

Excessive Oxygen Administration in High-Risk Patients Admitted to Medical and Surgical Wards Monitored by Wireless Pulse Oximeter

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting and Participants
2.3. Monitoring
2.4. Data and Variables
2.5. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bitterman, H. Bench-to-bedside review: Oxygen as a drug. Crit. Care 2009, 13, 205. [Google Scholar] [CrossRef]
- Meyhoff, C.S.; Jorgensen, L.N.; Wetterslev, J.; Christensen, K.B.; Rasmussen, L.S. Increased long-term mortality after a high perioperative inspiratory oxygen fraction during abdominal surgery: Follow-up of a randomized clinical trial. Anesth. Analg. 2012, 115, 849–854. [Google Scholar] [CrossRef]
- Damiani, E.; Donati, A.; Girardis, M. Oxygen in the critically ill: Friend or foe? Curr. Opin. Anaesthesiol. 2018, 31, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Boom, W.v.D.; Hoy, M.; Sankaran, J.; Liu, M.; Chahed, H.; Feng, M.; See, K.C. The Search for Optimal Oxygen Saturation Targets in Critically III Patients: Observational Data from Large ICU Databases. Chest 2020, 157, 566–573. [Google Scholar] [CrossRef] [PubMed]
- O’Driscoll, B.R.; Smith, R. Oxygen Use in Critical Illness. Respir. Care 2019, 64, 1293–1307. [Google Scholar] [CrossRef] [PubMed]
- Helmerhorst, H.J.F.; Schultz, M.J.; van der Voort, P.H.J.; de Jonge, E.; van Westerloo, D.J. Bench-to-bedside review: The effects of hyperoxia during critical illness. Crit. Care 2015, 19, 284. [Google Scholar] [CrossRef]
- Farquhar, H.; Weatherall, M.; Wijesinghe, M.; Perrin, K.; Ranchord, A.; Simmonds, M.; Beasley, R. Systematic review of studies of the effect of hyperoxia on coronary blood flow. Am. Hear. J. 2009, 158, 371–377. [Google Scholar] [CrossRef] [PubMed]
- O’Driscoll, B.R.; Howard, L.S.; Earis, J.; Mak, V. BTS guideline for oxygen use in adults in healthcare and emergency settings. Thorax 2017, 72 (Suppl. S1), ii1–ii90. [Google Scholar] [CrossRef] [PubMed]
- Troensegaard, H.; Petersen, C.; Pedersen, N.E.; Petersen, T.S.; Meyhoff, C.S. Variable oxygen administration in surgical and medical wards evaluated by 30-day mortality—An observational study. Acta Anaesthesiol. Scand. 2021, 65, 952–958. [Google Scholar] [CrossRef]
- Allegranzi, B.; Zayed, B.; Bischoff, P.; Kubilay, N.Z.; de Jonge, S.; de Vries, F.; Gomes, S.M.; Gans, S.; Wallert, E.D.; Wu, X.; et al. New WHO recommendations on intraoperative and postoperative measures for surgical site infection prevention: An evidence-based global perspective. Lancet Infect. Dis. 2016, 16, e288–e303. [Google Scholar] [CrossRef]
- Elvekjaer, M.; for the WARD-Project Group; Aasvang, E.K.; Olsen, R.M.; Sørensen, H.B.D.; Porsbjerg, C.M.; Jensen, J.-U.; Haahr-Raunkjær, C.; Meyhoff, C.S. Physiological abnormalities in patients admitted with acute exacerbation of COPD: An observational study with continuous monitoring. J. Clin. Monit. Comput. 2020, 34, 1051–1060. [Google Scholar] [CrossRef]
- Haahr-Raunkjaer, C.; Haahr-Raunkjaer, C.; Mølgaard, J.; Mølgaard, J.; Elvekjaer, M.; Elvekjaer, M.; Rasmussen, S.M.; Rasmussen, S.M.; Achiam, M.P.; Achiam, M.P.; et al. Continuous monitoring of vital sign abnormalities; association to clinical complications in 500 postoperative patients. Acta Anaesthesiol. Scand. 2022, 66, 552–562. [Google Scholar] [CrossRef]
- Wijesinghe, M.; Perrin, K.; Ranchord, A.; Simmonds, M.; Weatherall, M.; Beasley, R. Routine use of oxygen in the treatment of myocardial infarction: Systematic review. Heart 2009, 95, 198–202. [Google Scholar] [CrossRef]
- Shuvy, M.; Atar, D.; Steg, P.G.; Halvorsen, S.; Jolly, S.; Yusuf, S.; Lotan, C. Oxygen therapy in acute coronary syndrome: Are the benefits worth the risk? Eur. Hear. J. 2013, 34, 1630–1635. [Google Scholar] [CrossRef]
- Smith, M.E.B.; Chiovaro, J.C.; O’neil, M.; Kansagara, D.; Quiñones, A.R.; Freeman, M.; Motu’apuaka, M.L.; Slatore, C.G. Early Warning System Scores for Clinical Deterioration in Hospitalized Patients: A Systematic Review. Ann. Am. Thorac. Soc. 2014, 11, 1454–1465. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Ich Topic e 2 a Clinical Safety Data Management: Definitions and Standards for Expedited Reporting Step 5 Note for Guidance on Clinical Safety Data Management: Definitions and Standards for Expedited Reporting. 1995. Available online: http://www.ema.europa.eu (accessed on 8 December 2023).
- McIlroy, D.R.; Shotwell, M.S.; Lopez, M.G.; Vaughn, M.T.; Olsen, J.S.; Hennessy, C.; Wanderer, J.P.; Semler, M.S.; Rice, T.W.; Kheterpal, S.; et al. Oxygen administration during surgery and postoperative organ injury: Observational cohort study. BMJ 2022, 379, e070941. [Google Scholar] [CrossRef] [PubMed]
- Girardis, M.; Busani, S.; Damiani, E.; Donati, A.; Rinaldi, L.; Marudi, A.; Morelli, A.; Antonelli, M.; Singer, M. Effect of conservative vs conventional oxygen therapy on mortality among patients in an intensive care unit the oxygen-icu randomized clinical trial. JAMA J. Am. Med. Assoc. 2016, 316, 1583–1589. [Google Scholar] [CrossRef] [PubMed]
- Petersen, J.A.; Mackel, R.; Antonsen, K.; Rasmussen, L.S. Serious adverse events in a hospital using early warning score—What went wrong? Resuscitation 2014, 85, 1699–1703. [Google Scholar] [CrossRef] [PubMed]
- Fonnes, S.; Gögenur, I.; Søndergaard, E.S.; Siersma, V.D.; Jorgensen, L.N.; Wetterslev, J.; Meyhoff, C.S. Perioperative hyperoxia —Long-term impact on cardiovascular complications after abdominal surgery, a post hoc analysis of the PROXI trial. Int. J. Cardiol. 2016, 215, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Restrepo, M.I.; Sibila, O.; Anzueto, A. Pneumonia in patients with chronic obstructive pulmonary disease. Tuberc. Respir. Dis. (Seoul) 2018, 81, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Pahal, P.; Hashmi, M.F.; Sharma, S. Chronic Obstructive Pulmonary Disease Compensatory Measures; StatPearls: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK525962/ (accessed on 8 December 2023).
- Austin, M.A.; Wills, K.E.; Blizzard, L.; Walters, E.H.; Wood-Baker, R. Effect of high flow oxygen on mortality in chronic obstructive pulmonary disease patients in prehospital setting: Randomised controlled trial. BMJ 2010, 341, 927. [Google Scholar] [CrossRef] [PubMed]
- Jeffs, E.; Vollam, S.; Young, J.D.; Horsington, L.; Lynch, B.; Watkinson, P.J. Wearable monitors for patients following discharge from an intensive care unit: Practical lessons learnt from an observational study. J. Adv. Nurs. 2016, 72, 1851–1862. [Google Scholar] [CrossRef] [PubMed]
- Jensen, L.A.; Onyskiw, J.E.; Prasad, N. Meta-analysis of arterial oxygen saturation monitoring by pulse oximetry in adults. Hear. Lung 1998, 27, 387–408. [Google Scholar] [CrossRef] [PubMed]
- Songthawornpong, N.; Vijayakumar, T.; Jensen MS, V.; Elvekjaer, M.; Sørensen, H.B.; Aasvang, E.K.; Eriksen, V.R. Abstrat Continuous Monitoring of Vital Signs After Hospital Discharge: A Feasibility Study. Patient Saf. 2023, 5, 53–63. [Google Scholar]


{kind=link}
| Definition of Excessive Oxygen Administration | Cumulative Duration of Excessive Oxygen Administration | |
|---|---|---|
| No COPD diagnosis and BMI < 40 | SpO2 ≥ 99% with simultaneous supplemental oxygen therapy | 1–59 min ≥60 min |
| COPD or BMI ≥ 40 | SpO2 ≥ 93% with simultaneous supplemental oxygen therapy | 1–59 min |
| ≥60 min |
| Group 1 No EOA (N = 358) | Group 2 EOA 1–59 min (N = 146) | Group 3 EOA ≥ 60 min (N = 63) | |
|---|---|---|---|
| Age (yr) | 71 [60–85] | 70 [62–81] | 71 [60–85] |
| Sex female, n (%) | 133 (37%) | 69 (47%) | 34 (54%) |
| Body mass index (kg/m2) | 25 [19–34] | 25 [19–35] | 25 [18–36] |
| Inclusion diagnosis, n (%) | |||
| Acute exacerbation of COPD | 46 (13%) | 17 (12%) | 40 (63%) |
| Major abdominal surgery | 312 (87%) | 129 (88%) | 23 (37%) |
| Comorbidities, n (%) | |||
| Cerebral disease | 34 (9%) | 11 (8%) | 11 (17%) |
| Cardiac disease | 76 (21%) | 22 (15%) | 11 (17%) |
| COPD | 88 (25%) | 30 (21%) | 41 (65%) |
| Diabetes | 58 (16%) | 25 (17%) | 12 (19%) |
| Metastasis | 16 (4%) | 7 (5%) | 3 (5%) |
| Smoking status, n (%) | |||
| Current smoker | 56 (16%) | 28 (19%) | 14 (22%) |
| Previous smoker | 196 (55%) | 82 (56%) | 37 (59%) |
| Never smoked | 106 (30%) | 36 (25%) | 12 (19%) |
| FEV1/FVC, % | 72 [42–87] | 71 [42–90] | 57 [37–83] |
| GOLD, n (%) | |||
| GOLD I | 3 (0.8%) | 0 | 2 (3.2%) |
| GOLD II | 16 (4.5%) | 3 (2.1%) | 13 (21%) |
| GOLD III | 12 (3.4%) | 7 (4.8%) | 20 (32%) |
| GOLD IV | 9 (2.5%) | 6 (4.1%) | 4 (6.4%) |
| Medical History (Charlson Comorbidity Index), n (%) | |||
| CCI score: 2–3 | 49 (14%) | 14 (10%) | 9 (14%) |
| CCI score: 4–5 | 189 (53%) | 78 (53%) | 24 (38%) |
| CCI score: 6–7 | 78 (22%) | 40 (27%) | 18 (29%) |
| CCI score: 8+ | 32 (9%) | 13 (9%) | 8 (13%) |
| American Society of Anesthesiologists class, n (%) | |||
| I | 18 (5%) | 1 (0.7%) | 1 (1.6%) |
| II | 168 (47%) | 65 (45%) | 10 (16%) |
| III | 119 (33%) | 61 (42%) | 12 (19%) |
| IV | 2 (0.6%) | 2 (1.4%) | 0 |
| Baseline SpO2 (%) | 96 [92–100] | 98 [91–100] | 96 [92–100] |
| Baseline O2 supply, L/min | 2 [0–3] | 2 [0–4] | 2 [0–3] |
| Location of surgery, n (%) | |||
| Esophagus | 57 (16%) | 24 (16%) | 4 (6.4%) |
| Gastric | 40 (11%) | 17 (12%) | 3 (4.8%) |
| Pancreas | 114 (32%) | 42 (29%) | 7 (11%) |
| Intestines | 17 (4.8%) | 2 (1.4%) | 3 (4.8%) |
| Colorectal | 100 (28%) | 42 (29%) | 27 (43%) |
| Other | 12 (3.6%) | 10 (6.9%) | 2 (3.2%) |
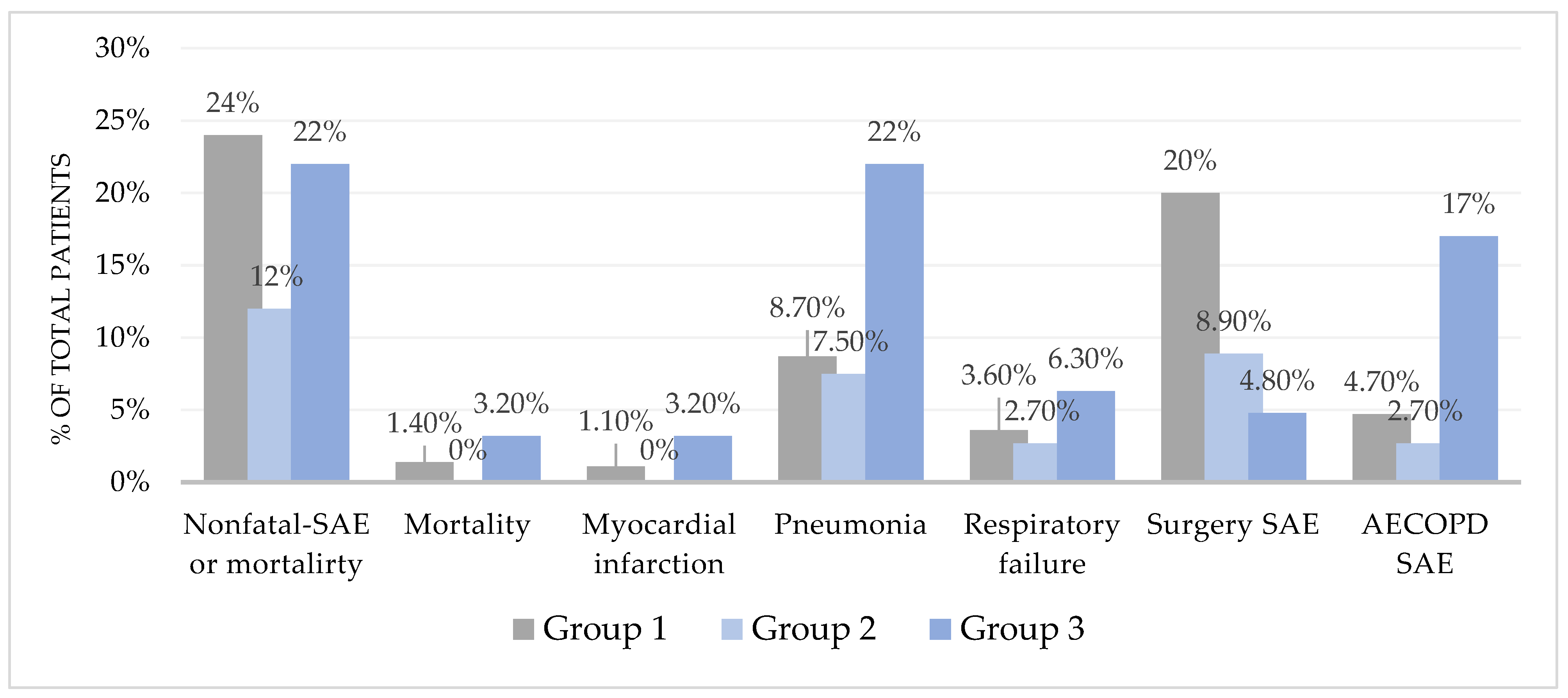
| Group 1 No EOA (N = 358) | Group 2 EOA 1–59 min (N = 146) | Group 3 EOA ≥ 60 min (N = 63) | Adjusted OR | 95% CI | p-Value | |
|---|---|---|---|---|---|---|
| Nonfatal SAE or mortality | 87 (24%) | 17 (12%) | 14 (22%) | 0.98 | [0.96–1.01] | 0.24 |
| Mortality | 5 (1.4%) | 0 | 2 (3.2%) | 1.00 | [0.94–1.07] | 0.98 |
| Myocardial injury or infarction | 4 (1.1%) | 0 | 2 (3.2%) | 1.00 | [0.95–1.08] | 0.80 |
| Pneumonia | 31 (8.7%) | 11 (7.5%) | 14 (22%) | 1.00 | [0.98–1.03] | 0.70 |
| Respiratory failure | 13 (3.6%) | 4 (2.7%) | 4 (6.3%) | 0.99 | [0.95–1.04] | 0.77 |
| Receiving NIV treatment | 5 (1.4%) | 3 (2%) | 2 (3.2%) | 0.99 | [0.93–1.07] | 0.97 |
| Receiving invasive mechanical ventilation | 7 (2%) | 1 (0.7%) | 1 (1.6%) | 0.99 | [0.93–1.06] | 0.78 |
| Subgroup analysis | ||||||
| SAE in surgical patients (N = 464) | 70 (22%) | 13 (10%) | 3 (13%) | 0.97 | [0.88–1.06] | 0.50 |
| SAE in patients with AECOPD (N = 103) | 17 (37%) | 4 (24%) | 11 (28%) | 0.98 | [0.96–1.02] | 0.35 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mathar, C.E.; Haahr-Raunkjær, C.; Elvekjær, M.; Gu, Y.; Holm, C.P.; Achiam, M.P.; Jorgensen, L.N.; Aasvang, E.K.; Meyhoff, C.S. Excessive Oxygen Administration in High-Risk Patients Admitted to Medical and Surgical Wards Monitored by Wireless Pulse Oximeter. Sensors 2024, 24, 1139. https://doi.org/10.3390/s24041139
Mathar CE, Haahr-Raunkjær C, Elvekjær M, Gu Y, Holm CP, Achiam MP, Jorgensen LN, Aasvang EK, Meyhoff CS. Excessive Oxygen Administration in High-Risk Patients Admitted to Medical and Surgical Wards Monitored by Wireless Pulse Oximeter. Sensors. 2024; 24(4):1139. https://doi.org/10.3390/s24041139
Chicago/Turabian StyleMathar, Clara E., Camilla Haahr-Raunkjær, Mikkel Elvekjær, Ying Gu, Claire P. Holm, Michael P. Achiam, Lars N. Jorgensen, Eske K. Aasvang, and Christian S. Meyhoff. 2024. "Excessive Oxygen Administration in High-Risk Patients Admitted to Medical and Surgical Wards Monitored by Wireless Pulse Oximeter" Sensors 24, no. 4: 1139. https://doi.org/10.3390/s24041139