer Cells" Current Issues in Molecular Biology 45, no. 8: 6880-6902. https://doi.org/10.3390/cimb45080434