
Adverse Events during Vitreoretinal Surgery under Adequacy of Anesthesia Guidance—Risk Factor Analysis

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Subjects
4.2. Assessment of the Surgical Pleth Index
4.3. Assessment of the Occurrence of OCR and PONV
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reibaldi, M.; Fallico, M.; Longo, A.; Avitabile, T.; Astuto, M.; Murabito, P.; Minardi, C.; Bonfiglio, V.; Boscia, F.; Furino, C.; et al. Efficacy of Three Different Prophylactic Treatments for Postoperative Nausea and Vomiting after Vitrectomy: A Randomized Clinical Trial. J. Clin. Med. 2019, 8, 391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heinke, W.; Frank, T.; Meier, P.; Wiegel, M.; Korth, D. Postoperative vomiting after pars plana vitrectomy. Anesthesiol. Reanim. 1996, 21, 47–50. [Google Scholar]
- Sallam, A.A.B.; Donachie, P.H.J.; Williamson, T.; Sparrow, J.M.; Johnston, R.L. The Royal College of Ophthalmologists’ National Ophthalmology Database Study of vitreoretinal surgery: Report 5, Anesthetic Techniques. Br. J. Ophthalmol. 2015, 100, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Cok, O.Y.; Eker, H.E.; Pelit, A.; Canturk, S.; Akin, S.; Aribogan, A.; Arslan, G. The effect of paracetamol on postoperative nausea and vomiting during the first 24 h after strabismus surgery: A prospective, randomised, double-blind study. Eur. J. Anesthesiol. 2011, 28, 836–841. [Google Scholar] [CrossRef]
- Bharti, N.; Chari, P.; Kumar, P. Effect of sevoflurane versus propofol-based anesthesia on the hemodynamic response and recovery characteristics in patients undergoing microlaryngeal surgery. Saudi J. Anesth. 2012, 6, 380–384. [Google Scholar] [CrossRef]
- Bergmann, I.; Göhner, A.; Crozier, T.A.; Hesjedal, B.; Wiese, C.H.; Popov, A.F.; Bauer, M.; Hinz, J.M. Surgical pleth index-guided remifentanil administration reduces remifentanil and propofol consumption and shortens recovery times in outpatient anesthesia. Br. J. Anesth. 2013, 110, 622–628. [Google Scholar] [CrossRef] [Green Version]
- Gruenewald, M.; Harju, J.; Preckel, B.; Molnár, Z.; Yli-Hankala, A.; Rosskopf, F.; Koers, L.; Orban, A.; Bein, B.; AoA Study Group. Comparison of adequacy of anesthesia monitoring with standard clinical practice monitoring during routine general anesthesia: An international, multicentre, single-blinded randomised controlled trial. Eur. J. Anesthesiol. 2021, 38, 73–81. [Google Scholar] [CrossRef]
- Wennervirta, J.; Hynynen, M.; Koivusalo, A.M.; Uutela, K.; Huiku, M.; Vakkuri, A. Surgical stress index as a measure of nocicep-tion/antinociception balance during general anesthesia. Acta Anesthesiol. Scand. 2008, 52, 1038–1045. [Google Scholar] [CrossRef]
- Ahonen, J.; Jokela, R.; Uutela, K.; Huiku, M. Surgical stress index reflects surgical stress in gynaecological laparoscopic day-case surgery. Br. J. Anesth. 2007, 98, 456–461. [Google Scholar] [CrossRef] [Green Version]
- Gruenewald, M.; Meybohm, P.; Ilies, C.; Höcker, J.; Hanss, R.; Scholz, J.; Bein, B. Influence of different remifentanil concentrations on the performance of the surgical stress index to detect a standardized painful stimulus during sevoflurane anesthesia. Br. J. Anesth. 2009, 103, 586–593. [Google Scholar] [CrossRef] [Green Version]
- Stasiowski, M.; Pluta, A.; Lyssek-Boroń, A.; Kawka, M.; Krawczyk, L.; Niewiadomska, E.; Dobrowolski, D.; Rejdak, R.; Król, S.; Żak, J.; et al. Preventive Analgesia, Hemodynamic Stability, and Pain in Vitreoretinal Surgery. Medicina 2021, 57, 262. [Google Scholar] [CrossRef]
- Pluta, A.; Stasiowski, M.J.; Lyssek-Boroń, A.; Król, S.; Krawczyk, L.; Niewiadomska, E.; Żak, J.; Kawka, M.; Dobrowolski, D.; Grabarek, B.O.; et al. Adverse Events during Vitrectomy under Adequacy of Anesthesia—An Additional Report. J. Clin. Med. 2021, 10, 4172. [Google Scholar] [CrossRef] [PubMed]
- Pluta, M.; Krzych, Ł.J. Użyteczność punktacji Apfel w przewidywaniu pooperacyjnych nudności i wymiotów—Doświadczenia jednego ośrodka. Ann. Acad. Med. Siles 2018, 72, 224–229. [Google Scholar] [CrossRef]
- Ali-Melkkilä, T.; Kanto, J.; Katevuo, R. Tropisetron and metoclopramide in the prevention of postoperative nausea and vomit-ing. A comparative, placebo controlled study in patients undergoing ophthalmic surgery. Anesthesia 1996, 51, 232–235. [Google Scholar]
- Bruderer, U.; Fisler, A.; Steurer, M.P.; Steurer, M.; Dullenkopf, A. Post-discharge nausea and vomiting after total intravenous anesthesia and standardised PONV prophylaxis for ambulatory surgery. Acta Anesthesiol. Scand. 2017, 61, 758–766. [Google Scholar] [CrossRef]
- Apfel, C.C.; Korttila, K.; Abdalla, M.; Kerger, H.; Turan, A.; Vedder, I.; Zernak, C.; Danner, K.; Jokela, R.; Pocock, S.J.; et al. A factorial trial of six interventions for the prevention of postop-erative nausea and vomiting. N. Engl. J. Med. 2004, 350, 2441–2451. [Google Scholar] [CrossRef] [Green Version]
- Weibel, S.; Rücker, G.; Eberhart, L.H.; Pace, N.L.; Hartl, H.M.; Jordan, O.L.; Mayer, D.; Riemer, M.; Schaefer, M.S.; Raj, D.; et al. Drugs for preventing postoperative nausea and vomiting in adults after general anesthesia: A network meta-analysis. Cochrane Database Syst. Rev. 2020, 10, CD012859. [Google Scholar] [CrossRef]
- Nitahara, K.; Sugi, Y.; Shono, S.; Hamada, T.; Higa, K. Risk factors for nausea and vomiting following vitrectomy in adults. Eur. J. Anesthesiol. 2007, 24, 166–170. [Google Scholar]
- Iwamoto, K.; Schwartz, H. Antiemetic Effect of Droperidol After Ophthalmic Surgery. Arch. Ophthalmol. 1978, 96, 1378–1379. [Google Scholar] [CrossRef]
- Quinn, A.C.; Brown, J.H.; Wallace, P.G.; Asbury, A.J. Studies in postoperative sequelae. Nausea and vomiting-still a problem. Anesthesia 1994, 49, 62–65. [Google Scholar] [CrossRef]
- Koivuranta, M.; Läärä, E.; Snåre, L.; Alahuhta, S. A survey of postoperative nausea and vomiting. Anesthesia 1997, 52, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Apfel, C.C.; Greim, C.A.; Haubitz, I.; Goepfert, C.; Usadel, J.; Sefrin, P.; Roewer, N. A risk score to predict the probability of postoperative vomiting in adults. Acta Anesthesiol. Scand. 1998, 42, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Apfel, C.C.; Kranke, P.; Katz, M.H.; Goepfert, C.; Papenfuss, T.; Rauch, S.; Heineck, R.; Greim, C.-A.; Roewer, N. Volatile anesthetics may be the main cause of early but not delayed postoperative vomiting: A randomized controlled trial of factorial design. Br. J. Anesth. 2002, 88, 659–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borgeat, A.; Stirnemann, H.R. Antiemetische Wirkung von Propofol [Antiemetic effect of propofol]. Anesthesist 1998, 47, 918–924. [Google Scholar] [CrossRef]
- Ewalenko, P.; Janny, S.; Dejonckheere, M.; Andry, G.; Wyns, C. Antiemetic effect of subhypnotic doses of propofol after thyroidectomy. Br. J. Anesth. 1996, 77, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Niu, K.; Liu, H.; Chen, R.W.; Fang, Q.W.; Wen, H.; Guo, S.M.; Williams, J.P.; An, J.X. Use of propofol for prevention of post-delivery nausea during cesarean section: A double-blind, randomized, placebo-controlled trial. J. Anesth. 2018, 32, 748–755. [Google Scholar] [CrossRef] [Green Version]
- Khalid, A.; Siddiqui, S.Z.; Aftab, S.; Sabbar, S.; Haider, S. Recovery profile—A comparison of isoflurane and propofol anesthesia for laparoscopic cholecystectomy. J. Coll. Physicians Surg. Pak. 2008, 18, 329–333. [Google Scholar]
- Xie, D.; Zhao, J.; Guo, R.; Jiao, L.; Zhang, Y.; Lau, W.B.; Lopez, B.; Christopher, T.; Gao, E.; Cao, J.; et al. Sevoflurane Pre-conditioning Ameliorates Diabetic Myocardial Ischemia/Reperfusion Injury Via Differential Regulation of p38 and ERK. Sci. Rep. 2020, 10, 23. [Google Scholar] [CrossRef]
- Watcha, M.F.; White, P.F. Postoperative nausea and vomiting: Its etiology, treatment, and prevention. Anesthesiology 1992, 77, 162–184. [Google Scholar] [CrossRef]
- Kranke, P.; Apfel, C.C.; Papenfuss, T.; Rauch, S.; Löbmann, U.; Rübsam, B.; Greim, C.-A.; Roewer, N. An increased body mass index is no risk factor for postoperative nausea and vomiting. A systematic review and results of original data. Acta Anesth. Scand. 2001, 45, 160–166. [Google Scholar] [CrossRef]
- Kim, J.H.; Hong, M.; Kim, Y.J.; Lee, H.S.; Kwon, Y.S.; Lee, J.J. Effect of Body Mass Index on Postoperative Nausea and Vomiting: Propensity Analysis. J. Clin. Med. 2020, 9, 1612. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.M.; Duncan, P.G.; DeBoer, D.P.; Tweed, W.A. The postoperative interview: Assessing risk factors for nausea and vomiting. Anesth. Analg. 1994, 78, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Stadler, M.; Bardiau, F.; Seidel, L.; Albert, A.; Boogaerts, J.G. Difference in Risk Factors for Postoperative Nausea and Vomiting. Anesthesiology 2003, 98, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Allison, C.E.; De Lange, J.J.; Koole, F.D.; Zuurmond, W.W.; Ros, H.H.; van Schagen, N.T. A comparison of the incidence of the oculocardiac and oculorespiratory reflexes during sevoflurane or halothane anesthesia for strabismus surgery in children. Anesth. Analg. 2000, 90, 306–310. [Google Scholar] [PubMed]
- Carlisle, J.B.; Stevenson, C.A. Drugs for preventing postoperative nausea and vomiting. Cochrane Database Syst. Rev. 2006, 3, CD004125. [Google Scholar]
- Mandelcorn, M.; Taback, N.; Mandelcorn, E.; Ananthanarayan, C. Risk factors for pain and nausea following retinal and vitreous surgery under conscious sedation. Can. J. Ophthalmol. 1999, 34, 281–285. [Google Scholar]
- Mallick-Searle, T.; Fillman, M. The pathophysiology, incidence, impact, and treatment of opioid-induced nausea and vomiting. J. Am. Assoc. Nurse Pract. 2017, 29, 704–710. [Google Scholar] [CrossRef]
- Chang, D.J.; Desjardins, P.J.; Bird, S.R.; Black, P.; Chen, E.; Petruschke, R.A.; Geba, G.P. Comparison of rofecoxib and a multidose oxycodone/acetaminophen regimen for the treatment of acute pain following oral surgery: A randomized con-trolled trial. Curr. Med. Res. Opin. 2004, 20, 939–949. [Google Scholar] [CrossRef]
- Daniels, S.; Casson, E.; Stegmann, J.-U.; Oh, C.; Okamoto, A.; Rauschkolb, C.; Upmalis, D. A randomized, double-blind, placebo-controlled phase 3 study of the relative efficacy and tolerability of tapentadol IR and oxycodone IR for acute pain. Curr. Med. Res. Opin. 2009, 25, 1551–1561. [Google Scholar] [CrossRef]
- Gan, T.J.; Diemunsch, P.; Habib, A.S.; Kovac, A.; Kranke, P.; Meyer, T.A.; Watcha, M.; Chung, F.; Angus, S.; Apfel, C.C.; et al. Consensus Guidelines for the Management of Postoperative Nausea and Vomiting. Anesth. Analg. 2014, 118, 85–113. [Google Scholar] [CrossRef] [Green Version]
- Apfel, C.C.; Turan, A.; Souza, K.; Pergolizzi, J.; Hornuss, C. Intravenous acetaminophen reduces postoperative nausea and vomiting: A systematic review and meta-analysis. Proc. Natl. Acad. Sci. USA 2013, 154, 677–689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefánsson, E. Diabetic macular edema. Saudi J. Ophthalmol. 2009, 23, 143–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribeiro, J.A.S.; Ribeiro, D.S.; Scott, I.U.; Abrão, J.; Jorge, R. Pain during pars plana vitrectomy following sub-Tenon versus peribulbar anesthesia: A randomized trial. PLoS ONE 2020, 15, e0236624. [Google Scholar] [CrossRef] [PubMed]
- Ostri, C.; la Cour, M.; Lund-Andersen, H. Diabetic vitrectomy in a large type 1 diabetes patient population: Long-term incidence and risk factors. Acta Ophthalmol. 2013, 92, 439–443. [Google Scholar] [CrossRef]
- Wilkes, S.R. Current therapy of diabetic retinopathy: Laser and vitreoretinal surgery. J. Natl. Med. Assoc. 1993, 85, 841–847. [Google Scholar]
- Cherian, D.; Parkman, H.P. Nausea and vomiting in diabetic and idiopathic gastroparesis. Neurogastroenterol. Motil. 2012, 24, 217-e103. [Google Scholar] [CrossRef]
- Parkman, H.P.; Hallinan, E.K.; Hasler, W.L.; Farrugia, G.; Koch, K.L.; Calles, J.; Snape, W.J.; Abell, T.L.; Sarosiek, I.; McCallum, R.W.; et al. Nausea and vomiting in gastroparesis: Similarities and differences in idiopathic and diabetic gastroparesis. Neurogastroenterol. Motil. 2016, 28, 1902–1914. [Google Scholar] [CrossRef]
- Fleischer, J. Diabetic Autonomic Imbalance and Glycemic Variability. J. Diabetes Sci. Technol. 2012, 6, 1207–1215. [Google Scholar] [CrossRef] [Green Version]
- McCaul, C.; Moran, C.; O’Cronin, D.; Naughton, F.; Geary, M.; Carton, E.; Gardiner, J. Intravenous fluid loading with or without supplementary dextrose does not prevent nausea, vomiting and pain after laparoscopy. Can. J. Anesth. 2003, 50, 440–444. [Google Scholar] [CrossRef]
- Haentjens, L.L.; Ghoundiwal, D.; Touhiri, K.; Renard, M.; Engelman, E.; Anaf, V.; Simon, P.; Barvais, L.; Ickx, B.E. Does infusion of colloid influence the occur-rence of postoperative nausea and vomiting after elective surgery in women? Anesth. Analg. 2009, 108, 1788–1793. [Google Scholar] [CrossRef]
- Dagher, C.F.; Abboud, B.; Richa, F.; Abouzeid, H.; El-Khoury, C.; Doumit, C.; Yaghi, C.; Yazbeck, P. Effect of intravenous crystalloid infusion on postoperative nausea and vomiting after thyroidectomy: A prospective, randomized, controlled study. Eur. J. Anesthesiol. 2009, 26, 188–191. [Google Scholar] [CrossRef] [PubMed]
- Kovac, A.L. Postoperative Nausea and Vomiting in Pediatric Patients. Pediatr. Drugs 2021, 23, 11–37. [Google Scholar] [CrossRef] [PubMed]
- Apfel, C.C.; Läärä, E.; Koivuranta, M.; Greim, C.A.; Roewer, N. A simplified risk score for predicting postoperative nausea and vomiting: Conclusions from cross-validations between two centers. Anesthesiology 1999, 91, 693–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apfel, C.C.; Meyer, A.; Orhan-Sungur, M.; Jalota, L.; Whelan, R.P.; Jukar-Rao, S. Supplemental intravenous crystalloids for the prevention of postoperative nausea and vomiting: Quantitative review. Br. J. Anesth. 2012, 108, 893–902. [Google Scholar] [CrossRef] [Green Version]
- Ali, S.Z.; Taguchi, A.; Holtmann, B.; Kurz, A. Effect of supplemental pre-operative fluid on postoperative nausea and vomiting. Anesthesia 2003, 58, 780–784. [Google Scholar] [CrossRef] [PubMed]
- Ruta, U.; Möllhoff, T.; Markodimitrakis, H.; Brodner, G. Attenuation of the oculocardiac reflex after topically applied lignocaine during surgery for strabismus in children. Eur. J. Anesthesiol. 1996, 13, 11–15. [Google Scholar] [CrossRef]
- Sajedi, P.; Nejad, M.S.; Montazeri, K.; Baloochestani, E. Comparing the preventive effect of 2 percent topical lidocaine and intra-venous atropine on oculocardiac reflex in ophthalmological surgeries under general anesthesia. Int. J. Prev. Med. 2013, 4, 1258–1265. [Google Scholar]
- Grant, M.C.; Kim, J.; Page, A.J.; Hobson, D.; Wick, E.; Wu, C.L. The Effect of Intravenous Midazolam on Postoperative Nausea and Vomiting: A Meta-Analysis. Anesth. Analg. 2016, 122, 656–663. [Google Scholar] [CrossRef]
- Ledowski, T.; Burke, J.; Hruby, J. Surgical pleth index: Prediction of postoperative pain and influence of arousal. Br. J. Anesth. 2016, 117, 371–374. [Google Scholar] [CrossRef] [Green Version]
- Stasiowski, M.; Missir, A.; Pluta, A.; Szumera, I.; Stasiak, M.; Szopa, W.; Błaszczyk, B.; Możdżyński, B.; Majchrzak, K.; Tymowski, M.; et al. Influence of infiltration anesthesia on perioperative outcomes following lumbar discectomy under surgical pleth index-guided general anesthesia: A preliminary report from a randomised controlled prospective trial. Adv. Med. Sci. 2020, 65, 149–155. [Google Scholar] [CrossRef]
- Stasiowski, M.; Starzewska, M.; Niewiadomska, E.; Król, S.; Marczak, K.; Żak, J.; Pluta, A.; Eszyk, J.; Grabarek, B.; Szumera, I.; et al. Adequacy of Anesthesia Guidance for Colonoscopy Procedures. Pharmaceuticals 2021, 14, 464. [Google Scholar] [CrossRef] [PubMed]
- Stasiowski, M.J.; Szumera, I.; Wardas, P.; Król, S.; Żak, J.; Missir, A.; Pluta, A.; Niewiadomska, E.; Krawczyk, L.; Jałowiecki, P.; et al. Adequacy of Anesthesia and Pupillometry for Endoscopic Sinus Surgery. J. Clin. Med. 2021, 10, 4683. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, R.C. Techniques of orbital regional anesthesia. Br. J. Anesth. 1995, 75, 88–92. [Google Scholar] [CrossRef]
- Gruenewald, M.; Ilies, C. Monitoring the nociception–anti-nociception balance. Best Pract. Res. Clin. Anesthesiol. 2013, 27, 235–247. [Google Scholar] [CrossRef] [PubMed]
- Kusza, K.; Kübler, A.; Maciejewski, D.; Mikstacki, A.; Owczuk, R.; Wujtewicz, M.; Piechota, M. Guidelines of the Polish Soci-ety of Anesthesiology and Intensive Therapy determining principles, conditions and organisational aspects of anesthesiol-ogy and intensive therapy services. Anesthesiol. Intensive Ther. 2013, 44, 201–212. [Google Scholar]
- Abouammoh, M.A.; Abdelhalim, A.A.; Mohamed, E.A.; Elzoughari, I.; Mustafa, M.; Al-Zahrani, T.A. Subtenon block com-bined with general anesthesia for vitreoretinal surgery improves postoperative analgesia in adult: A randomized controlled trial. J. Clin. Anesth. 2016, 30, 78–86. [Google Scholar] [CrossRef]
- Misiołek, H.; Cettler, M.; Woroń, J.; Wordliczek, J.; Dobrogowski, J.; Mayzner-Zawadzka, E. The 2014 guidelines for post-operative pain management. Anesthesiol. Intensive Ther. 2014, 46, 221–244. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | Total n = 175 (100%) | GA Group n = 35 (20%) | M Group n = 35 (20%) | P Group n = 35 (20%) | PBB Group n = 35 (20%) | T Group n = 35 (20%) | p-Value |
|---|---|---|---|---|---|---|---|
| Total n = 175 (100%) | 129.9 + 108.2 100 (150) | 144.3 + 102.7 150 (150) | 165.7 + 116.8 200 (200) | 95.7 + 81.7 100 (50) | 95.1 + 101.3 50 (150) | 148.6 + 120.3 150 (200) | p = 0.02 M vs. PBB * |
| Mean intraoperative FNT requirement in patients with overall PONV | 143.8 + 99.8 175 (200) | 137.5 + 62.9 150 (75) | 250 + 0 250 (0) | 150 + 0 150 (0) | 100 + 141.4 100 (200) | 143.8 + 120.8 200 (250) | p = 0.65 NS |
| Mean intraoperative FNT requirement in patients without overall PONV | 128.5 + 109.3 100 (150) | 145.2 + 107.5 150 (150) | 163.2 + 117.6 175 (200) | 94.1 + 82.4 100 (50) | 94.8 + 101.4 50 (150) | 150 + 122.5 100 (200) | p = 0.08 NS |
| p-value | p = 0.48 NS | p = 0.94 NS | - | - | - | p = 0.83 NS | p = 0.99 NS |
| Mean intraoperative FNT requirement in patients with OCR | 127.6 + 96.5 100 (150) | 100 + 70.7 75 (100) | 141.7 + 91.7 150 (100) | 87.5 + 47.9 75 (75) | 82.5 + 88.8 65 (135) | 250 + 132.3 200 (250) | p = 0.25 NS |
| Mean intraoperative FNT requirement in patients without OCR | 130.2 + 110 100 (150) | 150 + 105.7 150 (150) | 170.7 + 122.1 200 (200) | 96.8 + 85.6 100 (50) | 96.8 + 104 50 (150) | 139.1 + 116.9 100 (200) | p = 0.04 M vs. PBB * |
| p-value | p = 0.91 NS | p = 0.42 NS | p = 0.69 NS | p = 0.96 NS | p = 0.89 NS | p = 0.21 NS | p = 0.34 NS |
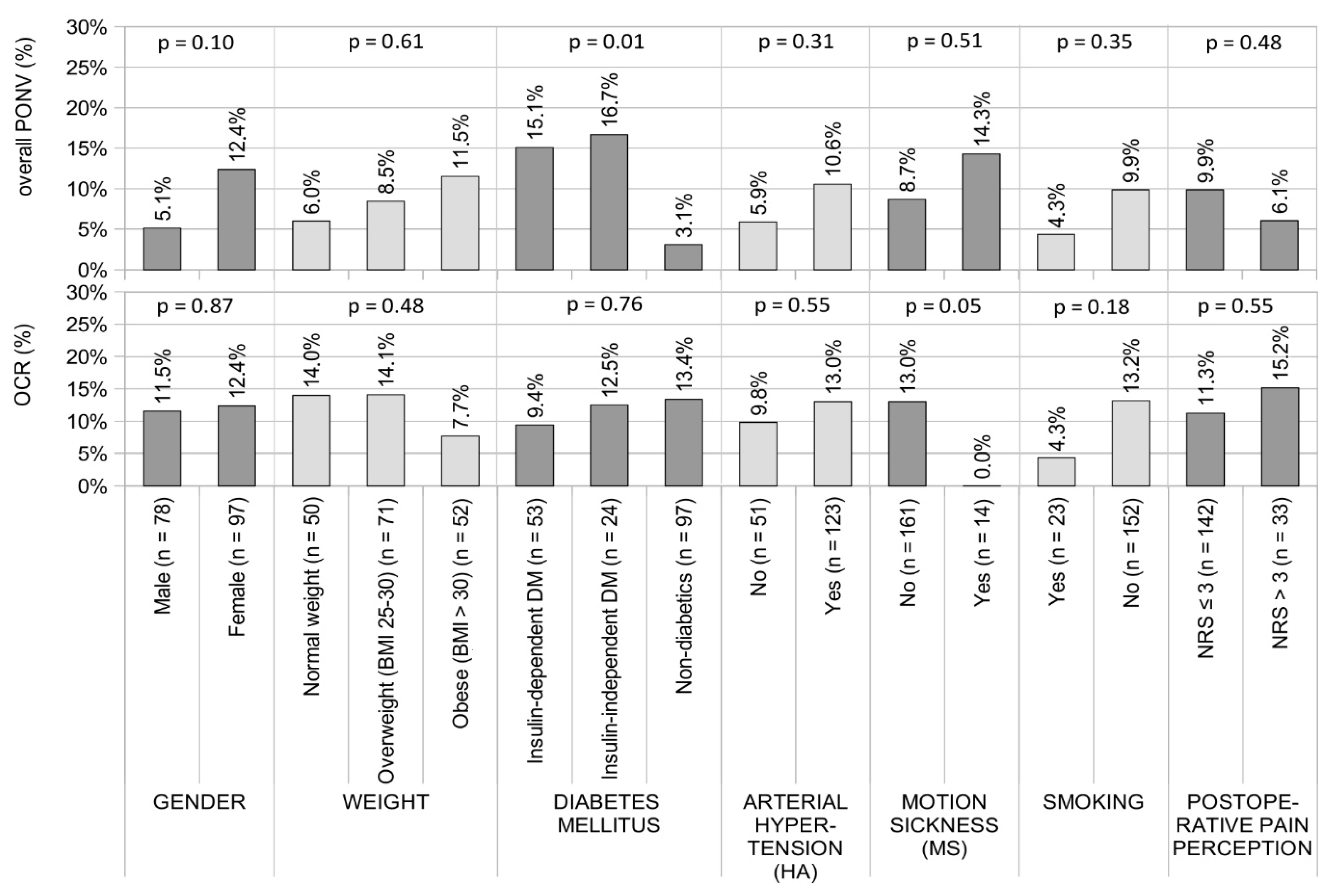
| Parameter | Gender | Weight | ||||
|---|---|---|---|---|---|---|
| Male | Female | Normal Weight | Overweight (BMI 25–30) | Obese (BMI > 30) | ||
| non-PONV | 74 (94.9) | 85 (87.6) | 47 (94) | 65 (91.5) | 46 (88.5) | |
| overall PONV | 4 (5.1) | 12 (12.4) | 3 (6) | 6 (8.5) | 6 (11.5) | |
| OR (95%CI) p-Value | ref | OR = 2.61 (0.81–8.44) p = 0.1 NS | ref | OR = 1.45 (0.34–6.08) p = 0.61 NS | OR = 2.04 (0.48–8.66) p = 0.33 NS | |
| Non-OCR | 69 (88.5) | 85 (87.6) | 43 (86) | 61 (85.9) | 48 (92.3) | |
| OCR | 9 (11.5) | 12 (12.4) | 7 (14) | 10 (14.1) | 4 (7.7) | |
| OR (95%CI) p-Value | ref | OR = 1.08 (0.43–2.72) p = 0.87 NS | ref | OR = 1.01 (0.35–2.85) p = 0.99 NS | OR = 0.51 (0.14–1.87) p = 0.31 NS | |
| Parameter | Arterial hypertension (HA) | Diabetes mellitus (DM) | ||||
| No | Yes | Insulin-dependent DM | Insulin-independent DM | Non-diabetics | ||
| non-PONV | 48 (94.1) | 110 (89.4) | 45 (84.9) | 20 (83.3) | 94 (96.9) | |
| overall PONV | 3 (5.9) | 13 (10.6) | 8 (15.1) | 4 (16.7) | 3 (3.1) | |
| OR (95%CI) p-Value | ref | OR = 1.89 (0.52–6.94) p = 0.34 NS | OR = 5.57 (1.41–22) p = 0.01 | OR = 6.27 (1.3–30.2) p = 0.02 | ref | |
| Non-OCR | 46 (90.2) | 107 (87) | 48 (90.6) | 21 (87.5) | 84 (86.6) | |
| OCR | 5 (9.8) | 16 (13) | 5 (9.4) | 3 (12.5) | 13 (13.4) | |
| OR (95%CI) p-Value | ref | OR = 1.38 (0.48–3.98) p = 0.56 NS | OR = 0.67 (0.23–2) p = 0.48 NS | OR = 0.92 (0.24–3.54) p = 0.91 NS | ref | |
| Parameter | Motion sickness (MS) | Smoking | ||||
| No | Yes | No | Yes | |||
| non-PONV | 147 (91.3) | 12 (85.7) | 137 (90.1) | 22 (95.7) | ||
| overall PONV | 14 (8.7) | 2 (14.3) | 15 (9.9) | 1 (4.3) | ||
| OR (95%CI) p-Value | ref | OR = 1.75 (0.36–8.62) p = 0.49 NS | ref | OR = 0.42 (0.05–3.3) p = 0.41 NS | ||
| Non-OCR | 140 (87) | 14 (100) | 22 (95.7) | 132 (86.8) | ||
| OCR | 21 (13) | 0 (0) | 1 (4.3) | 20 (13.2) | ||
| OR (95%CI) p-Value | ref | - | ref | OR = 0.3 (0.04–2.35) p = 0.25 NS | ||
| Parameter | Fluid challenge (mL) | Postoperative pain perception | ||||
| NRS ≤ 3 | NRS > 3 | |||||
| non-PONV | 996.8 + 312.2 1000 (360) | 128 (90.1) | 31 (93.9) | |||
| overall PONV | 940 + 211.5 1000 (250) | 14 (9.9) | 2 (6.1) | |||
| OR (95%CI) p-Value | OR = 0.99 (0.998–1.001) p = 0.49 NS | ref | OR = 0.59 (0.13–2.73) p = 0.49 NS | |||
| non-OCR | 978.8 + 287.8 1000 (350) | 126 (88.7) | 28 (84.8) | |||
| OCR | 1083.3 + 400.1 1000 (450) | 16 (11.3) | 5 (15.2) | |||
| OR (95%CI) p-Value | OR = 1.001 (0.999–1.003) p = 0.14 NS | ref | OR = 1.41 (0.48–4.16) p = 0.53 NS | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stasiowski, M.J.; Pluta, A.; Lyssek-Boroń, A.; Król, S.; Krawczyk, L.; Niewiadomska, E.; Żak, J.; Kawka, M.; Dobrowolski, D.; Grabarek, B.O.; et al. Adverse Events during Vitreoretinal Surgery under Adequacy of Anesthesia Guidance—Risk Factor Analysis. Pharmaceuticals 2022, 15, 237. https://doi.org/10.3390/ph15020237
Stasiowski MJ, Pluta A, Lyssek-Boroń A, Król S, Krawczyk L, Niewiadomska E, Żak J, Kawka M, Dobrowolski D, Grabarek BO, et al. Adverse Events during Vitreoretinal Surgery under Adequacy of Anesthesia Guidance—Risk Factor Analysis. Pharmaceuticals. 2022; 15(2):237. https://doi.org/10.3390/ph15020237
Chicago/Turabian StyleStasiowski, Michał Jan, Aleksandra Pluta, Anita Lyssek-Boroń, Seweryn Król, Lech Krawczyk, Ewa Niewiadomska, Jakub Żak, Magdalena Kawka, Dariusz Dobrowolski, Beniamin Oskar Grabarek, and et al. 2022. "Adverse Events during Vitreoretinal Surgery under Adequacy of Anesthesia Guidance—Risk Factor Analysis" Pharmaceuticals 15, no. 2: 237. https://doi.org/10.3390/ph15020237