
Hidradenitis Suppurativa: Molecular Etiology, Pathophysiology, and Management—A Systematic Review
 , and
, and
Abstract
:1. Introduction
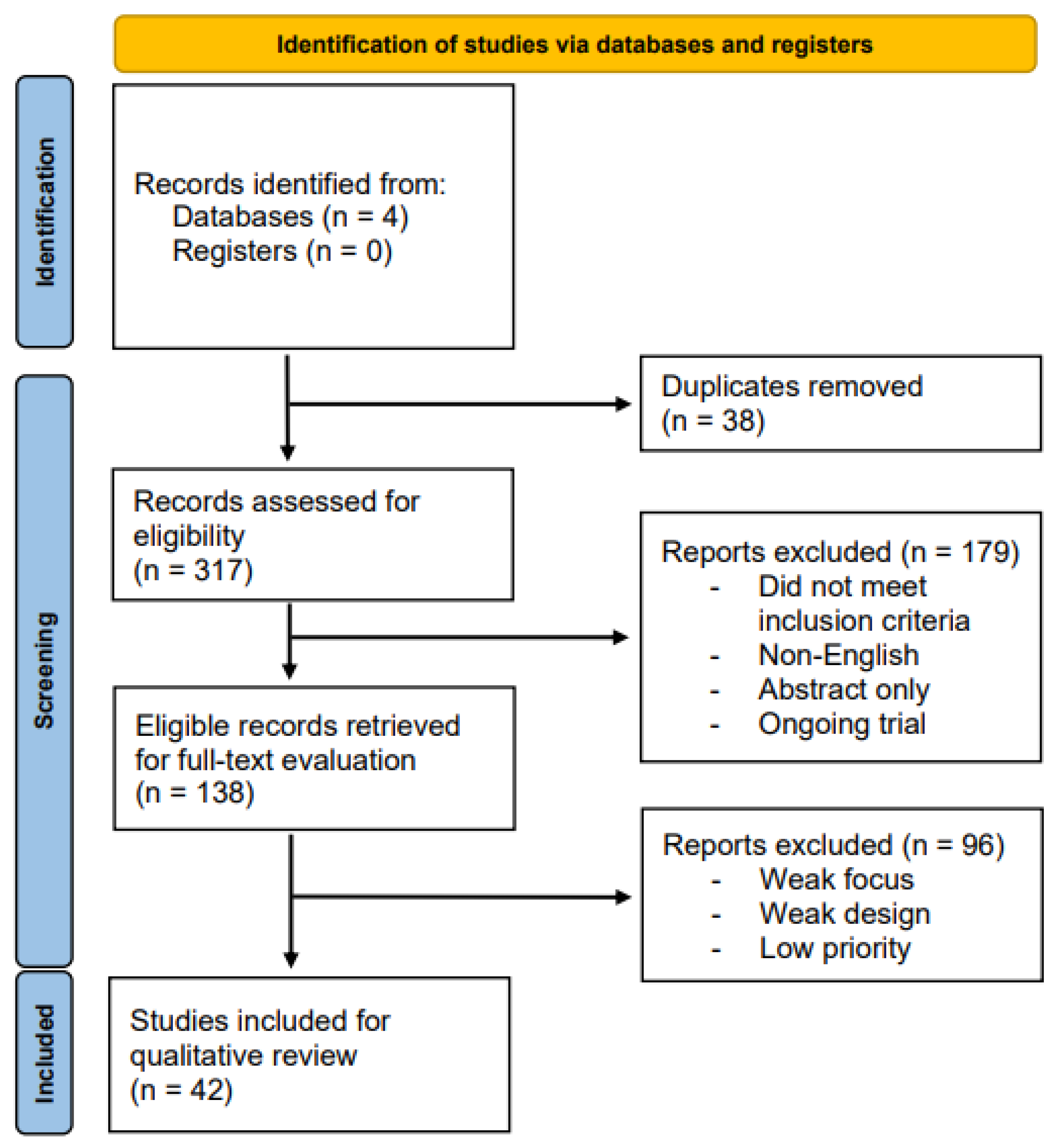
2. Methods
2.1. Study Design
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Data Extraction
3. Results
3.1. Etiology
3.1.1. Environmental Correlation
3.1.2. Genetic Correlation
3.1.3. Hormonal Correlation
3.2. Pathophysiology
3.3. Current Treatment Opportunities
3.3.1. Topical Regimens
3.3.2. Oral Antibiotics
3.3.3. Biologic Agents and Immunomodulatory Drugs
3.4. Emerging Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Reprints
References
- Zouboulis, V.A.; Zouboulis, K.C.; Zouboulis, C.C. Hidradenitis Suppurativa and Comorbid Disorder Biomarkers, Druggable Genes, New Drugs and Drug Repurposing-A Molecular Meta-Analysis. Pharmaceutics 2021, 14, 44. [Google Scholar] [CrossRef]
- Ingram, J.R.; Woo, P.-N.; Chua, S.L.; Ormerod, A.D.; Desai, N.; Kai, A.C.; Hood, K.; Burton, T.; Kerdel, F.; Garner, S.E.; et al. Interventions for hidradenitis suppurativa. Cochrane Database Syst. Rev. 2015, 2015, CD010081. [Google Scholar] [CrossRef]
- Egeberg, A.; Gislason, G.H.; Hansen, P.R. Risk of Major Adverse Cardiovascular Events and All-Cause Mortality in Patients With Hidradenitis Suppurativa. JAMA Dermatol. 2016, 152, 429–434. [Google Scholar] [CrossRef]
- Thorlacius, L.; Cohen, A.D.; Gislason, G.H.; Jemec, G.B.E.; Egeberg, A. Increased Suicide Risk in Patients with Hidradenitis Suppurativa. J. Investig. Dermatol. 2018, 138, 52–57. [Google Scholar] [CrossRef]
- Ingram, J.R. The epidemiology of hidradenitis suppurativa. Br. J. Dermatol. 2020, 183, 990–998. [Google Scholar] [CrossRef] [PubMed]
- Seivright, J.; Collier, E.; Grogan, T.; Shih, T.; Hogeling, M.; Shi, V.Y.; Hsiao, J.L. Pediatric hidradenitis suppurativa: Epidemiology, disease presentation, and treatments. J. Dermatol. Treat. 2022, 33, 2391–2393. [Google Scholar] [CrossRef] [PubMed]
- Seyed Jafari, S.M.; Knüsel, E.; Cazzaniga, S.; Hunger, R.E. A Retrospective Cohort Study on Patients with Hidradenitis Suppurativa. Dermatology 2018, 234, 71–78. [Google Scholar] [CrossRef]
- Seyed Jafari, S.M.; Hunger, R.E.; Schlapbach, C. Hidradenitis Suppurativa: Current Understanding of Pathogenic Mechanisms and Suggestion for Treatment Algorithm. Front. Med. 2020, 7, 68. [Google Scholar] [CrossRef]
- Gierek, M.; Kitala, D.; Łabuś, W.; Szyluk, K.; Niemiec, P.; Ochała-Gierek, G. Impact of Hidradenitis Suppurativa Surgical Treatment on Health-Related Life Quality. J. Clin. Med. 2022, 11, 4327. [Google Scholar] [CrossRef] [PubMed]
- Rosi, E.; Fastame, M.T.; Scandagli, I.; Di Cesare, A.; Ricceri, F.; Pimpinelli, N.; Prignano, F. Insights into the Pathogenesis of HS and Therapeutical Approaches. Biomedicines 2021, 9, 1168. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.; Mulrow, C.; Shamseer, L.; Tetzlaff, J.; Akl, E.; Moher, D.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Covidence Systematic Review Software, Veritas Health Innovation, Melbourne, Australia. Available online: www.covidence.org (accessed on 5 March 2023).
- Tchero, H.; Herlin, C.; Bekara, F.; Fluieraru, S.; Teot, L. Hidradenitis Suppurativa: A Systematic Review and Meta-analysis of Therapeutic Interventions. Indian J. Dermatol. Venereol. Leprol. 2019, 85, 248–257. [Google Scholar] [CrossRef]
- Phan, K.; Charlton, O.; Smith, S.D. Hidradenitis suppurativa and diabetes mellitus: Updated systematic review and adjusted meta-analysis. Clin. Exp. Dermatol. 2019, 44, e126–e132. [Google Scholar] [CrossRef] [PubMed]
- Acharya, P.; Mathur, M. Hidradenitis suppurativa and smoking: A systematic review and meta-analysis. J. Am. Acad. Dermatol. 2020, 82, 1006–1011. [Google Scholar] [CrossRef]
- Tugnoli, S.; Agnoli, C.; Silvestri, A.; Giari, S.; Bettoli, V.; Caracciolo, S. Anger, Emotional Fragility, Self-esteem, and Psychiatric Comorbidity in Patients with Hidradenitis Suppurativa/Acne Inversa. J. Clin. Psychol. Med. Settings 2020, 27, 527–540. [Google Scholar] [CrossRef] [PubMed]
- Salvador-Rodriguez, L.; Montero-Vílchez, T.; Arias-Santiago, S.; Molina-Leyva, A. Paradoxical Hidradenitis Suppurativa in Patients Receiving TNF-α Inhibitors: Case Series, Systematic Review, and Case Meta-Analysis. Dermatology 2020, 236, 307–313. [Google Scholar] [CrossRef]
- Phan, K.; Huo, Y.R.; Charlton, O.; Smith, S.D. Hidradenitis Suppurativa and Thyroid Disease: Systematic Review and Meta-Analysis. J. Cutan. Med. Surg. 2020, 24, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Choi, F.; Lehmer, L.; Ekelem, C.; Mesinkovska, N.A. Dietary and metabolic factors in the pathogenesis of hidradenitis suppurativa: A systematic review. Int. J. Dermatol. 2020, 59, 143–153. [Google Scholar] [CrossRef]
- Molinelli, E.; Brisigotti, V.; Campanati, A.; Sapigni, C.; Giacchetti, A.; Cota, C.; Offidani, A. Efficacy of oral zinc and nicotinamide as maintenance therapy for mild/moderate hidradenitis suppurativa: A controlled retrospective clinical study. J. Am. Acad. Dermatol. 2020, 83, 665–667. [Google Scholar] [CrossRef]
- Phan, K.; Charlton, O.; Smith, S.D. Hidradenitis suppurativa and metabolic syndrome—systematic review and adjusted meta-analysis. Int. J. Dermatol. 2019, 58, 1112–1117. [Google Scholar] [CrossRef]
- de Oliveira, A.S.L.E.; Bloise, G.; Moltrasio, C.; Coelho, A.; Agrelli, A.; Moura, R.; Tricarico, P.M.; Jamain, S.; Marzano, A.V.; Crovella, S.; et al. Transcriptome Meta-Analysis Confirms the Hidradenitis Suppurativa Pathogenic Triad: Upregulated Inflammation, Altered Epithelial Organization, and Dysregulated Metabolic Signaling. Biomolecules 2022, 12, 1371. [Google Scholar] [CrossRef]
- Liu, M.; Degner, J.; Davis, J.W.; Idler, K.B.; Nader, A.; Mostafa, N.M.; Waring, J.F. Identification of HLA-DRB1 association to adalimumab immunogenicity. PLoS ONE 2018, 13, e0195325. [Google Scholar] [CrossRef] [PubMed]
- Gau, S.-Y.; Preclaro, I.A.C.; Wei, J.C.-C.; Lee, C.-Y.; Kuan, Y.-H.; Hsiao, Y.-P.; Juang, S.-E.; Ma, K.S.-K. Risk of psoriasis in people with hidradenitis suppurativa: A systematic review and meta-analysis. Front. Immunol. 2022, 13, 1033844. [Google Scholar] [CrossRef]
- Jiménez-Gallo, D.; de la Varga-Martínez, R.; Ossorio-García, L.; Collantes-Rodríguez, C.; Rodríguez, C.; Linares-Barrios, M. Effects of adalimumab on T-helper-17 lymphocyte- and neutrophil-related inflammatory serum markers in patients with moderate-to-severe hidradenitis suppurativa. Cytokine 2018, 103, 20–24. [Google Scholar] [CrossRef]
- Almuhanna, N.; Finstad, A.; Alhusayen, R. Association between Hidradenitis Suppurativa and Inflammatory Arthritis: A Systematic Review and Meta-Analysis. Dermatology 2021, 237, 740–747. [Google Scholar] [CrossRef] [PubMed]
- Gau, S.-Y.; Chan, W.L.; Tsai, J.-D. Risk of Atopic Diseases in Patients with Hidradenitis Suppurativa: A Systematic Review and Meta-Analysis of Observational Studies. Dermatology 2023, 239, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Gau, S.-Y. Increased risk of renal diseases in people with hidradenitis suppurativa: A systematic review and meta-analysis. Int. J. Dermatol. 2023, 62, e4–e6. [Google Scholar] [CrossRef] [PubMed]
- Phan, K.; Ng, W.H.S.; Lai, B.; Garg, A.; Smith, S.D. Hidradenitis suppurativa and association with stroke: Systematic review and meta-analysis. J. Dermatol. Treat. 2022, 33, 2309–2316. [Google Scholar] [CrossRef]
- Crowley, J.J.; Mekkes, J.R.; Zouboulis, C.C.; Scheinfeld, N.; Kimball, A.; Sundaram, M.; Gu, Y.; Okun, M.M.; Kerdel, F. Association of hidradenitis suppurativa disease severity with increased risk for systemic comorbidities. Br. J. Dermatol. 2014, 171, 1561–1565. [Google Scholar] [CrossRef]
- Ingram, J.R.; Woo, P.N.; Chua, S.L.; Ormerod, A.D.; Desai, N.; Kai, A.C.; Hood, K.; Burton, T.; Kerdel, F.; Garner, S.E.; et al. Interventions for hidradenitis suppurativa: A Cochrane systematic review incorporating GRADE assessment of evidence quality. Br. J. Dermatol. 2016, 174, 970–978. [Google Scholar] [CrossRef]
- Rivitti-Machado, M.C.; Ferreira Magalhães, R.; Souto da Silva, R.; Duarte, G.V.; Bosnich, F.Z.; Tunala, R.G.; Forestiero, F.J. Therapies for hidradenitis suppurativa: A systematic review with a focus on Brazil. Drugs Context 2022, 11, 2021-9-6. [Google Scholar] [CrossRef] [PubMed]
- Delaunay, J.; Villani, A.P.; Guillem, P.; Tristan, A.; Boibieux, A.; Jullien, D. Oral ofloxacin and clindamycin as an alternative to the classic rifampicin-clindamycin in hidradenitis suppurativa: Retrospective analysis of 65 patients. Br. J. Dermatol. 2018, 178, e15–e16. [Google Scholar] [CrossRef] [PubMed]
- Marasca, C.; Annunziata, M.C.; Villani, A.; Volpe, S.; Marasca, D.; Fabbrocini, G. Adalimumab versus Rifampicin Plus Clindamycin for the Treatment of Moderate to Severe Hidradenitis Suppurativa: A Retrospective Study. J. Drugs Dermatol. JDD 2019, 18, 437–438. [Google Scholar] [PubMed]
- Shih, T.; Lee, K.; Grogan, T.; De, D.R.; Shi, V.Y.; Hsiao, J.L. Infliximab in hidradenitis suppurativa: A systematic review and meta-analysis. Dermatol. Ther. 2022, 35, e15691. [Google Scholar] [CrossRef] [PubMed]
- Romaní, J.; Vilarrasa, E.; Martorell, A.; Fuertes, I.; Ciudad, C.; Molina-Leyva, A. Ustekinumab with Intravenous Infusion: Results in Hidradenitis Suppurativa. Dermatology 2020, 236, 21–24. [Google Scholar] [CrossRef]
- Blok, J.L.; Li, K.; Brodmerkel, C.; Horvátovich, P.; Jonkman, M.F.; Horváth, B. Ustekinumab in hidradenitis suppurativa: Clinical results and a search for potential biomarkers in serum. Br. J. Dermatol. 2016, 174, 839–846. [Google Scholar] [CrossRef]
- Thorlacius, L.; Theut Riis, P.; Jemec, G.B.E. Severe hidradenitis suppurativa responding to treatment with secukinumab: A case report. Br. J. Dermatol. 2018, 179, 182–185. [Google Scholar] [CrossRef]
- Kimball, A.B.; Jemec, G.B.E.; Alavi, A.; Reguiai, Z.; Gottlieb, A.B.; Bechara, F.G.; Paul, C.; Giamarellos Bourboulis, E.J.; Villani, A.P.; Schwinn, A.; et al. Secukinumab in moderate-to-severe hidradenitis suppurativa (SUNSHINE and SUNRISE): Week 16 and week 52 results of two identical, multicentre, randomised, placebo-controlled, double-blind phase 3 trials. Lancet 2023, 401, 747–761. [Google Scholar] [CrossRef]
- Kerdel, F.R.; Azevedo, F.A.; Kerdel Don, C.; Don, F.A.; Fabbrocini, G.; Kerdel, F.A. Apremilast for the Treatment of Mild-to-Moderate Hidradenitis Suppurativa in a Prospective, Open-Label, Phase 2 Study. J. Drugs Dermatol. JDD 2019, 18, 170–176. [Google Scholar]
- Porter, M.L.; Salian, P.; Rosales Santillan, M.; Greif, C.; Kimball, A.B. An Open-Label, Prospective, Pilot Study of Hypertonic Saline for Hidradenitis Suppurativa. Dermatol. Surg. Off. Publ. Am. Soc. Dermatol. Surg. 2022, 48, 954–960. [Google Scholar] [CrossRef]
- Morita, A.; Takahashi, H.; Ozawa, K.; Imafuku, S.; Nakama, T.; Takahashi, K.; Matsuyama, T.; Okubo, Y.; Kitamura, S.; Matsuda, N.; et al. Twenty-four-week interim analysis from a phase 3 open-label trial of adalimumab in Japanese patients with moderate to severe hidradenitis suppurativa. J. Dermatol. 2019, 46, 745–751. [Google Scholar] [CrossRef]
- Morita, A.; Takahashi, H.; Ozawa, K.; Imafuku, S.; Takekuni, N.; Takahashi, K.; Matsuyama, T.; Okubo, Y.; Zhao, Y.; Kitamura, S.; et al. Long-term analysis of adalimumab in Japanese patients with moderate to severe hidradenitis suppurativa: Open-label phase 3 results. J. Dermatol. 2021, 48, 3–13. [Google Scholar] [CrossRef] [PubMed]
- van der Zee, H.H.; Longcore, M.; Geng, Z.; Garg, A. Weekly adalimumab treatment decreased disease flare in hidradenitis suppurativa over 36 weeks: Integrated results from the phase 3 PIONEER trials. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1050–1056. [Google Scholar]
- Andersen, P.L.; Riis, P.T.; Thorlacius, L.; Sigsgaard, V.; Nielsen, C.W.; Chafranska, L.; Westergaard, C.; Jemec, G.B.; Saunte, D.M. [Intense pulsed light treatment for hidradenitis suppurativa: A within-person randomized controlled trial]. Eur. J. Dermatol. 2020, 30, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Schultheis, M.; Staubach, P.; Nikolakis, G.; Grabbe, S.; Ruckes, C.; von Stebut, E.; Kirschner, U.; Matusiak, Ł.; Szepietowski, J.C. LAight® Therapy Significantly Enhances Treatment Efficacy of 16 Weeks of Topical Clindamycin Solution in Hurley I and II Hidradenitis Suppurativa: Results from Period A of RELIEVE, a Multicenter Randomized, Controlled Trial. Dermatology 2022, 238, 476–486. [Google Scholar] [CrossRef]
- Schultheis, M.; Staubach, P.; Grabbe, S.; Ruckes, C.; von Stebut, E.; Kirschner, U.; Matusiak, Ł.; Szepietowski, J.C.; Nikolakis, G. LAight® Therapy Is an Effective Treatment Option to Maintain Long-Term Remission of Hurley I and II Hidradenitis Suppurativa: Results from Period B of RELIEVE, a Multicenter Randomized, Controlled Trial. Dermatology 2022, 238, 1092–1103. [Google Scholar] [CrossRef]
- Salvador-Rodríguez, L.; Arias-Santiago, S.; Molina-Leyva, A. Ultrasound-assisted intralesional corticosteroid infiltrations for patients with hidradenitis suppurativa. Sci. Rep. 2020, 10, 13363. [Google Scholar] [CrossRef]
- Ring, H.C.; Egeberg, A.; Zachariae, C.; Thomsen, S.F.; Gyldenløve, M. Considerable improvement in hidradenitis suppurativa with oral roflumilast therapy. Br. J. Dermatol. 2022, 187, 813–815. [Google Scholar] [CrossRef]
- Gierek, M.; Łabuś, W.; Słaboń, A.; Ziółkowska, K.; Ochała-Gierek, G.; Kitala, D.; Szyluk, K.; Niemiec, P. Co-Graft of Acellular Dermal Matrix and Split Thickness Skin Graft-A New Reconstructive Surgical Method in the Treatment of Hidradenitis Suppurativa. Bioengineering 2022, 9, 389. [Google Scholar] [CrossRef] [PubMed]
- Kridin, K.; Shavit, E.; Damiani, G.; Cohen, A.D. Hidradenitis suppurativa and rheumatoid arthritis: Evaluating the bidirectional association. Immunol. Res. 2021, 69, 533–540. [Google Scholar] [CrossRef]
- Tanaka, N.; Fujioka, A.; Tajima, S.; Ishibashi, A.; Hirose, S. Elafin is induced in epidermis in skin disorders with dermal neutrophilic infiltration: Interleukin-1 beta and tumour necrosis factor-alpha stimulate its secretion in vitro. Br. J. Dermatol. 2000, 143, 728–732. [Google Scholar] [CrossRef] [PubMed]
- Melnik, B.C.; Plewig, G. Impaired Notch-MKP-1 signalling in hidradenitis suppurativa: An approach to pathogenesis by evidence from translational biology. Exp. Dermatol. 2013, 22, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Join-Lambert, O.; Ribadeau-Dumas, F.; Jullien, V.; Kitzis, M.-D.; Jais, J.-P.; Coignard-Biehler, H.; Guet-Revillet, H.; Consigny, P.-H.; Delage, M.; Nassif, X.; et al. Dramatic reduction of clindamycin plasma concentration in hidradenitis suppurativa patients treated with the rifampin-clindamycin combination. Eur. J. Dermatol. 2014, 24, 94–95. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author, Year | Study Type | Key Findings |
|---|---|---|
| Acharya, 2020 | Meta-analysis, 25 studies (101,977 patients with HS and 17,194,921 controls without HS) |
|
| Choi, 2020 | Systematic review, 25 studies |
|
| Molinelli, 2020 | Controlled clinical trial, 92 patients affected by Hurley stage I and II HS |
|
| Phan, 2019 | Systemic review, 12 studies |
|
| Phan, 2019 | Meta-analysis, 6 case-control studies |
|
| Phan, 2020 | Meta-analysis, 5 case-controls studies (36,103 HS cases and 170,517 controls) |
|
| Salvador-Rodriguez, 2020 | Systematic review, N = 34 patients receiving TNF-α inhibitor treatment (adalimumab = 21, infliximab = 9, etanercept = 4) |
|
| Tchero, 2019 | Meta-analysis, 13 randomized-controlled trials |
|
| Tugnoli, 2020 | Cross-sectional study, 38 HS subjects (22 F, 16 M), without previous major psychiatric disorders |
|
| Author, Year | Study Design | Key Findings |
|---|---|---|
| Almuhanna, 2021 | Meta-analysis, 7 studies (200,361 HS patients, 385,599 controls) |
|
| Choi, 2020 | Systemic review, 25 studies |
|
| Crowley, 2014 | Phase 2 controlled trial, N = 154 |
|
| de Oliveira, 2022 | Meta-analysis, 3 studies (N = 51) |
|
| Gau, 2022 | Observational study, N = 402,021 |
|
| Gau, 2022 | Meta-analysis, 10 studies (N = 560,000) |
|
| Gau, 2023 | Meta-analysis, 12 studies (N = 196,757) |
|
| Jiménez-Gallo, 2018 | Case-control study, 19 moderate-to-severe HS patients 19 controls |
|
| Liu, 2018 | Meta-analysis, 4 studies (N = 634) |
|
| Phan, 2019 | Meta-analysis, 5 studies (36,103 HS patients, 170,517 controls) |
|
| Phan, 2022 | Meta-analysis, 6 studies |
|
| Salvador-Rodriguez, 2020 | Meta-analysis, 2 studies (N = 34) |
|
| Tugnoli, 2020 | Cross-sectional study, 38 HS patients, 28 controls |
|
| Author, Year | Study Design | Key Findings |
|---|---|---|
| Blok, 2016 | Open-label study, N = 12 |
|
| ||
| Delaunay, 2017 | Retrospective analysis, N = 65 |
|
| Ingram, 2016 | Cochrane review, 12 studies |
|
| Kerdel, 2019 | Prospective, Open-Label, Phase 2 Study, N = 20 |
|
| Kimball, 2023 | Randomized, placebo-controlled, double-blind phase 3 trials N = 541 |
|
| Marasca, 2019 | Single-center retrospective study, 30 patients treated with rifampicin and clindamycin; 30 patients treated with adalimumab. |
|
| Rivitti-Machado, 2022 | Systematic review, 70 studies |
|
| Romaní, 2019 | Multicenter retrospective review, N = 14 |
|
| Shih, 2022 | Systematic review and Meta-analysis, 19 studies (N = 314) |
|
| Tchero, 2019 | Systematic review and Meta-analysis, 13 studies |
|
| Thorlacius, 2018 | Case report |
|
| Author, Year | Study Design | Key Findings |
|---|---|---|
| Gierek, 2022 | Clinical trial, N = 2 |
|
| Morita, 2019 | Controlled trial, N = 15 |
|
| Morita, 2020 | Controlled trial, N = 15 |
|
| Porter, 2022 | Controlled trial, N = 21 |
|
| Ring, 2022 | Case report |
|
| Salvador-Rodriguez, 2020 | Controlled trial, N = 193 |
|
| Schultheis, 2022 | Randomized controlled trial, N = 88 |
|
| Schultheis, 2022 | Randomized controlled trial, N = 78 |
|
| Van der Zee, 2020 | Randomized controlled trial, N = 633 |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diaz, M.J.; Aflatooni, S.; Abdi, P.; Li, R.; Anthony, M.R.; Neelam, S.; Farkouh, C.; Tran, J.T.; Svoboda, S.; Forouzandeh, M.; et al. Hidradenitis Suppurativa: Molecular Etiology, Pathophysiology, and Management—A Systematic Review. Curr. Issues Mol. Biol. 2023, 45, 4400-4415. https://doi.org/10.3390/cimb45050280
Diaz MJ, Aflatooni S, Abdi P, Li R, Anthony MR, Neelam S, Farkouh C, Tran JT, Svoboda S, Forouzandeh M, et al. Hidradenitis Suppurativa: Molecular Etiology, Pathophysiology, and Management—A Systematic Review. Current Issues in Molecular Biology. 2023; 45(5):4400-4415. https://doi.org/10.3390/cimb45050280
Chicago/Turabian StyleDiaz, Michael Joseph, Shaliz Aflatooni, Parsa Abdi, Rina Li, Michelle Robert Anthony, Sphurti Neelam, Chris Farkouh, Jasmine Thuy Tran, Steven Svoboda, Mahtab Forouzandeh, and et al. 2023. "Hidradenitis Suppurativa: Molecular Etiology, Pathophysiology, and Management—A Systematic Review" Current Issues in Molecular Biology 45, no. 5: 4400-4415. https://doi.org/10.3390/cimb45050280