
Mechanism Underlying Triple VEGFR Inhibitor Tivozanib-Induced Hypertension in Mice Model
 ,
,  and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Effect of Tivozanib and/or Losartan on the Survival Probability and Body Weight of the Mice
2.2. Effect of Tivozanib and/or Losartan on the Urine Flow and Levels of Urine Protein
2.3. Effect of Tivozanib and/or Losartan on the Hemodynamic Function and Morphological Changes of the Aorta
2.4. Effect of Tivozanib and/or Losartan on Cardiac and Renal Histopathology
2.5. Effect of Tivozanib and/or Losartan on Production of Angiotensin-II and AT1/AT2 Receptors Expression
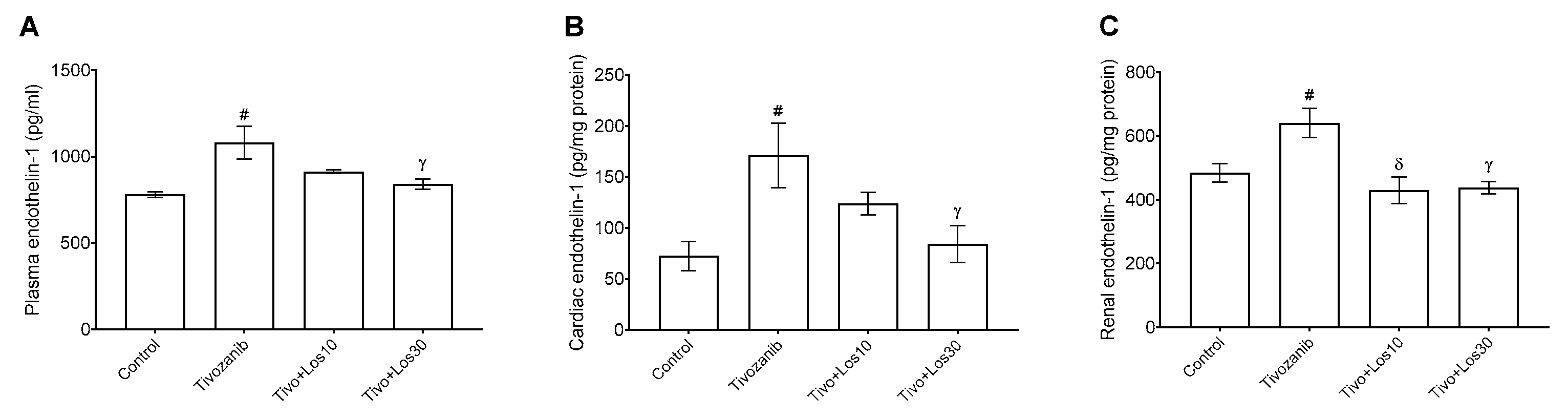
2.6. Effect of Tivozanib and/or Losartan on Production of Endothelin-1 and Nitric Oxide
2.7. Effect of Tivozanib and/or Losartan on Levels of Oxidative Stress Marker in Aorta, Heart and Kidney
3. Discussion
4. Materials and Methods
4.1. Animals and Treatments
4.2. Blood Pressure Measurement Using a Non-Invasive Tail-Cuff System
4.3. Histopathological Analysis
4.4. Measurement of Angiotensin-II and Endothelin-1 Levels Using Enzyme-Linked Immunosorbent Assays
4.5. Nitrite Determination Assay
4.6. Protein Expression of Angiotensin-II Type 1 and 2 Receptors Using Western Blot Analysis
4.7. Measurement of Oxidative Stress Markers Using Biochemical Assays
4.8. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J., Jr.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: Executive summary: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Hypertension 2018, 71, 1269–1324. [Google Scholar] [CrossRef]
- Patel, S.; Rauf, A.; Khan, H.; Abu-izneid, T. Renin-angiotensin-aldosterone (RAAS): The ubiquitous system for homeostasis and pathologies. Biomed. Pharmacother. 2017, 94, 317–325. [Google Scholar] [CrossRef] [PubMed]
- De Mello, W.C.; Frohlich, E.D. Clinical perspectives and fundamental aspects of local cardiovascular and renal Renin-Angiotensin systems. Front. Endocrinol. 2014, 5, 16. [Google Scholar] [CrossRef] [PubMed]
- Ames, M.K.; Atkins, C.E.; Pitt, B. The renin-angiotensin-aldosterone system and its suppression. J. Vet. Intern. Med. 2019, 33, 363–382. [Google Scholar] [CrossRef]
- Laurent, S. Antihypertensive drugs. Pharmacol. Res. 2017, 124, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Dézsi, C.A. The different therapeutic choices with ARBs. Which one to give? When? Why? Am. J. Cardiovasc. Drugs 2016, 16, 255–266. [Google Scholar] [CrossRef]
- Lemmon, M.A.; Schlessinger, J. Cell signaling by receptor tyrosine kinases. Cell 2010, 141, 1117–1134. [Google Scholar] [CrossRef] [PubMed]
- Pottier, C.; Fresnais, M.; Gilon, M.; Jérusalem, G.; Longuespée, R.; Sounni, N.E. Tyrosine kinase inhibitors in cancer: Breakthrough and challenges of targeted therapy. Cancers 2020, 12, 731. [Google Scholar] [CrossRef] [PubMed]
- Tseng, L.C.; Chen, K.H.; Wang, C.L.; Weng, L.C. Effects of tyrosine kinase inhibitor therapy on skin toxicity and skin-related quality of life in patients with lung cancer: An observational study. Medicine 2020, 99, e20510. [Google Scholar] [CrossRef]
- Chaar, M.; Kamta, J.; Ait-Oudhia, S. Mechanisms, monitoring, and management of tyrosine kinase inhibitors–associated cardiovascular toxicities. Onco. Targets Ther. 2018, 11, 6227–6237. [Google Scholar] [CrossRef] [Green Version]
- Ribatti, D.; Solimando, A.G.; Pezzella, F. The anti-VEGF(R) drug discovery legacy: Improving attrition rates by breaking the vicious cycle of angiogenesis in cancer. Cancers 2021, 13, 3433. [Google Scholar] [CrossRef] [PubMed]
- Salgia, N.J.; Zengin, Z.B.; Pal, S.K. Tivozanib in renal cell carcinoma: A new approach to previously treated disease. Ther. Adv. Med. Oncol. 2020, 12, 1758835920923818. [Google Scholar] [CrossRef] [PubMed]
- Wong, H.H.; Eisen, T. Tivozanib for the treatment of metastatic renal cancer. Expert. Rev. Anticancer. Ther. 2013, 13, 649–660. [Google Scholar] [CrossRef] [PubMed]
- Haberkorn, B.C.; Eskens, F.A. Structure, development, preclinical and clinical efficacy of tivozanib (KRN-951, AV-951). Future Oncol. 2013, 9, 13–20. [Google Scholar] [CrossRef]
- American Journal of Health-System Pharmacy. Tivozanib hydrochloride. Am. J. Health Syst. Pharm. 2021, 78, 1354–1358. [Google Scholar] [CrossRef]
- Ba, Z.; Xiao, Y.; He, M.; Liu, D.; Wang, H.; Liang, H.; Yuan, J. Risk factors for the comorbidity of hypertension and renal cell carcinoma in the cardio-oncologic era and treatment for tumor-induced hypertension. Front. Cardiovasc. Med. 2022, 9, 810262. [Google Scholar] [CrossRef]
- Schulz, E.; Gori, T.; Münzel, T. Oxidative stress and endothelial dysfunction in hypertension. Hypertens. Res. 2011, 34, 665–673. [Google Scholar] [CrossRef]
- Higashi, Y.; Maruhashi, T.; Noma, K.; Kihara, Y. Oxidative stress and endothelial dysfunction: Clinical evidence and therapeutic implications. Trends Cardiovasc. Med. 2014, 24, 165–169. [Google Scholar] [CrossRef]
- Li, Q.; Youn, J.Y.; Cai, H. Mechanisms and consequences of endothelial nitric oxide synthase dysfunction in hypertension. J. Hypertens. 2015, 33, 1128–1136. [Google Scholar] [CrossRef]
- Dobbin, S.J.H.; Cameron, A.C.; Petrie, M.C.; Jones, R.J.; Touyz, R.M.; Lang, N.N. Toxicity of cancer therapy: What the cardiologist needs to know about angiogenesis inhibitors. Heart 2018, 104, 1995–2002. [Google Scholar] [CrossRef] [Green Version]
- Kappers, M.H.; van Esch, J.H.; Sluiter, W.; Sleijfer, S.; Danser, A.H.; van den Meiracker, A.H. Hypertension induced by the tyrosine kinase inhibitor sunitinib is associated with increased circulating endothelin-1 levels. Hypertension 2010, 56, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Lankhorst, S.; Kappers, M.H.; van Esch, J.H.; Danser, A.H.; van den Meiracker, A.H. Hypertension during vascular endothelial growth factor inhibition: Focus on nitric oxide, endothelin-1, and oxidative stress. Antioxid. Redox Signal. 2014, 20, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Thijs, A.M.; van Herpen, C.M.; Sweep, F.C.; Geurts-Moespot, A.; Smits, P.; van der Graaf, W.T.; Rongen, G.A. Role of endogenous vascular endothelial growth factor in endothelium-dependent vasodilation in humans. Hypertension 2013, 61, 1060–1065. [Google Scholar] [CrossRef]
- Eechoute, K.; van der Veldt, A.A.; Oosting, S.; Kappers, M.H.; Wessels, J.A.; Gelderblom, H.; Guchelaar, H.J.; Reyners, A.K.; van Herpen, C.M.; Haanen, J.B.; et al. Polymorphisms in endothelial nitric oxide synthase (eNOS) and vascular endothelial growth factor (VEGF) predict sunitinib-induced hypertension. Clin. Pharmacol. Ther. 2012, 92, 503–510. [Google Scholar] [CrossRef]
- Mirabito Colafella, K.M.; Neves, K.B.; Montezano, A.C.; Garrelds, I.M.; van Veghel, R.; de Vries, R.; Uijl, E.; Baelde, H.J.; van den Meiracker, A.H.; Touyz, R.M.; et al. Selective ETA vs. dual ETA/B receptor blockade for the prevention of sunitinib-induced hypertension and albuminuria in WKY rats. Cardiovasc. Res. 2020, 116, 1779–1790. [Google Scholar] [CrossRef]
- Pandey, A.K.; Singhi, E.K.; Arroyo, J.P.; Ikizler, T.A.; Gould, E.R.; Brown, J.; Beckman, J.A.; Harrison, D.G.; Moslehi, J. Mechanisms of VEGF (Vascular Endothelial Growth Factor) inhibitor-associated hypertension and vascular disease. Hypertension 2018, 71, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Pialoux, V.; Foster, G.E.; Ahmed, S.B.; Beaudin, A.E.; Hanly, P.J.; Poulin, M.J. Losartan abolishes oxidative stress induced by intermittent hypoxia in humans. J. Physiol. 2011, 589, 5529–5537. [Google Scholar] [CrossRef]
- Derosa, G.; Mugellini, A.; Pesce, R.M.; D’Angelo, A.; Maffioli, P. Barnidipine compared to lercanidipine in addition to losartan on endothelial damage and oxidative stress parameters in patients with hypertension and type 2 diabetes mellitus. BMC Cardiovasc. Disord. 2016, 16, 66. [Google Scholar] [CrossRef]
- Liang, L.; Yuan, W.; Qu, L.; Li, H.; Zhang, L.; Fan, G.C.; Peng, T. Administration of losartan preserves cardiomyocyte size and prevents myocardial dysfunction in tail-suspended mice by inhibiting p47phox phosphorylation, NADPH oxidase activation and MuRF1 expression. J. Transl. Med. 2019, 17, 279. [Google Scholar] [CrossRef]
- Fortuño, A.; Bidegain, J.; Robador, P.A.; Hermida, J.; López-Sagaseta, J.; Beloqui, O.; Díez, J.; Zalba, G. Losartan metabolite EXP3179 blocks NADPH oxidase-mediated superoxide production by inhibiting protein kinase C: Potential clinical implications in hypertension. Hypertension 2009, 54, 744–750. [Google Scholar] [CrossRef] [Green Version]
- Ceron, C.S.; do Vale, G.T.; Simplicio, J.A.; Passaglia, P.; Ricci, S.T.; Tirapelli, C.R. Data on the effects of losartan on protein expression, vascular reactivity and antioxidant capacity in the aorta of ethanol-treated rats. Data Brief. 2017, 11, 111–116. [Google Scholar] [CrossRef]
- Ateyya, H.; Nader, M.A.; El-Sherbeeny, N.A. Beneficial effects of rosiglitazone and losartan combination in diabetic rats. Can. J. Physiol. Pharmacol. 2018, 96, 215–220. [Google Scholar] [CrossRef]
- Coffman, T.M. The inextricable role of the kidney in hypertension. J. Clin. Investig. 2014, 124, 2341–2347. [Google Scholar] [CrossRef] [PubMed]
- Magder, S. The meaning of blood pressure. Crit. Care 2018, 22, 257. [Google Scholar] [CrossRef] [PubMed]
- Nagata, S.; Kato, J.; Kuwasako, K.; Asami, M.; Kitamura, K. Plasma and tissue concentrations of proangiotensin-12 in rats treated with inhibitors of the renin-angiotensin system. Hypertens. Res. 2012, 35, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Raina, R.; Chauvin, A.; Chakraborty, R.; Nair, N.; Shah, H.; Krishnappa, V.; Kusumi, K. The role of endothelin and endothelin antagonists in chronic kidney disease. Kidney Dis. 2020, 6, 22–34. [Google Scholar] [CrossRef]
- Chang, Y.K.; Choi, H.; Jeong, J.Y.; Na, K.R.; Lee, K.W.; Choi, D.E. Co-inhibition of angiotensin II receptor and endothelin-1 attenuates renal injury in unilateral ureteral obstructed mice. Kidney Blood Press. Res. 2016, 41, 450–459. [Google Scholar] [CrossRef]
- Chou, Y.H.; Chu, T.S.; Lin, S.L. Role of renin-angiotensin system in acute kidney injury-chronic kidney disease transition. Nephrology 2018, 23, 121–125. [Google Scholar] [CrossRef]
- Civieri, G.; Iop, L.; Tona, F. Antibodies against angiotensin II type 1 and endothelin 1 type A receptors in cardiovascular pathologies. Int. J. Mol. Sci. 2022, 23, 927. [Google Scholar] [CrossRef]
- Ma, W.; Liu, M.; Liang, F.; Zhao, L.; Gao, C.; Jiang, X.; Zhang, X.; Zhan, H.; Hu, H.; Zhao, Z. Cardiotoxicity of sorafenib is mediated through elevation of ROS level and CaMKII activity and dysregulation of calcium homoeostasis. Basic Clin. Pharmacol. Toxicol. 2020, 126, 166–180. [Google Scholar] [CrossRef]
- Stępniak, J.; Krawczyk-Lipiec, J.; Lewiński, A.; Karbownik-Lewińska, M. Sorafenib versus Lenvatinib causes stronger oxidative damage to membrane lipids in noncancerous tissues of the thyroid, liver, and kidney: Effective protection by melatonin and indole-3-propionic acid. Biomedicines 2022, 10, 2890. [Google Scholar] [CrossRef] [PubMed]
- Alanazi, W.A.; Alhamami, H.N.; Alharbi, M.; Alhazzani, K.; Alanazi, A.S.; Alsanea, S.; Ali, N.; Alasmari, A.F.; Alanazi, A.Z.; Alotaibi, M.R.; et al. Angiotensin II type 1 receptor blockade attenuates gefitinib-induced cardiac hypertrophy via adjusting angiotensin II-mediated oxidative stress and JNK/P38 MAPK pathway in a rat model. Saudi Pharm. J. 2022, 30, 1159–1169. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.Y.; Choi, M.J.; Ko, T.K.; Lee, N.H.; Kim, O.H.; Cheon, H.G. Angiotensin AT1 receptor antagonism by losartan stimulates adipocyte browning via induction of apelin. J. Biol. Chem. 2020, 295, 14878–14892. [Google Scholar] [CrossRef]
- Albiges, L.; Barthélémy, P.; Gross-Goupil, M.; Negrier, S.; Needle, M.N.; Escudier, B. TiNivo: Safety and efficacy of tivozanib-nivolumab combination therapy in patients with metastatic renal cell carcinoma. Ann. Oncol. 2021, 32, 97–102. [Google Scholar] [CrossRef]
- Kang, S.; Roh, Y.J.; Kim, I.B. Antiangiogenic effects of tivozanib, an oral VEGF receptor tyrosine kinase inhibitor, on experimental choroidal neovascularization in mice. Exp. Eye Res. 2013, 112, 125–133. [Google Scholar] [CrossRef]
- Daugherty, A.; Rateri, D.; Hong, L.; Balakrishnan, A. Measuring blood pressure in mice using volume pressure recording, a tail-cuff method. J. Vis. Exp. 2009, 27, 1291. [Google Scholar] [CrossRef] [Green Version]
- Ouyang, J.; Guzman, M.; Desoto-Lapaix, F.; Pincus, M.R.; Wieczorek, R. Utility of desmin and a Masson’s trichrome method to detect early acute myocardial infarction in autopsy tissues. Int. J. Clin. Exp. Pathol. 2009, 3, 98–105. [Google Scholar]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alanazi, W.A.; Alanazi, A.S.; El-Nagar, D.M.; Aljuraybah, A.M.; Alsanea, S.; Alharbi, M. Mechanism Underlying Triple VEGFR Inhibitor Tivozanib-Induced Hypertension in Mice Model. Pharmaceuticals 2023, 16, 295. https://doi.org/10.3390/ph16020295
Alanazi WA, Alanazi AS, El-Nagar DM, Aljuraybah AM, Alsanea S, Alharbi M. Mechanism Underlying Triple VEGFR Inhibitor Tivozanib-Induced Hypertension in Mice Model. Pharmaceuticals. 2023; 16(2):295. https://doi.org/10.3390/ph16020295
Chicago/Turabian StyleAlanazi, Wael A., Abdulrahman S. Alanazi, Doaa M. El-Nagar, Abdullah M. Aljuraybah, Sary Alsanea, and Metab Alharbi. 2023. "Mechanism Underlying Triple VEGFR Inhibitor Tivozanib-Induced Hypertension in Mice Model" Pharmaceuticals 16, no. 2: 295. https://doi.org/10.3390/ph16020295