Author Contributions
Conceptualization, P.S. and A.W.; methodology, P.S., A.W. and P.H.; formal analysis, P.S.; investigation, P.H., G.I. and A.P.; resources, J.A. and A.R.; writing—original draft preparation, P.S.; writing—review and editing, P.S., A.W., P.H., G.I., J.A., A.R., A.W.L. and A.P.; visualization, P.S.; funding acquisition, A.W.L., G.I. and A.P. All authors have read and agreed to the published version of the manuscript.
Figure 1.
The forward velocity and acceleration of the center of mass during a single gait cycle. The peak-to-peak distance of velocity and acceleration is equivalent to one step length. Illustration based on speed profile and gait descriptions is given in [
24,
25].
Figure 1.
The forward velocity and acceleration of the center of mass during a single gait cycle. The peak-to-peak distance of velocity and acceleration is equivalent to one step length. Illustration based on speed profile and gait descriptions is given in [
24,
25].
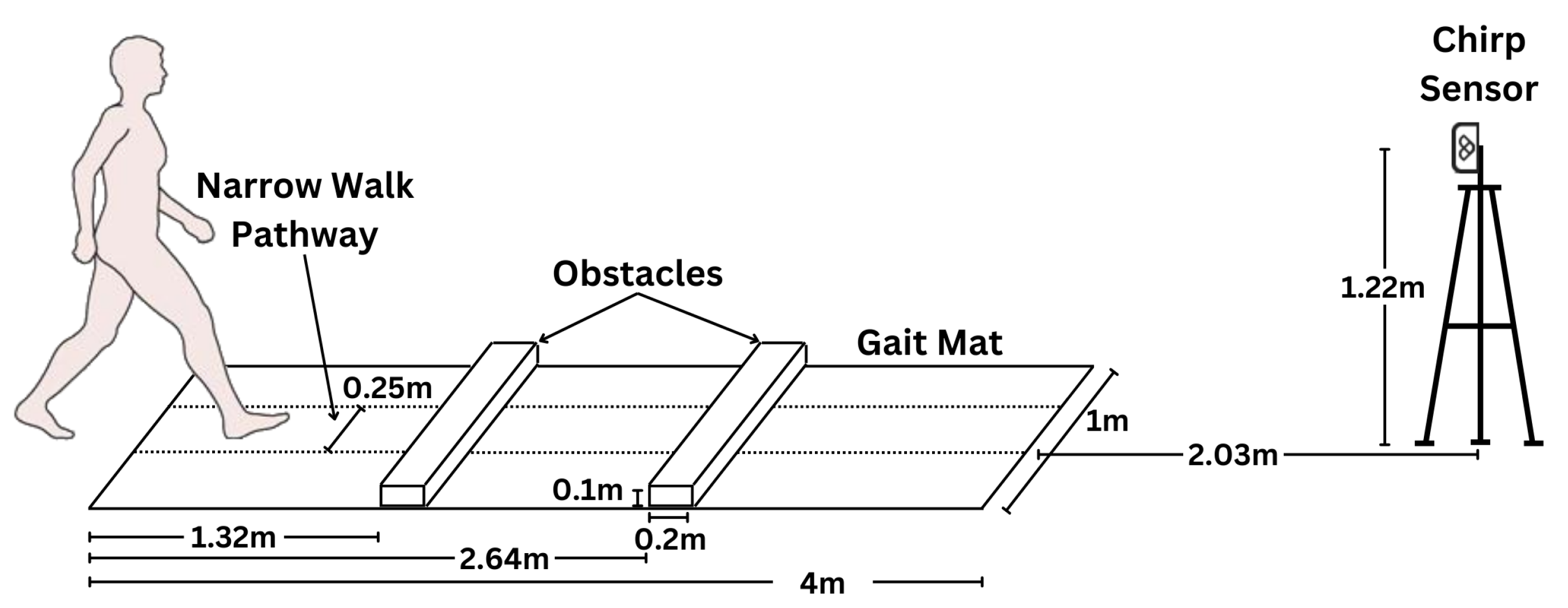
Figure 2.
In-clinic setup of the 4 m ProtoKinetics Zeno Walkway Gait Analysis System and Chirp Smart Home Sensor for testing concurrent validity of step length measurement. Obstacles are only used for obstacle walks. Narrow walk pathway is used for narrow walking scenario only.
Figure 2.
In-clinic setup of the 4 m ProtoKinetics Zeno Walkway Gait Analysis System and Chirp Smart Home Sensor for testing concurrent validity of step length measurement. Obstacles are only used for obstacle walks. Narrow walk pathway is used for narrow walking scenario only.
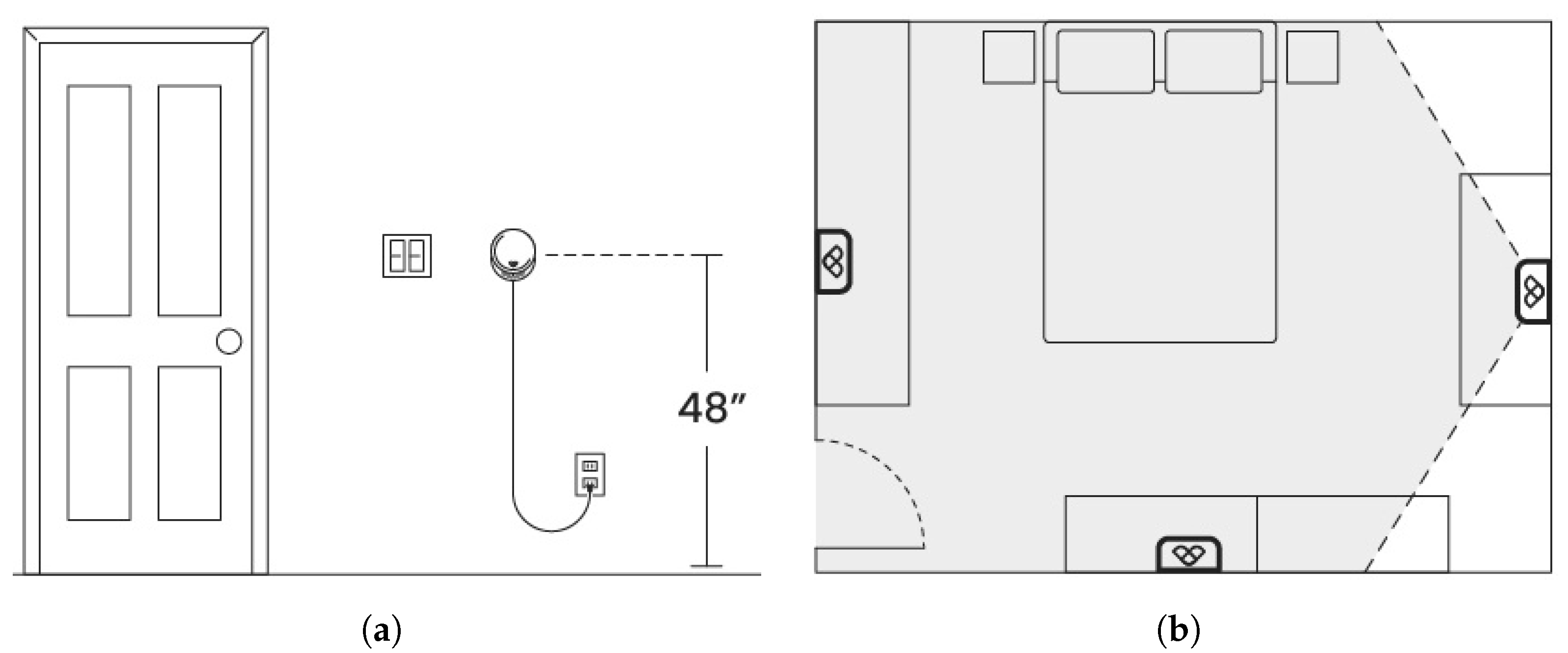
Figure 3.
Placement of Chirp sensor in the room. (a) Elevation at switch height. (b) Possible locations of the Chirp sensor at center of wall covering entire room.
Figure 3.
Placement of Chirp sensor in the room. (a) Elevation at switch height. (b) Possible locations of the Chirp sensor at center of wall covering entire room.
Figure 4.
Step length measurement methodology: Radar signal processing generates 3D point clouds with speeds, enabling detection and tracking of individuals. In the home, linear track segments along the radar’s radial axis are isolated, while in the clinic, track segments along Zeno Walkway’s linear path are extracted. Step length is determined as the peak-to-peak distance of torso speed. The contributions of this paper are highlighted by the dashed rectangle (cyan).
Figure 4.
Step length measurement methodology: Radar signal processing generates 3D point clouds with speeds, enabling detection and tracking of individuals. In the home, linear track segments along the radar’s radial axis are isolated, while in the clinic, track segments along Zeno Walkway’s linear path are extracted. Step length is determined as the peak-to-peak distance of torso speed. The contributions of this paper are highlighted by the dashed rectangle (cyan).
Figure 5.
Tracking illustration: Radar point clouds are clustered to form detections, which are associated to tracks through the Hungarian algorithm and tracked using Kalman filtering. The floor is depicted with a 1 m by 1 m checkerboard pattern, while Zeno Walkway is represented by a cyan rectangle. The blue rectangular prism represents observations of people or tracked location of people.
Figure 5.
Tracking illustration: Radar point clouds are clustered to form detections, which are associated to tracks through the Hungarian algorithm and tracked using Kalman filtering. The floor is depicted with a 1 m by 1 m checkerboard pattern, while Zeno Walkway is represented by a cyan rectangle. The blue rectangular prism represents observations of people or tracked location of people.
Figure 6.
Track is segmented into linear track segments using the Ramer–Douglas–Peucker algorithm. m for this figure. The segments of track corresponding to , , , and are indicated by the colors magenta, red, blue and cyan respectively.
Figure 6.
Track is segmented into linear track segments using the Ramer–Douglas–Peucker algorithm. m for this figure. The segments of track corresponding to , , , and are indicated by the colors magenta, red, blue and cyan respectively.
Figure 7.
Linear track segment has a length (10) and an orientation (11) that is needed to orient the track along radar’s radial axis.
Figure 7.
Linear track segment has a length (10) and an orientation (11) that is needed to orient the track along radar’s radial axis.
Figure 8.
Control (normal speed) walk by a participant: On the left, the tracked location overlaid with the expected location of the Zeno Walkway. On the right, the Doppler torso speed, featuring detected torso speed spikes. Notably, the speed trend is non-constant due to the acceleration and deceleration effects of starting and stopping.
Figure 8.
Control (normal speed) walk by a participant: On the left, the tracked location overlaid with the expected location of the Zeno Walkway. On the right, the Doppler torso speed, featuring detected torso speed spikes. Notably, the speed trend is non-constant due to the acceleration and deceleration effects of starting and stopping.
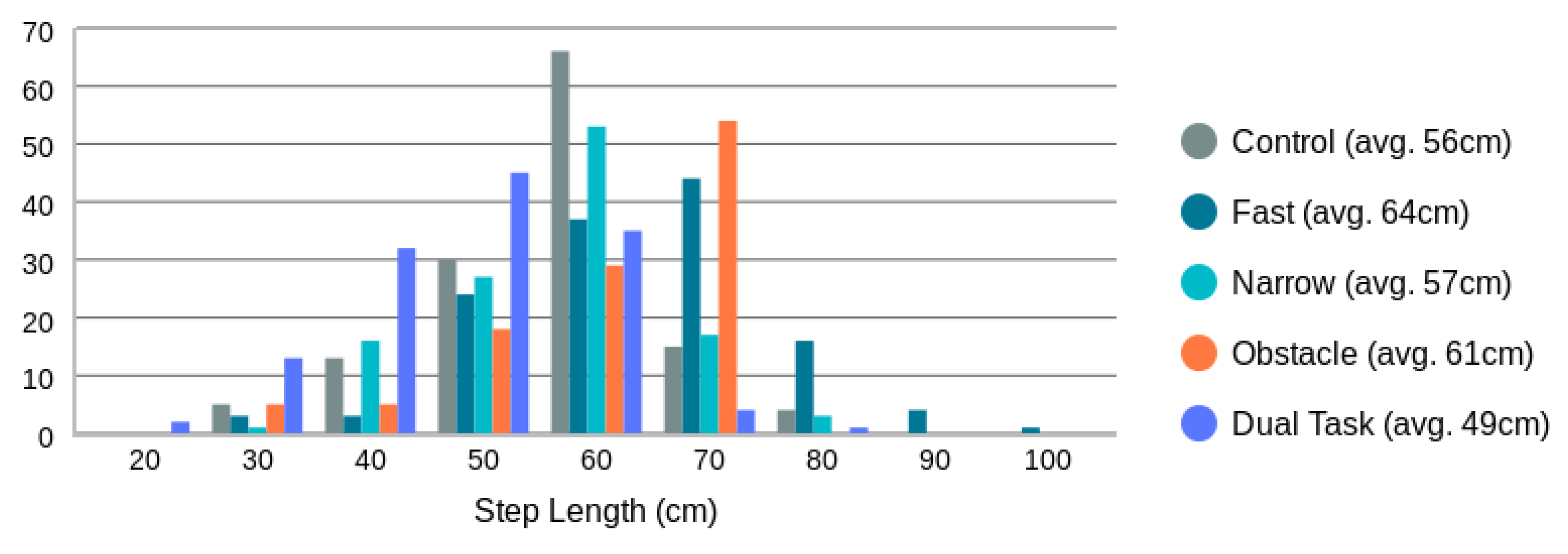
Figure 9.
Ground truth step length distribution as measured by the Zeno Walkway Gait Analysis System. Overall average step length is 57 cm (12 cm).
Figure 9.
Ground truth step length distribution as measured by the Zeno Walkway Gait Analysis System. Overall average step length is 57 cm (12 cm).
Figure 10.
Distribution of step times as measured by torso speed peak-to-peak times.
Figure 10.
Distribution of step times as measured by torso speed peak-to-peak times.
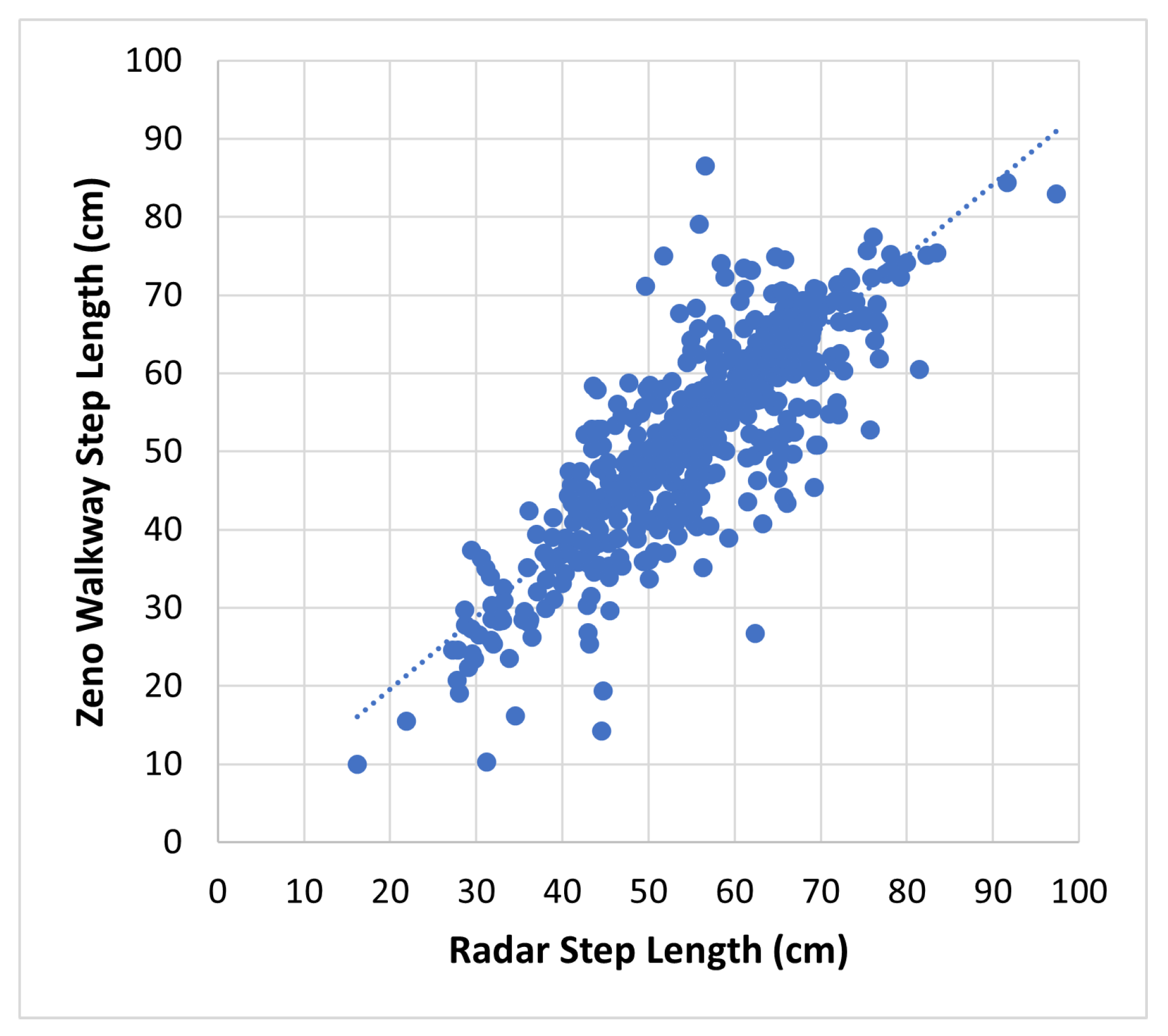
Figure 11.
Proposed radar-based step length measurement vs. Zeno Walkway. Data include all 599 walks (4 m each) by 35 frail older adults.
Figure 11.
Proposed radar-based step length measurement vs. Zeno Walkway. Data include all 599 walks (4 m each) by 35 frail older adults.
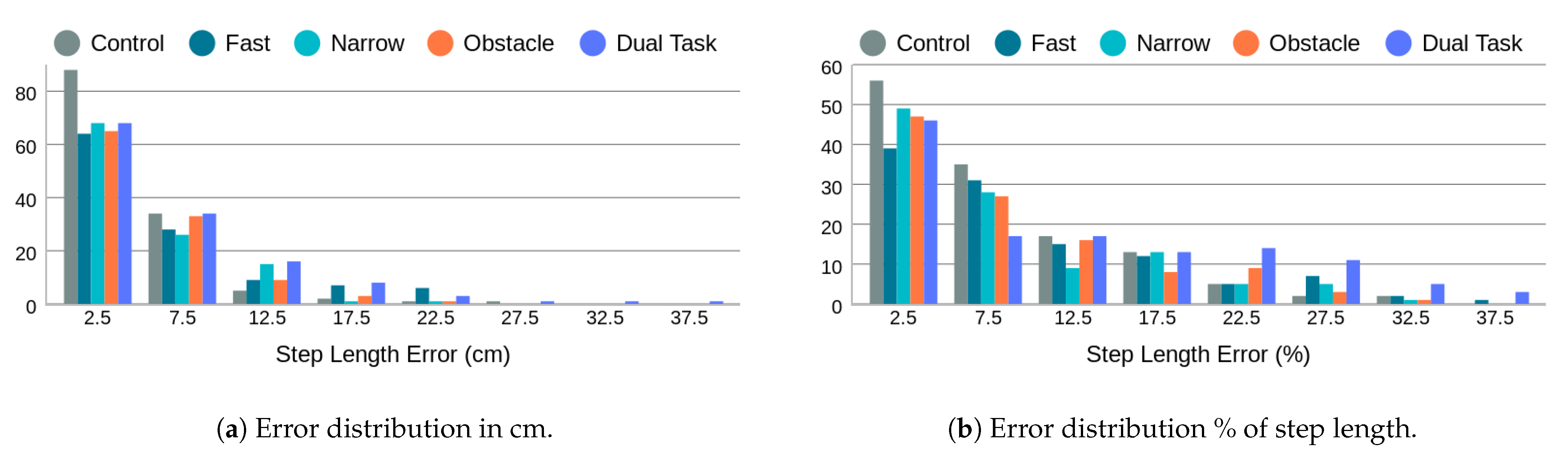
Figure 12.
Step length error distribution by walk type in cm and as a percentage of the true step length measured by Zeno Walkway.
Figure 12.
Step length error distribution by walk type in cm and as a percentage of the true step length measured by Zeno Walkway.
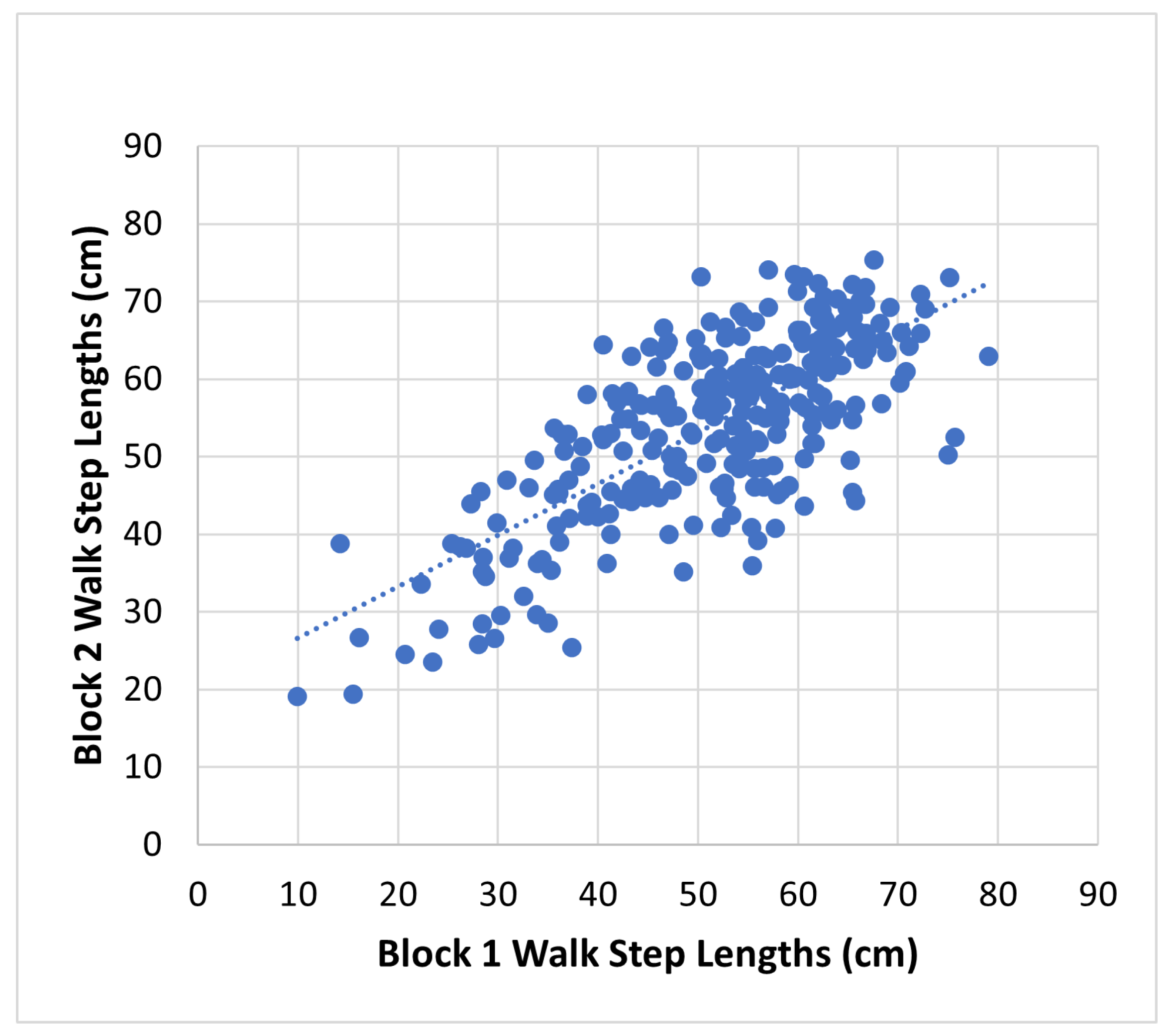
Figure 13.
Intra-session reliability. Block 1 to block 2 step lengths measured in the clinic. ICC(2,k) = 0.83 (95% CI 0.77 to 0.87).
Figure 13.
Intra-session reliability. Block 1 to block 2 step lengths measured in the clinic. ICC(2,k) = 0.83 (95% CI 0.77 to 0.87).
Figure 14.
Average step length measurement, obtained by the proposed method, between week 1 and week 2 for each room. ICC(2,k) = 0.91 (95% CI 0.82 to 0.96), indicates excellent reliability.
Figure 14.
Average step length measurement, obtained by the proposed method, between week 1 and week 2 for each room. ICC(2,k) = 0.91 (95% CI 0.82 to 0.96), indicates excellent reliability.
Figure 15.
Test–retest reliability of in-home step length as a function of aggregation interval. Reliability is measured using inter-class correlation (ICC).
Figure 15.
Test–retest reliability of in-home step length as a function of aggregation interval. Reliability is measured using inter-class correlation (ICC).
Figure 16.
In-home average radar step length compared to in-clinic average control (normal walk) step length measured by Zeno Walkway. ICC(3,k) = 0.81 (95% CI 0.53 to 0.92), indicates strong consistency.
Figure 16.
In-home average radar step length compared to in-clinic average control (normal walk) step length measured by Zeno Walkway. ICC(3,k) = 0.81 (95% CI 0.53 to 0.92), indicates strong consistency.
Figure 17.
Distribution of all step lengths measured in the home over the full two-week data collection period.
Figure 17.
Distribution of all step lengths measured in the home over the full two-week data collection period.
Figure 18.
Percentage of valid linear track segments where step length can be measured. Valid linear track segments are linear track segments that are at least 2 m in length and within of radar’s radial axis direction.
Figure 18.
Percentage of valid linear track segments where step length can be measured. Valid linear track segments are linear track segments that are at least 2 m in length and within of radar’s radial axis direction.
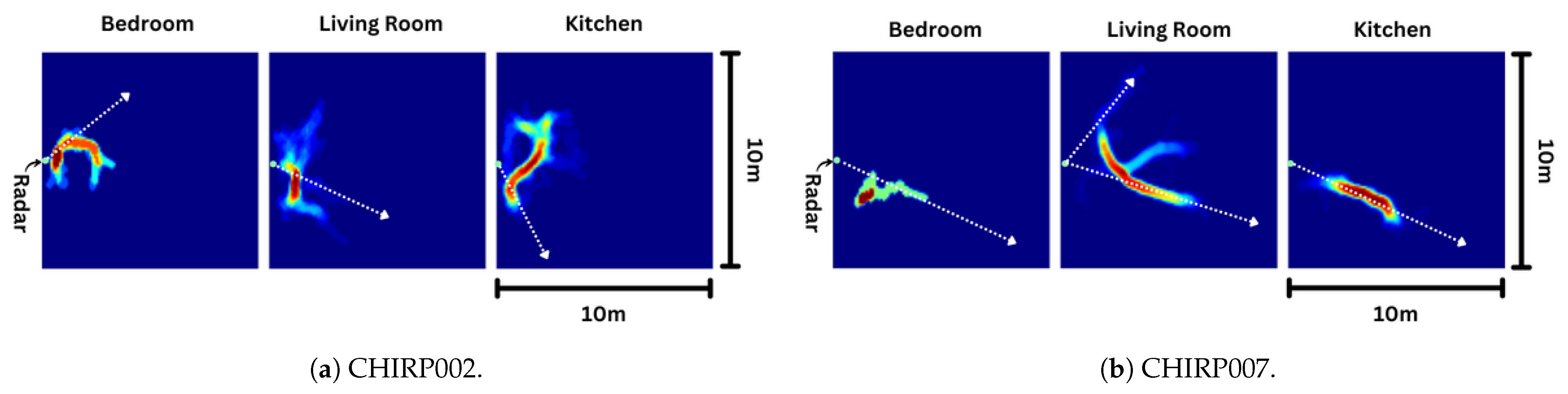
Figure 19.
Heatmap of tracks in each room outlines the commonly used pathways in the home. CHIRP007’s home has many commonly used pathways that lines up with radar’s radial axis (illustrated in white dotted lines). CHIRP002’s home’s commonly used pathways do not line up with radar’s radial axis.
Figure 19.
Heatmap of tracks in each room outlines the commonly used pathways in the home. CHIRP007’s home has many commonly used pathways that lines up with radar’s radial axis (illustrated in white dotted lines). CHIRP002’s home’s commonly used pathways do not line up with radar’s radial axis.
Table 1.
Existing radar-based step length measurement techniques using trunk movement.
Table 1.
Existing radar-based step length measurement techniques using trunk movement.
| Method | Distance (m) | No. of Participants | Participants | Ground Truth |
|---|
| [21] | 4 | 3 | Young adults | Marker attached to shoe |
| [22] | 25.2 † | 4 | Young adults | Fixed 70 cm steps |
| [18] | 56 ‡ | 5 | Young adults | Fixed 70 cm steps |
| [23] | 10 | 10 | Young adults | MOCAP |
Table 2.
Demographics of the participants. M—mean, SD—standard deviation, SPPB—Short Physical Performance Battery, FES—Fall Efficacy Scale, and MoCA—Montreal Cognitive Assessment.
Table 2.
Demographics of the participants. M—mean, SD—standard deviation, SPPB—Short Physical Performance Battery, FES—Fall Efficacy Scale, and MoCA—Montreal Cognitive Assessment.
| Demographics | All Participants (N = 35) |
|---|
| Age, M (SD) | 75.49 (6.56) |
| Age, Range | 60 to 89 |
| Sex, % female | 30/35 (85.71%) |
| Education, n more than high school | 23/35 (65.71%) |
| Living arrangement, n lives alone | 35/35 (100%) |
| Physical function, SPPB total score, M (SD) | 8.53 (2.74) |
| Physical function, n SPPB < 9 | 12/34 (35.29%) |
| Fear of falling, FES-I total score, M (SD) | 24.97 (6.62) |
| Fear of falling, n FES-I moderate to high severity | 26/34 (76.47%) |
| Cognition, MoCA total score, M (SD) | 23.38 (3.64) |
| Cognition, n MoCA total score < 25 | 20/34 (58.82%) |
Table 3.
Of the 700 walks (35 participant × 20 walks), data are missed due to technical difficulties and participants unable to complete the walks due to frailty.
Table 3.
Of the 700 walks (35 participant × 20 walks), data are missed due to technical difficulties and participants unable to complete the walks due to frailty.
| | Control | Fast | Narrow | Obstacle | Dual Task | All |
|---|
| Tech. Difficulty | 6 | 4 | 6 | 5 | 7 | 28 (4.0%) |
| Unable | 1 | 4 | 17 | 24 | 1 | 47 (6.7%) |
| Collected Walks | 133 | 132 | 117 | 111 | 132 | 625 (89.3%) |
Table 4.
Step length detection rates for the proposed approach on the 625 walks.
Table 4.
Step length detection rates for the proposed approach on the 625 walks.
| | Control | Fast | Narrow | Obstacle | Dual Task | All |
|---|
| Alg. Missed | 2 | 18 | 6 | 0 | 0 | 26/625 (4.2%) |
| Alg. Detected | 131 | 114 | 111 | 111 | 132 | 599/625 (95.8%) |
Table 5.
Average (standard deviation) error in step length in cm and percentage of Zeno Walkway step length (%).
Table 5.
Average (standard deviation) error in step length in cm and percentage of Zeno Walkway step length (%).
| | Control | Fast | Narrow | Obstacle | Dual Task | All |
|---|
| cm | 4.5 (4.3) | 6.5 (5.9) | 5.0 (4.3) | 5.0 (4.4) | 6.5 (6.4) | 5.5 (5.2) |
| % | 8.3 (8.0) | 10.4 (9.3) | 9.3 (9.2) | 8.5 (7.4) | 14.3 (13.4) | 10.2 (10.1) |
Table 6.
Comparison to existing methods for normal walking in a controlled setting.
Table 6.
Comparison to existing methods for normal walking in a controlled setting.
| Method | Avg. Error (cm) | Total No. of Walks | No. of Participants | Distance (m) | Type |
|---|
| [21] | 1.1 (0.8) | 3 | 3 | 4 | Young Fit |
| [22] | 2.3 | 4 | 4 | 25.2 | Young Fit |
| [18] | 2.6 (1.5) | 5 | 5 | 56 | Young Fit |
| [23] | 2.2 (1.4) | 100 | 10 | 10 | Young Fit |
| Ours | 4.5 (4.3) | 131 | 35 | 4 | Older Frail |

 ,
, 



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}